You might also like
- Build A Borz Practical Scrap Metal Small Arms Vol9Document23 pagesBuild A Borz Practical Scrap Metal Small Arms Vol9Gia Linh Văn100% (2)
- MiG 21Document29 pagesMiG 21Zoran Vulovic100% (2)
- Natural ResourcesDocument5 pagesNatural ResourcesAsrock Loop100% (1)
- The Spring, Energy Accumulator A Mechanical WatchDocument5 pagesThe Spring, Energy Accumulator A Mechanical WatchismbllNo ratings yet
- L1 Finding Nemo Teacher Notes American EnglishDocument9 pagesL1 Finding Nemo Teacher Notes American Englishcris_simescuNo ratings yet
- Integral CalculusDocument48 pagesIntegral CalculusVincent CortezNo ratings yet
- Less Than 60 MilesDocument36 pagesLess Than 60 MilesDavid MckinleyNo ratings yet
- Listeria MonocytogenesDocument28 pagesListeria Monocytogenestummalapalli venkateswara rao100% (1)
- Manual stack emission monitoring standardDocument29 pagesManual stack emission monitoring standardsantisal11No ratings yet
- IKM - Sample Size Calculation in Epid Study PDFDocument7 pagesIKM - Sample Size Calculation in Epid Study PDFcindyNo ratings yet
- About Monkey PoxDocument3 pagesAbout Monkey PoxObakoma Josiah100% (1)
- Analysis of Cantilever Retaining Wall MathcadDocument4 pagesAnalysis of Cantilever Retaining Wall MathcadNéstor Walter Barrera RomeroNo ratings yet
- FPUK-0714-61536364: Salmonella InfectionsDocument11 pagesFPUK-0714-61536364: Salmonella InfectionsaliyahimranNo ratings yet
- Food Mbio II AssighnmentDocument10 pagesFood Mbio II AssighnmentRazia UrmiNo ratings yet
- Listeriosis Term PaperDocument6 pagesListeriosis Term Paperapi-302332571No ratings yet
- Listeriosis in PregnancyDocument29 pagesListeriosis in PregnancyNogie E PrasetiyoNo ratings yet
- Listeria Monocytogenes ThesisDocument4 pagesListeria Monocytogenes Thesisjennymancinibuffalo100% (1)
- Listeria Mono OIEDocument17 pagesListeria Mono OIEAjay PathakNo ratings yet
- Essay ListeriosisDocument7 pagesEssay ListeriosisNor Ashikin IsmailNo ratings yet
- Lesson 07 Listeriosis - Bacterial Infection From Listeria Monocytogenes PDFDocument4 pagesLesson 07 Listeriosis - Bacterial Infection From Listeria Monocytogenes PDFGwendolyn CalatravaNo ratings yet
- Agric AssigmentDocument4 pagesAgric Assigmentkenefavour50No ratings yet
- Foods: Listeria Monocytogenes in Fresh Produce: Outbreaks, Prevalence and Contamination LevelsDocument11 pagesFoods: Listeria Monocytogenes in Fresh Produce: Outbreaks, Prevalence and Contamination LevelsAnnisa FitriyaniNo ratings yet
- Multistate Outbreak of Listeriosis Linked To Packaged Salads Produced at Springfield, Ohio Dole Processing FacilityDocument24 pagesMultistate Outbreak of Listeriosis Linked To Packaged Salads Produced at Springfield, Ohio Dole Processing FacilityAnnisa FitriyaniNo ratings yet
- Xmas ArticleDocument3 pagesXmas ArticleKeesha MitchellNo ratings yet
- Types of Hazards and Food SafetyDocument5 pagesTypes of Hazards and Food SafetyAarajita ParinNo ratings yet
- Listeria Monocytogenes (Listeriosis) 2-12-2015Document11 pagesListeria Monocytogenes (Listeriosis) 2-12-2015MohamedNo ratings yet
- Concept of Food Contamination and Food-Borne IllnessDocument88 pagesConcept of Food Contamination and Food-Borne IllnessSheirra SantosNo ratings yet
- Concept of Food Contamination and Food-Borne IllnessDocument88 pagesConcept of Food Contamination and Food-Borne IllnessMicah ClearNo ratings yet
- Food Borne DiseasesDocument42 pagesFood Borne DiseasesJesse LeeNo ratings yet
- Ijarbs 7Document15 pagesIjarbs 7amanmalako50No ratings yet
- POLIOMYELITIS: AGENT, TRANSMISSION & PREVENTIONDocument28 pagesPOLIOMYELITIS: AGENT, TRANSMISSION & PREVENTIONyahyaNo ratings yet
- Listeria Monocytogenes (A Psychrophilic Bacterium) : ListeriosisDocument13 pagesListeria Monocytogenes (A Psychrophilic Bacterium) : ListeriosisAnous AlamiNo ratings yet
- Introduction For Food SafetyDocument16 pagesIntroduction For Food SafetyEdi AshraffNo ratings yet
