You might also like
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Foreign Bodies of The Ear and NoseDocument6 pagesForeign Bodies of The Ear and NoseLeez KhanNo ratings yet
- Ear, Nose, and Throat EmergenciesDocument23 pagesEar, Nose, and Throat EmergenciesRajesh SharmaNo ratings yet
- Assisting Bone Marrow Aspiration DraftDocument6 pagesAssisting Bone Marrow Aspiration Draftabcde pwnjabiNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- New Vertin CME Slides FinalDocument98 pagesNew Vertin CME Slides FinalGaurav KatariaNo ratings yet
- ENT Guide for Neck ExaminationDocument79 pagesENT Guide for Neck ExaminationJohn M. HemsworthNo ratings yet
- Cortical Mastoid SurgeryDocument22 pagesCortical Mastoid Surgerymanu100% (1)
- Paranasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandParanasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Initial Assessment and Management of Trauma PatientsDocument8 pagesInitial Assessment and Management of Trauma PatientsAlvin De LunaNo ratings yet
- Short Case PterygiumDocument21 pagesShort Case PterygiumRSNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- AnesthesiaDocument59 pagesAnesthesiaHasse Hasse100% (1)
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentFrom EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahNo ratings yet
- Medication Errors: Causes and PreventionDocument22 pagesMedication Errors: Causes and PreventionUzamaNo ratings yet
- Clinical Microbiology Laboratory Test RequisitionDocument1 pageClinical Microbiology Laboratory Test RequisitionRhodjane Dela Cruz0% (1)
- Research Synopsis FormatDocument13 pagesResearch Synopsis Formatmaya vermaNo ratings yet
- 1) BiopsyDocument30 pages1) BiopsySosa GeorgeNo ratings yet
- Aqueous HumorDocument46 pagesAqueous HumorJ NATASHA MARIANo ratings yet
- LeprosyDocument26 pagesLeprosyFamous manNo ratings yet
- Perimetry: By: Najwa Mansuri 3 Batch 3 Year B.OPTOM BMCO, SuratDocument71 pagesPerimetry: By: Najwa Mansuri 3 Batch 3 Year B.OPTOM BMCO, SuratNajwa MansuriNo ratings yet
- Cataract NewDocument51 pagesCataract NewApoorva AgrawalNo ratings yet
- Dhanusthamba/Dhanurvata/Tetanus: Dr. Mahesh C KundagolDocument19 pagesDhanusthamba/Dhanurvata/Tetanus: Dr. Mahesh C KundagolkundagolNo ratings yet
- Intracranial SurgeryDocument12 pagesIntracranial SurgerysetanpikulanNo ratings yet
- Causes, Signs, Treatment of Acute Otitis MediaDocument19 pagesCauses, Signs, Treatment of Acute Otitis MediaRajesh Sharma100% (1)
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDocument2 pagesAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasNo ratings yet
- Maxillary Sinus CarcinomaDocument4 pagesMaxillary Sinus CarcinomaSuresh MettaNo ratings yet
- CPR 1Document12 pagesCPR 1Renju JoseNo ratings yet
- Surgical Management of Thyroid NeoplasmsDocument15 pagesSurgical Management of Thyroid NeoplasmsalameluNo ratings yet
- Link ClickDocument4 pagesLink ClickMitch MontielNo ratings yet
- TRIAGEDocument55 pagesTRIAGELaveena AswaleNo ratings yet
- Common Ent DisordersDocument20 pagesCommon Ent DisordersattaheeraNo ratings yet
- Stridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiDocument33 pagesStridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiVishal GauravNo ratings yet
- Abnormal EcgDocument6 pagesAbnormal EcgYash Raj SisodiyaNo ratings yet
- Neurological Health AssessmentDocument63 pagesNeurological Health AssessmentAhmed ElryahNo ratings yet
- Presentation1 Cervical BiopsyDocument14 pagesPresentation1 Cervical BiopsyChanta MaharjanNo ratings yet
