You might also like
- Faculty of Medicine and Surgery Community Medicine An Introduction Lecture ThreeDocument50 pagesFaculty of Medicine and Surgery Community Medicine An Introduction Lecture ThreeSAKARIYE MAXAMEDNo ratings yet
- MCQ KidneyDocument8 pagesMCQ KidneyRimaZouzNo ratings yet
- The Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument21 pagesThe Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- P. Cavity: (Female Reproductive Organs)Document38 pagesP. Cavity: (Female Reproductive Organs)SAKARIYE MAXAMEDNo ratings yet
- Pelvic Wall-Cont.: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument39 pagesPelvic Wall-Cont.: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- The Anatomy of the Pelvic CavityDocument44 pagesThe Anatomy of the Pelvic CavitySAKARIYE MAXAMEDNo ratings yet
- Innate & Adaptive Immunity: Innate Immunity Exposure To The Microbe (Antigen) - It Is Nonspecific andDocument14 pagesInnate & Adaptive Immunity: Innate Immunity Exposure To The Microbe (Antigen) - It Is Nonspecific andSAKARIYE MAXAMEDNo ratings yet
- The Neck: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument30 pagesThe Neck: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- Hemorrhage and Hemostasis: By/Dr - Abdisamad Omar AliDocument24 pagesHemorrhage and Hemostasis: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Ischemia: By/Dr - Abdisamad Omar AliDocument21 pagesIschemia: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Regulation of Respiration: DR Mohamed HassanDocument27 pagesRegulation of Respiration: DR Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- Pelvic Cavity (Reproductive System) : Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument49 pagesPelvic Cavity (Reproductive System) : Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- The Pelvic Girdle: By/Dr - Abdisamad Omar AliDocument30 pagesThe Pelvic Girdle: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Principles of Gas Exchange Diffusionof Oxygen and Carbon Dioxide Through The Respiratory MembraneDocument23 pagesPrinciples of Gas Exchange Diffusionof Oxygen and Carbon Dioxide Through The Respiratory MembraneSAKARIYE MAXAMEDNo ratings yet
- The Kidneys: By/Dr - Abdisamad Omar AliDocument12 pagesThe Kidneys: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
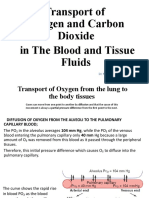
- Transport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidDocument19 pagesTransport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidSAKARIYE MAXAMEDNo ratings yet
- Insulin, Glucagon, and Diabetes Mellitus: Dr. Mohamed HassanDocument66 pagesInsulin, Glucagon, and Diabetes Mellitus: Dr. Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- Temperature Regulation: Dr. Mohamed Hassan MBBS, Mmed Ped, Ph.D. CandDocument46 pagesTemperature Regulation: Dr. Mohamed Hassan MBBS, Mmed Ped, Ph.D. CandSAKARIYE MAXAMEDNo ratings yet
- Covid - 19: By/Dr - Abdisamad Omar AliDocument34 pagesCovid - 19: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Calcitonin Hormone Role and RegulationDocument6 pagesCalcitonin Hormone Role and RegulationSAKARIYE MAXAMEDNo ratings yet
- Thrombosis and Embolism ExplainedDocument20 pagesThrombosis and Embolism ExplainedSAKARIYE MAXAMEDNo ratings yet
- Secretory Functions of The Alimentary Tract: Dr. Mohamed HassanDocument55 pagesSecretory Functions of The Alimentary Tract: Dr. Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- Metaplasia and Dysplasia: By/Dr - Abdisamad Omar AliDocument31 pagesMetaplasia and Dysplasia: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Ischemia: By/Dr - Abdisamad Omar AliDocument21 pagesIschemia: By/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- ANATOMYDocument8 pagesANATOMYSAKARIYE MAXAMEDNo ratings yet
- By/Dr - Abdisamad Omar AliDocument27 pagesBy/Dr - Abdisamad Omar AliSAKARIYE MAXAMEDNo ratings yet
- Causes and Mechanisms of Atrophy, Aplasia and HypoplasiaDocument22 pagesCauses and Mechanisms of Atrophy, Aplasia and HypoplasiaSAKARIYE MAXAMEDNo ratings yet
