You might also like
- Arginine Vasopressin (AVP) and Treatment With ArginineDocument14 pagesArginine Vasopressin (AVP) and Treatment With Argininedhimas satriaNo ratings yet
- Role of Kidney in Salt and Water HomeostasisDocument31 pagesRole of Kidney in Salt and Water HomeostasisHakimah K. Suhaimi100% (1)
- The Kidney Study QuestionsDocument14 pagesThe Kidney Study QuestionsEmilie ParkeNo ratings yet
- Tarif Prodia 2020 Untuk EmailDocument32 pagesTarif Prodia 2020 Untuk Emailklinik bhaksenatragia100% (2)
- Diabetes Insipidus HarrisonDocument18 pagesDiabetes Insipidus HarrisonAlmas TNo ratings yet
- Clinical MedicineDocument15 pagesClinical MedicineTiti SulistiowatiNo ratings yet
- Fluid ElektrolitDocument63 pagesFluid ElektrolitsyifaNo ratings yet
- Vasopressin and Its Analogues in Shock States: A ReviewDocument7 pagesVasopressin and Its Analogues in Shock States: A ReviewbanzethyskyNo ratings yet
- Vasopressin and The Regulation of ThirstDocument5 pagesVasopressin and The Regulation of ThirstPame RuizNo ratings yet
- Prodia Laboratory Tariff 2020Document16 pagesProdia Laboratory Tariff 2020Kukuruyuk KukuruyukNo ratings yet
- Elevated Urinary Neutrophil Gelatinase-Associated Lipocalin Reflects Kidney InjuryDocument10 pagesElevated Urinary Neutrophil Gelatinase-Associated Lipocalin Reflects Kidney InjuryResiden KardiologiNo ratings yet
- Fluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoDocument34 pagesFluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoNinaNo ratings yet
- Cairan Biologi: I Gaa. SuartiniDocument52 pagesCairan Biologi: I Gaa. SuartiniAlif Ilham100% (1)
- Physiology and pathophysiology of the vasopressin-regulated renal water reabsorptionDocument20 pagesPhysiology and pathophysiology of the vasopressin-regulated renal water reabsorptionalma ramirezNo ratings yet
- Acute Renal Failure: An UpdateDocument52 pagesAcute Renal Failure: An Updatepranav1512No ratings yet
- Aica Ribonucleotide MechanismsDocument2 pagesAica Ribonucleotide Mechanismshaydunn55No ratings yet
- Body Fluids: M. Alif Prizarky 04011381419173 GammaDocument7 pagesBody Fluids: M. Alif Prizarky 04011381419173 GammaAlviss RmidNo ratings yet
- Activation of The Metabolic Sensor AMP-activated Protein Kinase Inhibits Aquaporin-2 Function in Kidney Principal CellsDocument11 pagesActivation of The Metabolic Sensor AMP-activated Protein Kinase Inhibits Aquaporin-2 Function in Kidney Principal CellsAlmas TNo ratings yet
- Renal System Physiology: GFR, Tubular Reabsorption and Urine ConcentrationDocument47 pagesRenal System Physiology: GFR, Tubular Reabsorption and Urine ConcentrationMuhammad Saim Bin Saeed0% (1)
- 01-Revisi 03-2022 Tarif SumateraDocument26 pages01-Revisi 03-2022 Tarif SumateraAmelia Prity SyaniNo ratings yet
- Electrolytes: George A. HarwellDocument29 pagesElectrolytes: George A. HarwellWho Knows100% (1)
- Fluid and Electrolyte Balance: Compartments of Body and Distribution of Water by WeightDocument137 pagesFluid and Electrolyte Balance: Compartments of Body and Distribution of Water by Weight0921pyNo ratings yet
- 1 s2.0 S0014579399005876 MainDocument4 pages1 s2.0 S0014579399005876 MainPablo GabrielNo ratings yet
- Chapter-28 Electrolyte and Water Balance: January 2017Document13 pagesChapter-28 Electrolyte and Water Balance: January 2017Freddy Negron HuamaniNo ratings yet
- Hyponatremia in Cirrhosis: Pathogenesis, Clinical Significance, and ManagementDocument48 pagesHyponatremia in Cirrhosis: Pathogenesis, Clinical Significance, and ManagementrlagamNo ratings yet
- Cushing ReflexDocument4 pagesCushing ReflexJoko SusesoNo ratings yet
- Fluid and Electrolyte Imbalances Part 1Document34 pagesFluid and Electrolyte Imbalances Part 1Gabrielle Frances FernandezNo ratings yet
