You might also like
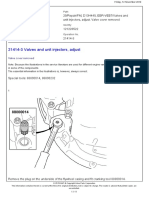
- 21414-3 Valves and Unit Injectors, AdjustDocument11 pages21414-3 Valves and Unit Injectors, AdjustTeguh Imam Adri100% (1)
- Colon CancerDocument64 pagesColon CancerAjay BhagatNo ratings yet
- Python Tutorial For BeginnersDocument10 pagesPython Tutorial For BeginnerscidBookBee100% (2)
- Small Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerDocument32 pagesSmall Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerMia DangaNo ratings yet
- Hepatocellular Carcinoma: Manal Abdel Hamid Associate Prof. of Medical OncologyDocument24 pagesHepatocellular Carcinoma: Manal Abdel Hamid Associate Prof. of Medical OncologyfridaNo ratings yet
- HEPATOMADocument30 pagesHEPATOMASemestaNo ratings yet
- SS 551-2009 - PreviewDocument12 pagesSS 551-2009 - PreviewRichard LeongNo ratings yet
- Relevance of Serum Tumor MarkersDocument25 pagesRelevance of Serum Tumor MarkersDrPawan KirtaniNo ratings yet
- Ch7 NeoplasmDocument96 pagesCh7 Neoplasmmormor80No ratings yet
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantDaniel Alfredo Tenorio GonzálezNo ratings yet
- Liver TumorsDocument52 pagesLiver TumorsRajendra DesaiNo ratings yet
- Hepatocellular CarcinomaDocument24 pagesHepatocellular CarcinomaEthan Matthew HuntNo ratings yet
- Management Gastric CancerDocument76 pagesManagement Gastric Cancerwawan siswokoNo ratings yet
- Audi 101 and 102 Auditing NotesDocument126 pagesAudi 101 and 102 Auditing Notesgavin henningNo ratings yet
- Hepatocellular Carcinoma: Dr. Isbandiyah, SPPDDocument26 pagesHepatocellular Carcinoma: Dr. Isbandiyah, SPPDMeta ShofiaNo ratings yet
- ListDocument331 pagesListabhidssNo ratings yet
- Viral Hepatitis Clinical CorrelationDocument59 pagesViral Hepatitis Clinical Correlationdrhananfathy100% (3)
- Gis 1 EnglishDocument85 pagesGis 1 Englishexand861No ratings yet
- Hepatocellular CarcinomaDocument62 pagesHepatocellular CarcinomaWilliams Emmanuel AdeyeyeNo ratings yet
- Colorectal Cancer: - Dr. Suneet KhuranaDocument36 pagesColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooNo ratings yet
- Assessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesDocument45 pagesAssessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesboubiyouNo ratings yet
- A2 Prostate Ca - AinDocument4 pagesA2 Prostate Ca - AinNur Liyana Ahmad ZakiNo ratings yet
- OnkologieDocument41 pagesOnkologieNatz BatzNo ratings yet
- Definisi Epidemiologi Klasifikasi Etiologi & Faktor Risiko Manifestasi Klinis Diagnosis Sistem Staging TerapiDocument37 pagesDefinisi Epidemiologi Klasifikasi Etiologi & Faktor Risiko Manifestasi Klinis Diagnosis Sistem Staging TerapikadinfathiaNo ratings yet
- Biologi Neoplasma: DR Suryani Eka Mustika SP - PADocument33 pagesBiologi Neoplasma: DR Suryani Eka Mustika SP - PAHarry FaisalNo ratings yet
- Tumor Urogenital: Dr. Alvarino SPB SpuDocument41 pagesTumor Urogenital: Dr. Alvarino SPB SpuDita Azzahra SupraptoNo ratings yet
- LiverDocument177 pagesLiverChiiraq EugeneNo ratings yet
- Far Eastern University - Nicanor Reyes Medical FoundationDocument2 pagesFar Eastern University - Nicanor Reyes Medical FoundationJyl Yan SelasorNo ratings yet
- 14 HF-Limfoma GI TractDocument27 pages14 HF-Limfoma GI TractNur akilaNo ratings yet
- Neoplasms of The Genitourinary TractDocument71 pagesNeoplasms of The Genitourinary Tractvishalzenia100% (2)