- Public Health Measures for Controlling DiseaseDocument3 pagesPublic Health Measures for Controlling Disease339 Humera ShaikhNo ratings yet
- Untitled Presentation6898762338998871016Document8 pagesUntitled Presentation6898762338998871016shinwar benyamenNo ratings yet
- Listeria Monocytogenes 1Document27 pagesListeria Monocytogenes 1Mumin Alamin AllaminNo ratings yet
- Ecampus Notes-Topic 9 COMMUNICABLE DISEASES I PDFDocument18 pagesEcampus Notes-Topic 9 COMMUNICABLE DISEASES I PDFYutman Wa dagoNo ratings yet
- Food borne Disease Causes and PreventionDocument42 pagesFood borne Disease Causes and Preventionhadi yusufNo ratings yet
- Food Safety: Foodborne Illness Disease-Causing GermsDocument22 pagesFood Safety: Foodborne Illness Disease-Causing GermsMariel DelossantosNo ratings yet
- 142 P - Introductory-Food-Microbiology-FDocument142 pages142 P - Introductory-Food-Microbiology-FdrjoyloverNo ratings yet
- Listeria SlideDocument13 pagesListeria SlideTemidayoNo ratings yet
- Journal Jya 4Document5 pagesJournal Jya 4gythrieNo ratings yet
- 38 ListerioseDocument4 pages38 Listeriosetrs1234No ratings yet
- Listeriosis PDFDocument3 pagesListeriosis PDFShubhendu ChattopadhyayNo ratings yet
- Japanese Encephalitis: A Viral Brain InfectionDocument50 pagesJapanese Encephalitis: A Viral Brain InfectionPhilip SebastianNo ratings yet
- UNP-0064-archivekontoliosiss 2 PDFDocument2 pagesUNP-0064-archivekontoliosiss 2 PDFfarah rachmahNo ratings yet
- Acute Gastroenteritis Guide: Causes, Symptoms, TreatmentDocument15 pagesAcute Gastroenteritis Guide: Causes, Symptoms, TreatmentEri EriNo ratings yet
- Food-Borne Disease: Campylobacter JejuniDocument3 pagesFood-Borne Disease: Campylobacter JejuniVic JanorasNo ratings yet
- Food PoisoningDocument25 pagesFood PoisoningNicole FarquharsonNo ratings yet
- Food SafetyDocument5 pagesFood Safetyreadreaz98No ratings yet
- The Re-Emergence of Tuberculosis 2Document4 pagesThe Re-Emergence of Tuberculosis 2Navid Ali AskariNo ratings yet
- Report - Part 4 - Bacilli PDFDocument1 pageReport - Part 4 - Bacilli PDFEryel KaytNo ratings yet
- Precious Marie Dipus - Synthesis PaperDocument5 pagesPrecious Marie Dipus - Synthesis PaperPreciousNo ratings yet
- YeneneshDocument10 pagesYeneneshLakew DestaNo ratings yet
- CholeraDocument11 pagesCholerashahzadrana543No ratings yet
- GastroenteritisDocument16 pagesGastroenteritisdiqa aridaniNo ratings yet
- Typhoid DiseaseDocument28 pagesTyphoid DiseaseSaba Parvin Haque100% (1)
- Yersinia Enterocolitica Infection GuideDocument19 pagesYersinia Enterocolitica Infection GuideLaura Anghel-MocanuNo ratings yet
- School of Health and Sciences: San Lazaro Affiliation Communicable DiseasesDocument4 pagesSchool of Health and Sciences: San Lazaro Affiliation Communicable DiseasesMar OrdanzaNo ratings yet
- Trends of Major Foodborne Outbreaks in The European Union During The Years 2015-2019Document14 pagesTrends of Major Foodborne Outbreaks in The European Union During The Years 2015-2019Calidad CODITEV SACNo ratings yet
- Food Poisoning A 2013 Comprehensive Review Articles Articles Medical Toxicology Expert Witness Forensic Toxicology - DRDocument1 pageFood Poisoning A 2013 Comprehensive Review Articles Articles Medical Toxicology Expert Witness Forensic Toxicology - DRBahirahNo ratings yet
- Chronic Inflammation of The Thin Tissue Lining Each Air Sac Causes Scarring and Makes The Sacs Less FlexibleDocument8 pagesChronic Inflammation of The Thin Tissue Lining Each Air Sac Causes Scarring and Makes The Sacs Less FlexibleRosalina MarilaoNo ratings yet
- ListeriaDocument12 pagesListeriaapi-528116245No ratings yet
- ListeriaDocument10 pagesListeriasajad abasNo ratings yet
- Shupe AssignmentDocument7 pagesShupe AssignmentBright Kasapo BowaNo ratings yet
- World's Deadliest Disease and Remains A Major Public Health Problem in The PhilippinesDocument17 pagesWorld's Deadliest Disease and Remains A Major Public Health Problem in The Philippineslorella_abejuelaNo ratings yet
