You might also like
- Metal Gear Solid - Characters Profile and TimelineDocument65 pagesMetal Gear Solid - Characters Profile and Timelinekrevorkian1653100% (1)
- Employee Safety Training Matrix Template ExcelDocument79 pagesEmployee Safety Training Matrix Template Excelشاز إياسNo ratings yet
- Passenger Elevator Operation ManualDocument24 pagesPassenger Elevator Operation ManualJahn Ray B. Lanozo100% (1)
- Strategy Implementation, Evaluation and ControlDocument6 pagesStrategy Implementation, Evaluation and Controlbonny MishNo ratings yet
- AsthmaDocument66 pagesAsthmaapi-3729824100% (4)
- v0.4.3 BomDocument1 pagev0.4.3 BomCristián Quiroz100% (1)
- Pedia 3.1 Pediatric PulmoDocument8 pagesPedia 3.1 Pediatric PulmoAswanth ThisaiveeranNo ratings yet
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocument4 pagesPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Pathophysiology of AsthmaDocument10 pagesPathophysiology of AsthmaEden Mae100% (4)
- Workshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Document33 pagesWorkshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Ilie Viorel60% (5)
- Logix 5000 Controllers Tasks, Programs, and RoutinesDocument73 pagesLogix 5000 Controllers Tasks, Programs, and Routinesobi SalamNo ratings yet
- Risk For Infection - NCPDocument3 pagesRisk For Infection - NCPHamil BanagNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaMaria Cristina100% (1)
- COPD - Update Diagnosis and Management of Stable COPDDocument29 pagesCOPD - Update Diagnosis and Management of Stable COPDIwanNo ratings yet
- Refrat Asma Eksaserbasi - Dr. Retna, Sp. PDocument24 pagesRefrat Asma Eksaserbasi - Dr. Retna, Sp. PWaskito Setiaji100% (1)
- Chronic Obstructive Pulmonary Diseases (COPD) Penyakit Paru Obstruktif Kronik (PPOK)Document55 pagesChronic Obstructive Pulmonary Diseases (COPD) Penyakit Paru Obstruktif Kronik (PPOK)Yolanda Octaviana TariganNo ratings yet
- Lecture 27-Clinical Manifestation, Diagnostics and Management Approach To Obstructive Lung Disease-Dr. Sumardi, SPPD, KP (2018)Document40 pagesLecture 27-Clinical Manifestation, Diagnostics and Management Approach To Obstructive Lung Disease-Dr. Sumardi, SPPD, KP (2018)stefany huangNo ratings yet
- Wheezing in InfantDocument27 pagesWheezing in Infantgalihmd07No ratings yet
- Chronic Obstructive Pulmonary Disease Versus Bronchial AsthmaDocument5 pagesChronic Obstructive Pulmonary Disease Versus Bronchial AsthmaDon JuanNo ratings yet
- EFP - Periodontal Health and Gingival Diseases and ConditionsDocument37 pagesEFP - Periodontal Health and Gingival Diseases and ConditionsRoshan PatelNo ratings yet
- Conceptmap Oct 12Document1 pageConceptmap Oct 12Aziil LiizaNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveSherlyn KirisakiNo ratings yet
- Concept Map March 11Document1 pageConcept Map March 11Dinah Rose VitorilloNo ratings yet
- Penyakit Paru Obstruktif Kronik (PPOK) : Fakultas Kedokteran Universitas Sultan Khairun (Unkhair)Document53 pagesPenyakit Paru Obstruktif Kronik (PPOK) : Fakultas Kedokteran Universitas Sultan Khairun (Unkhair)WahyunitadotokaNo ratings yet
- What Should Every Intensivist Know About Antibiotics PDFDocument171 pagesWhat Should Every Intensivist Know About Antibiotics PDFAndreea MitranNo ratings yet
- Nursing Care Plan by MecDocument4 pagesNursing Care Plan by MecMech CayananNo ratings yet
- Lunch Symposium 2 WWA 2020-Roni Naning-AntileukotrienDocument36 pagesLunch Symposium 2 WWA 2020-Roni Naning-AntileukotriensuliyantoasaNo ratings yet