- 4 Esophagus 2018Document55 pages4 Esophagus 2018a20-0353-958No ratings yet
- Surgery of Colorectal Cancer: IncidenceDocument31 pagesSurgery of Colorectal Cancer: Incidencekarim1291No ratings yet
- Genitourinary Cancer: Urology Division, Surgery Department Medical Faculty, University of Sumatera UtaraDocument31 pagesGenitourinary Cancer: Urology Division, Surgery Department Medical Faculty, University of Sumatera UtarafeonajaparNo ratings yet
- Tumor Urogenital: Dr. Hariyono, SpuDocument42 pagesTumor Urogenital: Dr. Hariyono, SpumelianyNo ratings yet
- Triple Synchronous Malignancy: A Case ofDocument21 pagesTriple Synchronous Malignancy: A Case ofAshish SatyalNo ratings yet
- Sunaryo Hardjowijoto Wahjoe Djatisoesanto: Division Oncology Department of Urology Airlangga School of MedicineDocument33 pagesSunaryo Hardjowijoto Wahjoe Djatisoesanto: Division Oncology Department of Urology Airlangga School of MedicineAdith FileanugrahaNo ratings yet
- ARROCase SalivaryGlandTumorsDocument61 pagesARROCase SalivaryGlandTumorssnolinNo ratings yet
- 1diseases of The Colon and RectumDocument42 pages1diseases of The Colon and RectumEngidawork MaruNo ratings yet
- Gastroenterology Clinical Focus High Yield Gi and HepatologyDocument426 pagesGastroenterology Clinical Focus High Yield Gi and HepatologyAhana MukherjeeNo ratings yet
- Differentiated Thyroid Cancer: Presenter: DR Aakriti Athavale Moderated By: GP Capt (DR) PK SahuDocument43 pagesDifferentiated Thyroid Cancer: Presenter: DR Aakriti Athavale Moderated By: GP Capt (DR) PK SahuAakritiNo ratings yet
- Oesophageal Carcinom A & Its Managment: DR - Vivek Garg (JR-2) Dr. Mohd. Athar (Oncosurgeon)Document71 pagesOesophageal Carcinom A & Its Managment: DR - Vivek Garg (JR-2) Dr. Mohd. Athar (Oncosurgeon)Abhishek KumarNo ratings yet
- Stomach Neoplasms: Professor Ravi KantDocument75 pagesStomach Neoplasms: Professor Ravi KantcoksiNo ratings yet
- Cancer OropharynxDocument108 pagesCancer OropharynxAshokNo ratings yet
- Dr. Pankaj Tejasvi: Dept. of Surgery MGMMC & MYH IndoreDocument76 pagesDr. Pankaj Tejasvi: Dept. of Surgery MGMMC & MYH IndoreDang HungNo ratings yet
- SaleemDocument14 pagesSaleemHafiz AwaisNo ratings yet
- Prostate Cancer: AdenocarcinomaDocument3 pagesProstate Cancer: AdenocarcinomaSarah AbdullahNo ratings yet
- c2f PresDocument25 pagesc2f Presapi-195799092No ratings yet
- TJW Bladder CancerDocument35 pagesTJW Bladder CancerShariq ShaNo ratings yet
- Mass in Epigastrium-2Document37 pagesMass in Epigastrium-2brown_chocolate87643100% (1)
- Litiasis VesicularDocument26 pagesLitiasis VesicularEULER FARADAY ALTAMIRANO FARFANNo ratings yet
- Tumor UG - Edit 1Document74 pagesTumor UG - Edit 1Krisna Adhitya WilantaraNo ratings yet
- Gastric CancerDocument126 pagesGastric Cancermwani775100% (1)
- Lynch SyndDocument4 pagesLynch SyndRamez AntakiaNo ratings yet
- Oncology - Colorectal Cancer BrieflyDocument1 pageOncology - Colorectal Cancer Briefly20094113No ratings yet
- Urology Sub Division Department of Surgery Medical School University of Sumatera UtaraDocument26 pagesUrology Sub Division Department of Surgery Medical School University of Sumatera UtaraAulia SiregarNo ratings yet
- Pancreatic Cancer: DR - Avit Suchitra, SPB - (K) BDDocument24 pagesPancreatic Cancer: DR - Avit Suchitra, SPB - (K) BDdevin mahendikaNo ratings yet
