You might also like
- TIH COVID Guideline AdultDocument24 pagesTIH COVID Guideline AdultMr MWSKNo ratings yet
- MoHP Protocol For COVID19 November 2020Document28 pagesMoHP Protocol For COVID19 November 2020medya dostorNo ratings yet
- Penatalaksanaan Keperawatan Covid 19 Di Respiratory Ward AustraliaDocument22 pagesPenatalaksanaan Keperawatan Covid 19 Di Respiratory Ward AustraliaRadenroro Atih Utari RizkyNo ratings yet
- DM 2020-0439 "Omnibus Interim Guidelines On Prevention, Detection, Isolation, Treatment, and Reintegration Strategies For COVID-19"Document55 pagesDM 2020-0439 "Omnibus Interim Guidelines On Prevention, Detection, Isolation, Treatment, and Reintegration Strategies For COVID-19"Seriel TismoNo ratings yet
- Management Cases Contacts OmicronDocument17 pagesManagement Cases Contacts OmicronCarlos DuqueNo ratings yet
- COVID-19 MoHP Protocol May 2020Document14 pagesCOVID-19 MoHP Protocol May 2020BARAKA ROKANo ratings yet
- Guidance on prioritising PPE during COVID-19Document3 pagesGuidance on prioritising PPE during COVID-19MN IrshadNo ratings yet
- COVID-Referral Pathway With Temporary COVID-19 ITC 280320 - ForsharingDocument3 pagesCOVID-Referral Pathway With Temporary COVID-19 ITC 280320 - ForsharingSaima Binte IkramNo ratings yet
- Module 3 Triage SARIDocument26 pagesModule 3 Triage SARIEstefania Cuta HernandezNo ratings yet
- Setting up Effective Triage and Isolation Areas in Healthcare FacilitiesDocument16 pagesSetting up Effective Triage and Isolation Areas in Healthcare FacilitiesrohitNo ratings yet
- Fever Clinic SOPDocument4 pagesFever Clinic SOPJery JsNo ratings yet
- COVID-19 ER Clinical Pathway: Registration or Triage NurseDocument2 pagesCOVID-19 ER Clinical Pathway: Registration or Triage NurseBassam AlqadasiNo ratings yet
- Covid in PregnancyDocument30 pagesCovid in Pregnancyvidhi chaudharyNo ratings yet
- Quarantine and isolation protocols for COVID-19 managementDocument13 pagesQuarantine and isolation protocols for COVID-19 managementRyan Paul PastoleroNo ratings yet
- DOH Memorandum 2020-0178Document7 pagesDOH Memorandum 2020-0178Raffy BelloNo ratings yet
- INFORMATION SHEET 1. - Risk Categorisation Guidelines: Protection Against The Specified Infectious Diseases Is RequiredDocument4 pagesINFORMATION SHEET 1. - Risk Categorisation Guidelines: Protection Against The Specified Infectious Diseases Is RequiredjacksonzchenNo ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- Managing COVID-19 Cases in the CommunityDocument18 pagesManaging COVID-19 Cases in the CommunityElteyb Nor eldaimNo ratings yet
- SISTEM TRIAGE - Dr. Mirza, SP - An, FIPM, FIPPDocument34 pagesSISTEM TRIAGE - Dr. Mirza, SP - An, FIPM, FIPPlittle sunflowerfieldNo ratings yet
- STRENGTHENING COMMUNITY SURVEILLANCE FOR COVID-19Document24 pagesSTRENGTHENING COMMUNITY SURVEILLANCE FOR COVID-19didilajnNo ratings yet
- Covid-19 Infection in Pregnancy: Dr. Asmita Pantha 3 Year Resident Department of OBGYN KusmsDocument61 pagesCovid-19 Infection in Pregnancy: Dr. Asmita Pantha 3 Year Resident Department of OBGYN Kusmsshrinkhala bhattaraiNo ratings yet
