You might also like
- Health Teaching Plan (Breastfeeding)Document5 pagesHealth Teaching Plan (Breastfeeding)Zam Pamate100% (7)
- Breastfeeding Your Little OneDocument12 pagesBreastfeeding Your Little OneCalvin LooNo ratings yet
- Breastfeeding Introduction - Grace Tay HandoutDocument73 pagesBreastfeeding Introduction - Grace Tay Handoutazri.hafiziNo ratings yet
- Techniques of BreastfeedingDocument9 pagesTechniques of BreastfeedingLerma PagcaliwanganNo ratings yet
- Second Stage Labor ReportDocument34 pagesSecond Stage Labor ReportDimple AnticamaraNo ratings yet
- BreastfeedingDocument3 pagesBreastfeedingXjunz TolzNo ratings yet
- Breastfeeding - Express and Store PDFDocument24 pagesBreastfeeding - Express and Store PDFM Isyhaduul IslamNo ratings yet
- Breast EngorgeDocument16 pagesBreast EngorgeNadiya RashidNo ratings yet
- Postpartum Discharge InstructionsDocument7 pagesPostpartum Discharge InstructionsGilianne JimeneaNo ratings yet
- East FeedingDocument5 pagesEast FeedingJeya vanithaNo ratings yet
- Northwestern Medicine NICU Breast Pump Usage NMHDocument5 pagesNorthwestern Medicine NICU Breast Pump Usage NMHFayrouz EssawiNo ratings yet
- Breastfeeding OrientationDocument41 pagesBreastfeeding Orientationstudyyash100% (2)
- PL 969.1 Antenatal Colostrum HarvestingDocument8 pagesPL 969.1 Antenatal Colostrum HarvestingAmy PainterNo ratings yet
- Breastfeeding FinalDocument25 pagesBreastfeeding FinalWengel RedkissNo ratings yet
- Importance of BreastfeedingDocument6 pagesImportance of BreastfeedingJade HemmingsNo ratings yet
- Breastfeeding LectDocument26 pagesBreastfeeding LectJan Erika AlmeronNo ratings yet
- Health Teaching Plan BreastfeedingDocument6 pagesHealth Teaching Plan BreastfeedingSandeepNo ratings yet
- G Hid Montes Sory Pentru Bebelus IDocument42 pagesG Hid Montes Sory Pentru Bebelus Imelimatyas100% (1)
- Breastfeeding TechniqueDocument2 pagesBreastfeeding TechniqueKaye Niale BaleteNo ratings yet
- ISIS Manual Breast Pump: Skincare For BabiesDocument8 pagesISIS Manual Breast Pump: Skincare For BabiesfarhanmileNo ratings yet
- Breastfeeding Pamphlet - English ReformatDocument2 pagesBreastfeeding Pamphlet - English ReformatRisalouise LucasNo ratings yet
- Feeding of Normal AND Low Birth Weight Babies: Amola Khandwala Under Guidance of DR Dipen PatelDocument54 pagesFeeding of Normal AND Low Birth Weight Babies: Amola Khandwala Under Guidance of DR Dipen PatelDeep ShahNo ratings yet
- Lesson Plan On Expressed Breast MilkDocument13 pagesLesson Plan On Expressed Breast MilkBinal Joshi100% (3)
- Stages of Breastfeeding August 2017Document6 pagesStages of Breastfeeding August 2017tabbyketketNo ratings yet
- Feeding of High Risk NeonatesDocument33 pagesFeeding of High Risk Neonatesannu panchal67% (3)
- PostpartumDocument7 pagesPostpartummaryNo ratings yet
- 1 Preventive PediatricsDocument115 pages1 Preventive Pediatricssorianokentjonyl09No ratings yet
- Manual Breast Manual ExpressionDocument9 pagesManual Breast Manual ExpressionhoneykrizelNo ratings yet
- Lamaze Session 3Document32 pagesLamaze Session 3Andrea Olimpia PopNo ratings yet