- Penyakit Paru Obstruktif Kronik (Ppok)Document32 pagesPenyakit Paru Obstruktif Kronik (Ppok)Rudy LusmiandaNo ratings yet
- Materi Dr. Darmawan B. Setyanto, Sp.A (K)Document42 pagesMateri Dr. Darmawan B. Setyanto, Sp.A (K)deddyNo ratings yet
- Streptococcus: PneumoniaeDocument12 pagesStreptococcus: PneumoniaeZeth MoturiNo ratings yet
- AthmaDocument47 pagesAthmadrthanallaNo ratings yet
- Quino LonesDocument19 pagesQuino LonesSunanda mohanNo ratings yet
- Obstructive Airway DiseasesDocument67 pagesObstructive Airway DiseasesImran Ali TunioNo ratings yet
- Pcap C Case StudyDocument21 pagesPcap C Case StudyKate PedzNo ratings yet
- Aling Juana, 42 Years Old, FemaleDocument2 pagesAling Juana, 42 Years Old, FemaleGenynne RagasaNo ratings yet
- Infectious Disorder: Prepared By: Dellero, Sarah Joy P. BSN3-DDocument19 pagesInfectious Disorder: Prepared By: Dellero, Sarah Joy P. BSN3-Dngoto88No ratings yet
- IPD. 2. DR Theo - PPOKDocument96 pagesIPD. 2. DR Theo - PPOKTheopilus Obed LayNo ratings yet
- Efficacy of Povidone-Iodine Nasal and Oral Antiseptic Preparations Against Severe Acute Respiratory Syndrome-Coronavirus 2 (Sars-Cov-2)Document5 pagesEfficacy of Povidone-Iodine Nasal and Oral Antiseptic Preparations Against Severe Acute Respiratory Syndrome-Coronavirus 2 (Sars-Cov-2)GTNo ratings yet
- Tonsilitis + Scarlet + MeningitisDocument3 pagesTonsilitis + Scarlet + Meningitisd3mooz13No ratings yet
- Covid 19 Testing GuidanceDocument2 pagesCovid 19 Testing GuidanceBernewsAdminNo ratings yet
- Bronchial Asthma: West Visayas State University Medical Center - Department of PediatricsDocument9 pagesBronchial Asthma: West Visayas State University Medical Center - Department of PediatricsPGI Miayo, StephenNo ratings yet
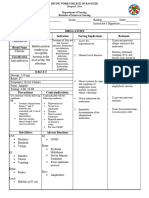
- Drugs For AsthmaDocument1 pageDrugs For Asthmakamil malikNo ratings yet
- Rle RequirementsDocument8 pagesRle RequirementsUzziel Galinea TolosaNo ratings yet
- Corona Virus - 19: A Case PresentationDocument25 pagesCorona Virus - 19: A Case PresentationYessamin Paith RoderosNo ratings yet
- CAP Pneumonia Elderly Kasus 1 (Revisi)Document39 pagesCAP Pneumonia Elderly Kasus 1 (Revisi)nellizulfiaNo ratings yet
- Hooper SepsismanagementDocument42 pagesHooper SepsismanagementElavarasi GanesanNo ratings yet
- Case Study Respiratory DisorderDocument17 pagesCase Study Respiratory DisorderJester GalayNo ratings yet
- Pengenalan TB, Diagnosis, Dan Pengobatannya FKM 2019Document47 pagesPengenalan TB, Diagnosis, Dan Pengobatannya FKM 2019yuly rahmawatiNo ratings yet
- PATHOPHYSIOLOGYDocument2 pagesPATHOPHYSIOLOGYmadelaine_espiritu0% (1)
- Drugs For Asthma and Other Respiratory DiseasesDocument8 pagesDrugs For Asthma and Other Respiratory DiseasesJoanna Maiden GaciasNo ratings yet
- Bronchiectasis: Causes and DiagnosisDocument25 pagesBronchiectasis: Causes and DiagnosisRathchapon BuranasawadNo ratings yet
- SARSDocument4 pagesSARSClyde EnriquezNo ratings yet
- Asma Anak - FIXDocument54 pagesAsma Anak - FIXVIVI YULIYANINo ratings yet
- Asia Pacific College of Advanced StudiesDocument4 pagesAsia Pacific College of Advanced Studiesaella gracieNo ratings yet
- Obstructive Lung Disease + Lung Cancer: Rob NicholsonDocument42 pagesObstructive Lung Disease + Lung Cancer: Rob NicholsontigizetayNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document16 pagesChronic Obstructive Pulmonary Disease (COPD)Kimberly Abella CabreraNo ratings yet