- DB Week 13.1Document2 pagesDB Week 13.1Aryse SantanderNo ratings yet
- Viral Vistas: Insights into Infectious Diseases: The Invisible War: Decoding the Game of Hide and Seek with PathogensFrom EverandViral Vistas: Insights into Infectious Diseases: The Invisible War: Decoding the Game of Hide and Seek with PathogensNo ratings yet
- TASK-3: Name Host Types of Diarrhe A Toxin Producin G Symptom SDocument2 pagesTASK-3: Name Host Types of Diarrhe A Toxin Producin G Symptom SRazia UrmiNo ratings yet
- Task 02 Id No:181-025-031 Differentiate Between Different Types of Foodborne Illness Foodborne IllnessDocument1 pageTask 02 Id No:181-025-031 Differentiate Between Different Types of Foodborne Illness Foodborne IllnessRazia UrmiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument10 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsRazia UrmiNo ratings yet
- Presentation1 Mbio 313Document12 pagesPresentation1 Mbio 313Razia UrmiNo ratings yet
- Mbio313 Assignment 2Document8 pagesMbio313 Assignment 2Razia UrmiNo ratings yet
- Primeasia University Molecular Genetics Techniques AssignmentDocument12 pagesPrimeasia University Molecular Genetics Techniques AssignmentRazia UrmiNo ratings yet
- MBIO 404 Assighnment 1 181-025-031Document8 pagesMBIO 404 Assighnment 1 181-025-031Razia UrmiNo ratings yet
- Mbio313 Assignment 01 181-025-031Document7 pagesMbio313 Assignment 01 181-025-031Razia UrmiNo ratings yet
- Mbio313 Assignment 01 181-025-031Document7 pagesMbio313 Assignment 01 181-025-031Razia UrmiNo ratings yet
- Aisladores Polimericos vs. Aisladores Ceramicos Unmsm PDFDocument22 pagesAisladores Polimericos vs. Aisladores Ceramicos Unmsm PDFvgcasasNo ratings yet
- NEDO's Role in International Technical Cooperation ProjectsDocument45 pagesNEDO's Role in International Technical Cooperation Projectsamitsh20072458No ratings yet
- ABR College Mechanical Mid Exam Questions on MetrologyDocument1 pageABR College Mechanical Mid Exam Questions on MetrologySrinu ArnuriNo ratings yet
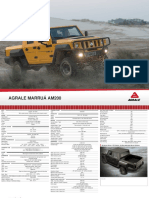
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- Rodriguez ViereaDocument51 pagesRodriguez ViereaAwawawawa UwuwuwuwuNo ratings yet
- Agribusiness ManagementDocument20 pagesAgribusiness Managementronald_leabresNo ratings yet
- Sui Gas Connection FormsDocument1 pageSui Gas Connection Formsare50% (2)
- Union Performance Ministry Cultures Monuments Antiquities 18 2013 Chapter 6Document28 pagesUnion Performance Ministry Cultures Monuments Antiquities 18 2013 Chapter 6Aarushi JainNo ratings yet
- 1N4001S THRU 1N4007S: General Purpose Silicon RectifierDocument2 pages1N4001S THRU 1N4007S: General Purpose Silicon RectifierBhadreshkumar SharmaNo ratings yet
- Chapter 11: The EyesDocument26 pagesChapter 11: The Eyesriley2021No ratings yet
- Environmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesDocument27 pagesEnvironmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesLaraNo ratings yet
- Beira Port MozambiqueDocument4 pagesBeira Port Mozambiqueripper_oopsNo ratings yet
- I PU Assignment 2023-24 For WorkshopDocument12 pagesI PU Assignment 2023-24 For Workshopfaruff111100% (1)
- Atoms & Ions Worksheet 1 /63: Atomic Number and Mass NumberDocument4 pagesAtoms & Ions Worksheet 1 /63: Atomic Number and Mass Numbercate christineNo ratings yet
- Nexon Genuine AccessoriesDocument15 pagesNexon Genuine AccessoriesjagaaniNo ratings yet
- Hematological Conditions QUESTIONSDocument9 pagesHematological Conditions QUESTIONSCJ RelleveNo ratings yet
- Fiat Type 199 Punto Evo 3 PDFDocument9 pagesFiat Type 199 Punto Evo 3 PDFGestione SportivaNo ratings yet
- CP 108: Home Assignment Topics-2021Document2 pagesCP 108: Home Assignment Topics-2021Biswajit PaulNo ratings yet
- 241-Article Text-1014-1-10-20201017Document8 pages241-Article Text-1014-1-10-20201017derismurib4No ratings yet
- 4.5.1.1 Inside and Outside Control Instructions - IG PDFDocument4 pages4.5.1.1 Inside and Outside Control Instructions - IG PDFMaksim Korsakov100% (4)