- Genitourinary Tumors: Urology Division, Surgery Department Medical Faculty, University of Sumatera UtaraDocument32 pagesGenitourinary Tumors: Urology Division, Surgery Department Medical Faculty, University of Sumatera UtaraJoice RumondangNo ratings yet
- ThyroidDocument43 pagesThyroidchowhan04No ratings yet
- Pleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterDocument46 pagesPleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterderereyNo ratings yet
- Tuberculosis Pleural Effusion - ManagementDocument68 pagesTuberculosis Pleural Effusion - Managementhei thereNo ratings yet
- Efusi PeluraDocument68 pagesEfusi Pelurahei thereNo ratings yet
- Surg 2 JaundicedDocument94 pagesSurg 2 Jaundicedapi-3728522No ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- Anticoagulation TherapyFrom EverandAnticoagulation TherapyJoe F. LauNo ratings yet
- Studentzone 02 2017Document3 pagesStudentzone 02 2017YahiaEl-obidyNo ratings yet
- Mpo - Compressor MotorDocument2 pagesMpo - Compressor MotorroelNo ratings yet
- Commission Breakup: Khulna SadarDocument4 pagesCommission Breakup: Khulna Sadarsamiul azadNo ratings yet
- Visiting Angkor Wat - The Ultimate Guide (With A Map)Document1 pageVisiting Angkor Wat - The Ultimate Guide (With A Map)Vibol ChhomNo ratings yet
- Project Estmate (Final)Document65 pagesProject Estmate (Final)Bilal Ahmed BarbhuiyaNo ratings yet
- PD233 Lecture16Document17 pagesPD233 Lecture16Sameer GautamNo ratings yet
- Society & Culture With Family Planning PrelimDocument2 pagesSociety & Culture With Family Planning PrelimKent LNo ratings yet
- Uttar Pradesh Land Revenue (Amendment) Act, 1970Document4 pagesUttar Pradesh Land Revenue (Amendment) Act, 1970Latest Laws TeamNo ratings yet
- EndorseDocument2 pagesEndorseAbhay SrivastavaNo ratings yet
- Cobre Panamá - Feasibility (2010)Document188 pagesCobre Panamá - Feasibility (2010)Nicolas CarrascoNo ratings yet
- Government Memo On Claimed Farms - Part 1Document25 pagesGovernment Memo On Claimed Farms - Part 1noko-makgato-6232No ratings yet
- CbgapiDocument32 pagesCbgapiBurke Coco NoorNo ratings yet
- Name GroupDocument4 pagesName GroupAmit KashikarNo ratings yet
- Air Pollution EcologyDocument4 pagesAir Pollution EcologyCharlemyne Quevedo LachanceNo ratings yet
- Image Enhancement in The Spatial DomainDocument60 pagesImage Enhancement in The Spatial DomainSurenderMalanNo ratings yet
- Chapter - 5 Organic MaterialsDocument36 pagesChapter - 5 Organic MaterialsJayvin PrajapatiNo ratings yet
- IntegrationDocument23 pagesIntegrationnikowawaNo ratings yet
- ISUZU Vehicle XM Spec 4JB1TDocument4 pagesISUZU Vehicle XM Spec 4JB1TKevin Sevilla100% (1)
- Law of Crimes Assingement: Done byDocument8 pagesLaw of Crimes Assingement: Done byAadhitya NarayananNo ratings yet
- Drug Study CaseDocument7 pagesDrug Study CaseKevin Sam AguirreNo ratings yet
- 17CS754 San Notes Svit Module 3Document30 pages17CS754 San Notes Svit Module 3Jacob DragonetteNo ratings yet
- Environment Position PaperDocument6 pagesEnvironment Position PaperJenlisa KimanobanNo ratings yet
- Load Case CombinationsDocument5 pagesLoad Case CombinationsFrancisco UgarteNo ratings yet
- Record A FaceTime CallDocument3 pagesRecord A FaceTime Calltsultim bhutiaNo ratings yet
- Solution Manual For Mis Cases Decision Making 4th Edition by MillerDocument8 pagesSolution Manual For Mis Cases Decision Making 4th Edition by MillerElizabethSteelefocgk100% (81)