- Breastfeeding and Breast Care: King Edward Memorial HospitalDocument13 pagesBreastfeeding and Breast Care: King Edward Memorial HospitalSteve JeffersonNo ratings yet
- 2 BF BCDocument5 pages2 BF BCKyle GonzalesNo ratings yet
- Guidelines To ExercisingDocument12 pagesGuidelines To ExercisingSathish GlNo ratings yet
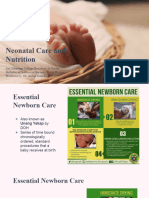
- 10 Neonatal Care and NutritionDocument56 pages10 Neonatal Care and NutritionJn CasuelaNo ratings yet
- A NEW DADS HANDBOOK: Settle & sleep in 90 seconds plus other secrets from a real dadFrom EverandA NEW DADS HANDBOOK: Settle & sleep in 90 seconds plus other secrets from a real dadNo ratings yet
- NICU Discharge PlanDocument58 pagesNICU Discharge PlanElla Mae AbutinNo ratings yet
- Presentation 1Document55 pagesPresentation 1roshen02No ratings yet
- NCM 107 Postpartum Care Guide QuestionDocument6 pagesNCM 107 Postpartum Care Guide QuestionMiguel LigasNo ratings yet
- Maternal and Child SeparationDocument40 pagesMaternal and Child Separationcorzpun168678No ratings yet
- Breastfeeding Lecture PowerpointDocument36 pagesBreastfeeding Lecture PowerpointMa. Isabel A. EnriquezNo ratings yet
- Unang YakapDocument27 pagesUnang YakapMary Faith Kiat-ongNo ratings yet
- Yes Going To Breastfeed EnglishDocument2 pagesYes Going To Breastfeed EnglishalexandracappNo ratings yet
- Child Care Procedures (New)Document18 pagesChild Care Procedures (New)Donna Lyngie MacaranasNo ratings yet
- Takingbabyhome EnglishDocument20 pagesTakingbabyhome Englishwaleed sallamNo ratings yet
- Infant Feeding: DR - Divyarani.D.C Assistant Professor Department of Pediatrics, KoimsDocument69 pagesInfant Feeding: DR - Divyarani.D.C Assistant Professor Department of Pediatrics, KoimsDr Divyarani D CNo ratings yet
- Breast Feeding Teaching ToolDocument5 pagesBreast Feeding Teaching ToolRene ContrerasNo ratings yet
- Mothers ClassDocument73 pagesMothers ClassJuliana Andres83% (6)
- Care Plan For Breast EngorgementDocument2 pagesCare Plan For Breast EngorgementTin Jaugan0% (1)
- Manual Expression of Breast Milk Marmet TechniqueDocument2 pagesManual Expression of Breast Milk Marmet TechniqueandrigunariNo ratings yet
- BREAST - CARE FinalDocument5 pagesBREAST - CARE FinalSandhya GuptaNo ratings yet
- CakeMaternity Breastfeeding GuideDocument17 pagesCakeMaternity Breastfeeding GuideisliNo ratings yet
- Finals 1. Maternal and Child Nursing - IntrapartumDocument11 pagesFinals 1. Maternal and Child Nursing - IntrapartumAlgen GayapNo ratings yet
- Breech Baby - Causes, Complications, Turning & DeliveryDocument5 pagesBreech Baby - Causes, Complications, Turning & DeliveryJoshua TomoNo ratings yet
- Lecture (1) Breast FeedingDocument15 pagesLecture (1) Breast Feedingbongomin joelNo ratings yet
- pp0214 Nut FeedingDocument2 pagespp0214 Nut Feedingapi-169796451No ratings yet
- Jack Newman Latching HandoutDocument3 pagesJack Newman Latching HandoutOctavia Raica100% (1)
- A New Mother's Guide: To Breastfeeding SuccessDocument16 pagesA New Mother's Guide: To Breastfeeding SuccessharishNo ratings yet