- Eop AnaesDocument26 pagesEop AnaesSheera EiyraaNo ratings yet
- Fluid & ElectrolytesDocument75 pagesFluid & ElectrolytesfaridahuNo ratings yet
- Fluid Management FundamentalsDocument64 pagesFluid Management FundamentalspaulaNo ratings yet
- Slide Fluids ElectrolyteDocument28 pagesSlide Fluids Electrolyteandirio7486No ratings yet
- 2long Term Regulation of Blood PressureDocument21 pages2long Term Regulation of Blood PressureamrendraNo ratings yet
- 4. Fluid and electrolyteปี4Document82 pages4. Fluid and electrolyteปี4patchara vongvijitNo ratings yet
- Tatalaksana Syok Hipovolemik & HipoglikemiaDocument40 pagesTatalaksana Syok Hipovolemik & HipoglikemiaMuhammad Daviq0% (1)
- Aquas Humor DynamicsDocument30 pagesAquas Humor DynamicsRatnesh ShuklaNo ratings yet
- Resusitasi Cairan Dan DarahDocument33 pagesResusitasi Cairan Dan DarahWahyu HidayatiNo ratings yet
- Kes - Cairan TBH ElektrolitDocument31 pagesKes - Cairan TBH ElektrolitDino Syofian TriadiNo ratings yet
- Arthrex PersonalizedCellTherapyDocument27 pagesArthrex PersonalizedCellTherapyMofit penjačka stijenaNo ratings yet
- Electrolyzed water elicits antioxidant effect in ratsDocument4 pagesElectrolyzed water elicits antioxidant effect in ratsJoaqs JoaquinNo ratings yet
- Fluid Balance: D. C. MikuleckyDocument14 pagesFluid Balance: D. C. MikuleckyJoevet T. TadlasNo ratings yet
- Fluid & Electrolytes SaurabhDocument88 pagesFluid & Electrolytes Saurabhunknownsince1986No ratings yet
- Analysis of Urine and Body Fluids FunctionsDocument5 pagesAnalysis of Urine and Body Fluids FunctionsBEVERLY JANE LLUVERASNo ratings yet
- PHARMACOLOGYDocument19 pagesPHARMACOLOGYKiela Therese LabroNo ratings yet
- Fluid and Electrolytes BalanceDocument29 pagesFluid and Electrolytes BalanceHachi Nini Shop IINo ratings yet
- Lo Week 1-1Document11 pagesLo Week 1-1Martien Silviandy SetiawanNo ratings yet
- CH 25 of GuytonDocument7 pagesCH 25 of GuytonBea Samonte100% (2)
- Management Terapi CairanDocument60 pagesManagement Terapi CairanHayat Hamzah DawiNo ratings yet
- Questions From Exam 08.09.22Document12 pagesQuestions From Exam 08.09.22Ismo SNo ratings yet
- Tema 3 Fisiologi A I FM 2013Document21 pagesTema 3 Fisiologi A I FM 2013Daniel MeravigliaNo ratings yet
- Voltage PaperDocument5 pagesVoltage Paperpisces7390No ratings yet
- ACPP enDocument4 pagesACPP enSyahdie FahledieNo ratings yet
- PEDIA REPORT - Fluids and ElectrolytesDocument47 pagesPEDIA REPORT - Fluids and ElectrolytesFaydhal SalikNo ratings yet
- Regulation of Fluid and Electrolyte BalanceDocument43 pagesRegulation of Fluid and Electrolyte BalanceMsKizzyNo ratings yet
- Body Fluid Compartment SlidesDocument18 pagesBody Fluid Compartment SlidesAkanbi FavourNo ratings yet
- Bone markers and collagen breakdown testsDocument11 pagesBone markers and collagen breakdown testsFrancesco De PalmaNo ratings yet
- Notes Cerebrospinal FluidDocument10 pagesNotes Cerebrospinal FluidsusuigenerisNo ratings yet
- Fisiologi Cairan Tubuh: DRH Nurina Titisari MSC Lab Fisiologi Veteriner 2020Document34 pagesFisiologi Cairan Tubuh: DRH Nurina Titisari MSC Lab Fisiologi Veteriner 2020Rizky SumawijayaNo ratings yet
- Biology: in Vivo Monitoring of Acetylcholine Release From Nerve Endings in Salivary GlandDocument9 pagesBiology: in Vivo Monitoring of Acetylcholine Release From Nerve Endings in Salivary GlandImas-hendryNo ratings yet
- Why Do Benign Paroxysmal Positional Vertigo EpisodDocument6 pagesWhy Do Benign Paroxysmal Positional Vertigo EpisodGugutza DoiNo ratings yet
- MCQ KidneyDocument8 pagesMCQ KidneyRimaZouzNo ratings yet
- P. Cavity: (Female Reproductive Organs)Document38 pagesP. Cavity: (Female Reproductive Organs)SAKARIYE MAXAMEDNo ratings yet