- Muscle Strength TestingDocument3 pagesMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Oncological Emergencies-2018Document8 pagesOncological Emergencies-2018CamiloRada100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Nasal Fractures: Trauma To NoseDocument38 pagesNasal Fractures: Trauma To NoseSindhura ManjunathNo ratings yet
- Acute Laryngitis: Li SGD 21 LBM 5Document40 pagesAcute Laryngitis: Li SGD 21 LBM 511juni09No ratings yet
- Acute Otitis MediaDocument18 pagesAcute Otitis MediaaliramzanNo ratings yet
- Journal Reading on Evidence-Based Treatment of Otitis ExternaDocument45 pagesJournal Reading on Evidence-Based Treatment of Otitis ExternaSonya HyekyoNo ratings yet
- FundosDocument13 pagesFundosLi FaungNo ratings yet
- Acute Suppurative Otitis MediaDocument41 pagesAcute Suppurative Otitis Mediarani suwadjiNo ratings yet
- Epid COPDDocument9 pagesEpid COPDAgung WistaraNo ratings yet
- Recurrent Ear Infection Diagnosis and Treatment ScenarioDocument23 pagesRecurrent Ear Infection Diagnosis and Treatment ScenarioAakashNo ratings yet
- Sudden Sensorineural Hearing Loss: Christopher D. Muller, M.D. Jeffrey Vrabec, M.DDocument64 pagesSudden Sensorineural Hearing Loss: Christopher D. Muller, M.D. Jeffrey Vrabec, M.DDrKunal KaradeNo ratings yet
- Cancer LaryncDocument35 pagesCancer LaryncSaya MenangNo ratings yet
- Chronic SinusitisDocument19 pagesChronic SinusitisMunawwar AwaNo ratings yet
- Nasogastric Intubation Medical NCO CourseDocument32 pagesNasogastric Intubation Medical NCO CourseBilly PeterNo ratings yet
- Cuerp Extra en Orl-Econa-Feb 2019Document10 pagesCuerp Extra en Orl-Econa-Feb 2019surgeonyNo ratings yet
- Musculoskeletal System Disorders f03Document34 pagesMusculoskeletal System Disorders f03Marianne LayloNo ratings yet
- Implementation of An Inpatient Diabetes Team - Impact On HypoglyceDocument2 pagesImplementation of An Inpatient Diabetes Team - Impact On HypoglyceMarianne LayloNo ratings yet
- New Employee Orientation Evaluation Form: Rating Scheme: Not Helpful 1 Helpful 3 Extremely Helpful 6Document3 pagesNew Employee Orientation Evaluation Form: Rating Scheme: Not Helpful 1 Helpful 3 Extremely Helpful 6Marianne LayloNo ratings yet
- High Alert: MedicationsDocument25 pagesHigh Alert: MedicationsMarianne LayloNo ratings yet
- Nursing Responsibilities In: MedicationsDocument23 pagesNursing Responsibilities In: MedicationsMarianne LayloNo ratings yet
- Msc-Medication Administration PolicyDocument42 pagesMsc-Medication Administration PolicyMarianne Laylo100% (1)
- Nursing Documentation Course 2020Document36 pagesNursing Documentation Course 2020Marianne Laylo100% (1)
- Blood TransfusionDocument35 pagesBlood TransfusionMarianne LayloNo ratings yet
- Nursing Orientation Program Intravenous TherapyDocument45 pagesNursing Orientation Program Intravenous TherapyMarianne LayloNo ratings yet
- Crash Cart Emergency DrugsDocument103 pagesCrash Cart Emergency DrugsMarianne Laylo67% (3)
- Ebp Peritonsillar AbscessDocument1 pageEbp Peritonsillar AbscessMarianne LayloNo ratings yet
- Peritonsillar AbscessDocument19 pagesPeritonsillar AbscessMarianne LayloNo ratings yet
- Peritonsillar AbscessDocument19 pagesPeritonsillar AbscessMarianne LayloNo ratings yet
- Global CityDocument3 pagesGlobal Citycr lamigoNo ratings yet
- Appendix 2 Overview On HRM Defintions Contribution and Avenues For Future ResearchDocument6 pagesAppendix 2 Overview On HRM Defintions Contribution and Avenues For Future ResearchBarun Kumar SinghNo ratings yet