- Keys To Successful Breastfeeding Based On Recommendations of WHO and Ministry of Health of Ukraine O.V. RusanovskayaDocument15 pagesKeys To Successful Breastfeeding Based On Recommendations of WHO and Ministry of Health of Ukraine O.V. RusanovskayaGeorge Eusebio KuodzaNo ratings yet
- B.inggrisDocument8 pagesB.inggrisIka noviNo ratings yet
- Case Study-Typhoid FeverDocument37 pagesCase Study-Typhoid Feverjlhynn100% (2)
- MS Case PresDocument33 pagesMS Case PresShaine_Thompso_6877No ratings yet
- Pleura: LungsDocument7 pagesPleura: LungsbarbacumlaudeNo ratings yet
- Surgery McqsDocument8 pagesSurgery McqsZahra Gurmani100% (3)
- The Biology of Mind: Powerpoint® PresentationDocument56 pagesThe Biology of Mind: Powerpoint® PresentationJessa PacamparaNo ratings yet
- 2.2 - All Worksheets - Homework Sheets - Extension SheetsDocument20 pages2.2 - All Worksheets - Homework Sheets - Extension SheetslogineNo ratings yet
- 038 Health In1 PDFDocument281 pages038 Health In1 PDFbhatchinmay7100% (1)
- Brain Areas - Location and FunctionDocument12 pagesBrain Areas - Location and FunctionMattGilmoreNo ratings yet
- MCQsDocument32 pagesMCQsamNo ratings yet
- Brain Art Coloring Book f14Document3 pagesBrain Art Coloring Book f14api-261267976No ratings yet
- Physiological Origin of Biomedical SignalDocument35 pagesPhysiological Origin of Biomedical Signalsouvik5000100% (1)
- NEUROTRANSMITTERDocument28 pagesNEUROTRANSMITTERiqiqiqiqiq100% (1)
- Recurrent Hypokalemic ParalysisDocument10 pagesRecurrent Hypokalemic ParalysisDuke SucgangNo ratings yet
- Laboratory Exercise No. 8 Nervous SystemDocument4 pagesLaboratory Exercise No. 8 Nervous SystemAce ClaireNo ratings yet
- Marketing Management Kotler Keller 14th Edition Solutions ManualDocument24 pagesMarketing Management Kotler Keller 14th Edition Solutions ManualStephanieGarciawora100% (38)
- Understanding Medical Surgical Nursing - 0849-0849Document1 pageUnderstanding Medical Surgical Nursing - 0849-0849Anas TasyaNo ratings yet
- Hormon Hipotalamus HipofisisDocument20 pagesHormon Hipotalamus HipofisisSyam UnhasNo ratings yet
- Lecture 22 - The Digestive TractDocument32 pagesLecture 22 - The Digestive TractCarl Agape DavisNo ratings yet
- Hormonal Responses To Exercise-1Document48 pagesHormonal Responses To Exercise-1CHANGEZ KHAN SARDARNo ratings yet
- 2 Yr Zoology VSAQSDocument2 pages2 Yr Zoology VSAQSmnygq7dgqwNo ratings yet
- Nogier FrequenciesDocument2 pagesNogier Frequenciesinsead83% (6)
- Iycf AsiaDocument68 pagesIycf AsiaYahye CMNo ratings yet
- G-10 Biology Transportation and Excretion Question BankDocument13 pagesG-10 Biology Transportation and Excretion Question BankabimalligaNo ratings yet
- Anatomy MUHS PAPERSDocument26 pagesAnatomy MUHS PAPERSJayesh PawarNo ratings yet
- Medical-Surgical NCLEX Practice QUIZ Flashcards - QuizletDocument9 pagesMedical-Surgical NCLEX Practice QUIZ Flashcards - QuizletErika Bacarro100% (1)
- Endocrine SystemDocument8 pagesEndocrine SystemgabbypeigNo ratings yet
- Microsoft PowerPoint - Anfisman2Document30 pagesMicrosoft PowerPoint - Anfisman2Aswin Gumelar R.No ratings yet
- Nursing Lecture EndocrineDocument16 pagesNursing Lecture EndocrineAedge010100% (3)