- Antifungal Agents For Preventing Fungal Infections in Critically Ill PatientsDocument34 pagesAntifungal Agents For Preventing Fungal Infections in Critically Ill PatientsRTI SanglahNo ratings yet
- PALS (Pediatric Advanced Life Support)Document48 pagesPALS (Pediatric Advanced Life Support)Jackson HakimNo ratings yet
- GRANDPAR-PATHOPHYSIOLOGY-4 (1) Pertusis Whooping Cough Secondary To PneumoniaDocument5 pagesGRANDPAR-PATHOPHYSIOLOGY-4 (1) Pertusis Whooping Cough Secondary To PneumoniaJustin AlejoNo ratings yet
- Avalox in Aecb: PP-AVE-JO-0006-1Document160 pagesAvalox in Aecb: PP-AVE-JO-0006-1Mustafa JaradatNo ratings yet
- Biologic Therapies For Severe Asthma 2022Document15 pagesBiologic Therapies For Severe Asthma 2022Marina DomencoNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- Copd Gold 2016Document5 pagesCopd Gold 2016adheNo ratings yet
- 1 BronchiectasisDocument4 pages1 BronchiectasisrenNo ratings yet
- ClindamycinDocument2 pagesClindamycinCrissah LacernaNo ratings yet
- Asthma Patient EvaluationDocument1 pageAsthma Patient Evaluatione-MedToolsNo ratings yet
- Formula and Functions in MS ExcelDocument9 pagesFormula and Functions in MS ExcelBhavana SangamNo ratings yet
- TranscriptDocument1 pageTranscriptGursharanjit SinghNo ratings yet
- Lesson 2 - Língua Inglesa 7Document21 pagesLesson 2 - Língua Inglesa 7Shara Maria Venâncio SilvaNo ratings yet
- Joint Inspection Report FormatDocument2 pagesJoint Inspection Report FormatRAMAKRISHNAN RNo ratings yet
- Boss DD-6Document28 pagesBoss DD-6Justin Alexander SanzonENo ratings yet
- Jeeadv 2022 Press ReleaseDocument6 pagesJeeadv 2022 Press ReleaseIzumiNo ratings yet
- Civic Ass JolaxDocument3 pagesCivic Ass JolaxEyob TeferaNo ratings yet
- Srijana BahadurDocument13 pagesSrijana Bahadurkhadija khanNo ratings yet
- Grammar - File12 C ROMERO VIDALDocument3 pagesGrammar - File12 C ROMERO VIDALYuy Oré Pianto50% (2)
- UK Patient Metronidazole Vaginal Gel Medication LeafletDocument4 pagesUK Patient Metronidazole Vaginal Gel Medication Leafletmarisa apriliaNo ratings yet
- Abrar AwolDocument153 pagesAbrar AwolErmias Assaminew AlmazNo ratings yet
- Jisicom - Smart System of Fast Internet Access Development Using Backbone Network MethodDocument9 pagesJisicom - Smart System of Fast Internet Access Development Using Backbone Network MethodVerdi YasinNo ratings yet
- Hotel Management System AbstractDocument8 pagesHotel Management System AbstractJayesh TupeNo ratings yet
- Math Achievement Gr11GenMathDocument3 pagesMath Achievement Gr11GenMathMsloudy VilloNo ratings yet
- Control Grupos Electrogenos LobatoDocument20 pagesControl Grupos Electrogenos LobatoEdwin Santiago Villegas AuquesNo ratings yet
- Food Photographs Practical Guidelines II Development and Use of Photographic Atlases For Assessing Food Portion SizeDocument7 pagesFood Photographs Practical Guidelines II Development and Use of Photographic Atlases For Assessing Food Portion SizemmmdeandradeNo ratings yet
- IsomerismDocument60 pagesIsomerismTenali Rama KrishnaNo ratings yet
- Traffic Monitoring SystemDocument16 pagesTraffic Monitoring Systemankit kumarNo ratings yet
- Chapter 6Document32 pagesChapter 6John Rick DayondonNo ratings yet
- Electronics by Gibilisco QandADocument22 pagesElectronics by Gibilisco QandAMary Rose AtendidoNo ratings yet
- FCo Research Report Debit Card and Bitcoin in MenaDocument10 pagesFCo Research Report Debit Card and Bitcoin in MenaJhimy JeanNo ratings yet