- The Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument21 pagesThe Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- Ischemia: By/Dr - Abdisamad Omar AliDocument21 pagesIschemia: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Pelvic Wall-Cont.: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument39 pagesPelvic Wall-Cont.: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- Innate & Adaptive Immunity: Innate Immunity Exposure To The Microbe (Antigen) - It Is Nonspecific andDocument14 pagesInnate & Adaptive Immunity: Innate Immunity Exposure To The Microbe (Antigen) - It Is Nonspecific andSAKARIYE MAXAMEDNo ratings yet
- Pelvic Cavity (Reproductive System) : Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument49 pagesPelvic Cavity (Reproductive System) : Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- Hemorrhage and Hemostasis: By/Dr - Abdisamad Omar AliDocument24 pagesHemorrhage and Hemostasis: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Principles of Gas Exchange Diffusionof Oxygen and Carbon Dioxide Through The Respiratory MembraneDocument23 pagesPrinciples of Gas Exchange Diffusionof Oxygen and Carbon Dioxide Through The Respiratory MembraneSAKARIYE MAXAMEDNo ratings yet
- Faculty of Medicine and Surgery Community Medicine An Introduction Lecture ThreeDocument50 pagesFaculty of Medicine and Surgery Community Medicine An Introduction Lecture ThreeSAKARIYE MAXAMEDNo ratings yet
- The Neck: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument30 pagesThe Neck: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- Metaplasia and Dysplasia: By/Dr - Abdisamad Omar AliDocument31 pagesMetaplasia and Dysplasia: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Regulation of Respiration: DR Mohamed HassanDocument27 pagesRegulation of Respiration: DR Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- The Anatomy of the Pelvic CavityDocument44 pagesThe Anatomy of the Pelvic CavitySAKARIYE MAXAMEDNo ratings yet
- The Kidneys: By/Dr - Abdisamad Omar AliDocument12 pagesThe Kidneys: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- The Pelvic Girdle: By/Dr - Abdisamad Omar AliDocument30 pagesThe Pelvic Girdle: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Temperature Regulation: Dr. Mohamed Hassan MBBS, Mmed Ped, Ph.D. CandDocument46 pagesTemperature Regulation: Dr. Mohamed Hassan MBBS, Mmed Ped, Ph.D. CandSAKARIYE MAXAMEDNo ratings yet
- Causes and Mechanisms of Atrophy, Aplasia and HypoplasiaDocument22 pagesCauses and Mechanisms of Atrophy, Aplasia and HypoplasiaSAKARIYE MAXAMEDNo ratings yet
- Covid - 19: By/Dr - Abdisamad Omar AliDocument34 pagesCovid - 19: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
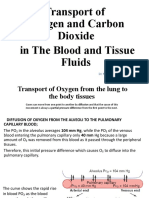
- Transport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidDocument19 pagesTransport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidSAKARIYE MAXAMEDNo ratings yet
- Introduction to Medical Bacteriology StructureDocument38 pagesIntroduction to Medical Bacteriology StructureSAKARIYE MAXAMEDNo ratings yet
- Insulin, Glucagon, and Diabetes Mellitus: Dr. Mohamed HassanDocument66 pagesInsulin, Glucagon, and Diabetes Mellitus: Dr. Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- Calcitonin Hormone Role and RegulationDocument6 pagesCalcitonin Hormone Role and RegulationSAKARIYE MAXAMEDNo ratings yet
- Thrombosis and Embolism ExplainedDocument20 pagesThrombosis and Embolism ExplainedSAKARIYE MAXAMEDNo ratings yet
- Ischemia: By/Dr - Abdisamad Omar AliDocument21 pagesIschemia: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- By/Dr - Abdisamad Omar AliDocument27 pagesBy/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- PATHOLOGYDocument32 pagesPATHOLOGYSAKARIYE MAXAMEDNo ratings yet