- Mechanical Seminar ListDocument9 pagesMechanical Seminar ListalokbdasNo ratings yet
- PSE Archery2015 RecurveDocument10 pagesPSE Archery2015 RecurvecarlheindlNo ratings yet
- An Improved TS Algorithm For Loss-Minimum Reconfiguration in Large-Scale Distribution SystemsDocument10 pagesAn Improved TS Algorithm For Loss-Minimum Reconfiguration in Large-Scale Distribution Systemsapi-3697505No ratings yet
- Indian Pharmaceutical Industry: The Changing Dynamics: April 2016Document26 pagesIndian Pharmaceutical Industry: The Changing Dynamics: April 2016payal joshiNo ratings yet
- Supreme Court: Arsenio C. Villalon, Jr. For Petitioner. Labaguis, Loyola, Angara & Associates For Private RespondentDocument43 pagesSupreme Court: Arsenio C. Villalon, Jr. For Petitioner. Labaguis, Loyola, Angara & Associates For Private RespondentpiaNo ratings yet
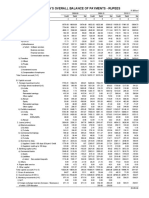
- Table 141: India'S Overall Balance of Payments - RupeesDocument2 pagesTable 141: India'S Overall Balance of Payments - Rupeesmahbobullah rahmaniNo ratings yet
- HQ 170aDocument82 pagesHQ 170aTony WellsNo ratings yet
- Last Minute Reviewer for 2019 Bar ExamDocument19 pagesLast Minute Reviewer for 2019 Bar ExamFrances Ann Teves100% (1)
- Introduction To Major Crop FieldsDocument32 pagesIntroduction To Major Crop FieldsCHANDANINo ratings yet
- The Stolen EaglesDocument12 pagesThe Stolen EaglesJavier Horacio FernandezNo ratings yet
- Newnew 151 ModelDocument1 pageNewnew 151 ModelCrestine Lily DongosaNo ratings yet
- Get started with Power BI DesktopDocument34 pagesGet started with Power BI Desktopbhargavc7No ratings yet
- Wiz107sr User Manual en v1.0Document29 pagesWiz107sr User Manual en v1.0Pauli Correa ArriagadaNo ratings yet
- Template For Preparing TANSCST ProposalDocument6 pagesTemplate For Preparing TANSCST ProposalAntony88% (8)
- Ansys Workbench Tutorial: Structural & Thermal Analysis Using The ANSYS Workbench Release 11.0 EnvironmentDocument5 pagesAnsys Workbench Tutorial: Structural & Thermal Analysis Using The ANSYS Workbench Release 11.0 EnvironmentMuhammad HaroonNo ratings yet
- App Cache 133069888033757953Document46 pagesApp Cache 133069888033757953akunkelasdNo ratings yet
- How Nokia Failed to Adapt to Market ChangesDocument5 pagesHow Nokia Failed to Adapt to Market ChangesRiangelli ExcondeNo ratings yet
- Nitro - Quiz 3 Ged102-A13Document3 pagesNitro - Quiz 3 Ged102-A13Eliezer NitroNo ratings yet
- Event Management Study Material Free PDFDocument2 pagesEvent Management Study Material Free PDFKim0% (1)
- ChecklistDocument2 pagesChecklistKyra AlesonNo ratings yet
- Jurnal Tentang Akuntansi Dengan Metode Kualitatif IDocument8 pagesJurnal Tentang Akuntansi Dengan Metode Kualitatif IAfni FebrianaNo ratings yet
- Drive Unit TENH EH 10003, 225, 50/60Hz 400/440V: Qty. Description Specification Material Size DT Doc IdDocument1 pageDrive Unit TENH EH 10003, 225, 50/60Hz 400/440V: Qty. Description Specification Material Size DT Doc IdKarikalan JayNo ratings yet
- Senate Bill 365Document5 pagesSenate Bill 365samtlevinNo ratings yet
- MSCL PipeDocument9 pagesMSCL PipeAhmad Zakwan Asmad100% (1)
- PRINCIPLES OF MANAGEMENT Model Questions - ADocument4 pagesPRINCIPLES OF MANAGEMENT Model Questions - ALionel MintsaNo ratings yet
- Manual SOC2 DVR Mini 90nDocument83 pagesManual SOC2 DVR Mini 90nDeybby Luna Laredo0% (1)
- Detect Body Temperature and Abnormalities with Thermal CameraDocument5 pagesDetect Body Temperature and Abnormalities with Thermal CameraPeter ShingNo ratings yet