- Introduction to Medical Bacteriology StructureDocument38 pagesIntroduction to Medical Bacteriology StructureSAKARIYE MAXAMEDNo ratings yet
- Immunology: ImmunityDocument10 pagesImmunology: ImmunitySAKARIYE MAXAMEDNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Control of Hormone SecretionDocument77 pagesControl of Hormone Secretionjohanna deguzmanNo ratings yet
- Endocrine System - Study NotesDocument6 pagesEndocrine System - Study Notesruchikaydv007No ratings yet
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocument2 pagesDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNo ratings yet
- Kumar Verma: Lab NoDocument3 pagesKumar Verma: Lab NoSamar SinghNo ratings yet
- Hypothyroidism in PregnancyDocument4 pagesHypothyroidism in PregnancyYesicaNo ratings yet
- Hypothyroidism Concept MapDocument1 pageHypothyroidism Concept MapMonica Ugarte Treta100% (6)
- Endocrine Anatomy 4Document16 pagesEndocrine Anatomy 4Snehal JayaramNo ratings yet
- The Endocrine System Regulates Key ProcessesDocument65 pagesThe Endocrine System Regulates Key Processesadamaditya666No ratings yet
- Mulit Ligand Control ML 300 - 01A07 - MB Rev 4 - Protocol PDFDocument1 pageMulit Ligand Control ML 300 - 01A07 - MB Rev 4 - Protocol PDFvivicon2004No ratings yet
- The Seminal Vesicles and Bulbourethral GlandsDocument7 pagesThe Seminal Vesicles and Bulbourethral GlandsMustafa HaithamNo ratings yet
- Enlarged Groin Glands - Hello Sir, I Am 30 Years Old I Am Very - Practo ConsultDocument4 pagesEnlarged Groin Glands - Hello Sir, I Am 30 Years Old I Am Very - Practo ConsultTony GonzalezNo ratings yet
- G5summary of Endocrine System and Maintenance of The BodyDocument15 pagesG5summary of Endocrine System and Maintenance of The BodyNeil Ian Casuga TemblorNo ratings yet
- Asan International Radiology Master Course VER2.6Document9 pagesAsan International Radiology Master Course VER2.6Ido BramantyaNo ratings yet
- Background: Congenital Hypothyroidism Pediatric HypothyroidismDocument1 pageBackground: Congenital Hypothyroidism Pediatric HypothyroidismNiddy Rohim FebriadiNo ratings yet
- HyperthyroidismDocument18 pagesHyperthyroidismWahyuni FatmonaNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancerNinikNo ratings yet
- Thyroid Disorders Part I Hyperthyroidism Little 2006Document9 pagesThyroid Disorders Part I Hyperthyroidism Little 2006Jing XueNo ratings yet
- FNAB Its Procedure and Method of Preserving SpecimenDocument12 pagesFNAB Its Procedure and Method of Preserving SpecimenNico LokoNo ratings yet
- Nursing Management of A Patient With: HyperthyroidismDocument31 pagesNursing Management of A Patient With: Hyperthyroidismember parkNo ratings yet
- Diagnostic Approach To and Treatment of Thyroid Nodules - UpToDate PDFDocument36 pagesDiagnostic Approach To and Treatment of Thyroid Nodules - UpToDate PDFDANIEL SANTAMARIANo ratings yet
- S60 - LPL - Noida 3 N-27, Sec-18, Commercial Complex, Near. Atta Market, Noida.120-3029866/3142530 NoidaDocument2 pagesS60 - LPL - Noida 3 N-27, Sec-18, Commercial Complex, Near. Atta Market, Noida.120-3029866/3142530 Noidavimal kumar dwivediNo ratings yet
- Clinical Case Study on HypothyroidismDocument36 pagesClinical Case Study on HypothyroidismLeslie Rufino100% (1)
- Endocrine System: Hormones and GlandsDocument68 pagesEndocrine System: Hormones and GlandsJerick Sevilla SearesNo ratings yet
- Drug Study On PtuDocument4 pagesDrug Study On PtuDizzy BualanNo ratings yet
- Q3 W3 Endocrine-SystemDocument4 pagesQ3 W3 Endocrine-Systemalexandra aliporoNo ratings yet
- PDF Crash Course Endocrinology 4e Pdftahir99 VRG CompressDocument60 pagesPDF Crash Course Endocrinology 4e Pdftahir99 VRG CompressNabila Azahara PutriNo ratings yet
- AssigmentDocument27 pagesAssigmentAndleeb RajNo ratings yet
- Kasus 1 Tiroid-1Document18 pagesKasus 1 Tiroid-1Ratih Sri rezekiNo ratings yet
- Grace - HyperthyroidismDocument9 pagesGrace - HyperthyroidismOkoro Tochukwu ProsperNo ratings yet
- Organ Systems and Body CavitiesDocument18 pagesOrgan Systems and Body Cavitiessound050% (2)