- Immunology: ImmunityDocument10 pagesImmunology: ImmunitySAKARIYE MAXAMEDNo ratings yet
- Secretory Functions of The Alimentary Tract: Dr. Mohamed HassanDocument55 pagesSecretory Functions of The Alimentary Tract: Dr. Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- ANATOMYDocument8 pagesANATOMYSAKARIYE MAXAMEDNo ratings yet
- Api RP 2a WSD 1pdf - CompressDocument1 pageApi RP 2a WSD 1pdf - CompressRamesh SelvarajNo ratings yet
- Consumer Behavior PP Chapter 4Document36 pagesConsumer Behavior PP Chapter 4tuongvyvyNo ratings yet
- Grab E-Receipt for 15,000 RP Ride on March 30Document1 pageGrab E-Receipt for 15,000 RP Ride on March 30WellyNo ratings yet
- CHM131 Presentation - Oxidation of MetalsDocument11 pagesCHM131 Presentation - Oxidation of MetalsNazrul ShahNo ratings yet
- Optical Fiber Communication Case Study on Material DispersionDocument5 pagesOptical Fiber Communication Case Study on Material DispersionAyush SharmaNo ratings yet
- cmc2 OiDocument147 pagescmc2 OiJesus Mack GonzalezNo ratings yet
- TM T70 BrochureDocument2 pagesTM T70 BrochureNikhil GuptaNo ratings yet
- Determination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Document11 pagesDetermination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Geovas GomezNo ratings yet
- Basketball 2011: Johnson CountyDocument25 pagesBasketball 2011: Johnson CountyctrnewsNo ratings yet
- Active Directory: Lab 1 QuestionsDocument2 pagesActive Directory: Lab 1 QuestionsDaphneHarrisNo ratings yet
- DTS-00750 Mast Maintenance ManualDocument12 pagesDTS-00750 Mast Maintenance Manualsertecs polNo ratings yet
- The Manning EquationDocument10 pagesThe Manning EquationFederico LeonNo ratings yet
- PathFit 1 (Lessons)Document10 pagesPathFit 1 (Lessons)Patawaran, Myka R.No ratings yet
- MKTG 2126 - Assignment 3Document2 pagesMKTG 2126 - Assignment 3omar mcintoshNo ratings yet
- Finding The Answers To The Research Questions (Qualitative) : Quarter 4 - Module 5Document39 pagesFinding The Answers To The Research Questions (Qualitative) : Quarter 4 - Module 5Jernel Raymundo80% (5)
- Retrenchment StrategiesDocument3 pagesRetrenchment StrategiesSABRI AKBAL MOHAMED HASSAN100% (3)
- Lecture Euler EquationDocument33 pagesLecture Euler EquationYash RajNo ratings yet
- Download Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterDocument68 pagesDownload Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterdevin.brown498100% (7)
- High Speed Board Design: Signal Integrity AnalysisDocument35 pagesHigh Speed Board Design: Signal Integrity Analysissrikanth chundiNo ratings yet
- Map Project Rubric 2018Document2 pagesMap Project Rubric 2018api-292774341No ratings yet
- Neutron SourcesDocument64 pagesNeutron SourcesJenodi100% (1)
- HFH ch04Document11 pagesHFH ch04Harikrishan RNo ratings yet
- MCQs on PharmacologyDocument101 pagesMCQs on PharmacologyMohammad Rashid88% (8)
- Unit 1Document50 pagesUnit 1vaniphd3No ratings yet
- 06 Dielectrics Capacitance 2018mkDocument41 pages06 Dielectrics Capacitance 2018mkTrần ĐứcAnhNo ratings yet
- 2008-14-03Document6 pages2008-14-03RAMON CALDERONNo ratings yet
- St. Francis de Sales Sr. Sec. School, Gangapur CityDocument12 pagesSt. Francis de Sales Sr. Sec. School, Gangapur CityArtificial GammerNo ratings yet
- GSAA HET 2005-15, Tranche B2 / BSABS 2005-TC2, Tranche M6 Shown As An Asset of Maiden LaneDocument122 pagesGSAA HET 2005-15, Tranche B2 / BSABS 2005-TC2, Tranche M6 Shown As An Asset of Maiden LaneTim BryantNo ratings yet
- Reporte Corporativo de Louis Dreyfus Company (LDC)Document21 pagesReporte Corporativo de Louis Dreyfus Company (LDC)OjoPúblico Periodismo de InvestigaciónNo ratings yet
- 01 - PV - RESCO 1d Workshop - S1 PDFDocument61 pages01 - PV - RESCO 1d Workshop - S1 PDFDeasy KurniawatiNo ratings yet