- COVID-19 Protocol July 2022Document36 pagesCOVID-19 Protocol July 2022Mobile AsdNo ratings yet
- MODIFIED COVID-19 REFERRAL FLOWCHARTDocument1 pageMODIFIED COVID-19 REFERRAL FLOWCHARTJohnPaulOliverosNo ratings yet
- PSMID Guidelines COVID 19 - EditedDocument8 pagesPSMID Guidelines COVID 19 - EditedIsrael H. ZantuaNo ratings yet
- WHO 2019 nCoV Surveillance - Case - Definition 2020.1 EngDocument1 pageWHO 2019 nCoV Surveillance - Case - Definition 2020.1 EngAkbar FikriNo ratings yet
- Annex 1: Ministry of Health Malaysia Updated On 22 April 2021 1Document3 pagesAnnex 1: Ministry of Health Malaysia Updated On 22 April 2021 1Lau LauNo ratings yet
- PHC ILI Guidlines COVID-19 FinalDocument4 pagesPHC ILI Guidlines COVID-19 Finalyalmas ugloNo ratings yet
- MANAGING PUIDocument4 pagesMANAGING PUIRosly BiunNo ratings yet
- Bu BudiDocument32 pagesBu Budinoi javuNo ratings yet
- COVID-19 SOP for Subcontractor as of June 17,2022Document11 pagesCOVID-19 SOP for Subcontractor as of June 17,2022lukmanNo ratings yet
- Saint - Lucia COVID-19 Community ManagenentDocument18 pagesSaint - Lucia COVID-19 Community ManagenentOqba AlzwainyNo ratings yet
- COVID-19 Guidelines For Renal Dialysis: 10 February 2022Document19 pagesCOVID-19 Guidelines For Renal Dialysis: 10 February 2022zulfiqarNo ratings yet
- Orientation On Monkeypox For Community PartnersDocument16 pagesOrientation On Monkeypox For Community PartnersNQ ZNo ratings yet
- Labor Room Managementduring Covid19-5Document78 pagesLabor Room Managementduring Covid19-5Kalyani RathNo ratings yet
- Penatalaksanaan Petugas Terpapar COVID-19Document30 pagesPenatalaksanaan Petugas Terpapar COVID-19Taupick ArsyNo ratings yet
- Covid Antiviral Medications How To Prescribe Mar 10 2022Document38 pagesCovid Antiviral Medications How To Prescribe Mar 10 2022ABDULLAH SDNo ratings yet
- Covid PathwayDocument37 pagesCovid PathwayMadhavi ModaNo ratings yet
- Case Defination - Covid19Document1 pageCase Defination - Covid19محمد ابراهيمNo ratings yet
- Triage Process of COVID 19: All Other Normal Patient Go With The Routing Number Order and TreatmentDocument3 pagesTriage Process of COVID 19: All Other Normal Patient Go With The Routing Number Order and TreatmentGihan SampathNo ratings yet
- Mitigation Response To Influenza A (H1N1) - v2Document24 pagesMitigation Response To Influenza A (H1N1) - v2gem_jae02No ratings yet
- COVID 19 FactsDocument27 pagesCOVID 19 FactsgjpaqueoNo ratings yet
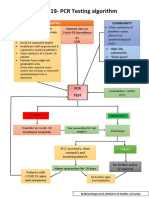
- CovidpcrtestingalgorithmDocument1 pageCovidpcrtestingalgorithmMWNo ratings yet
- Manage infants under 28 days with COVID-19 in NICUDocument1 pageManage infants under 28 days with COVID-19 in NICUCHIERBEENo ratings yet
- SOP Triage Suspected CovidDocument29 pagesSOP Triage Suspected CovidRoy Tanda Anugrah SihotangNo ratings yet
- Annex 2 Management of Pui and Confirmed Covid-19 Case 1. Admission CriteriaDocument7 pagesAnnex 2 Management of Pui and Confirmed Covid-19 Case 1. Admission CriteriaDamin FyeNo ratings yet
- Child With Fever in ER Non Covid 19Document6 pagesChild With Fever in ER Non Covid 19Suwandi AlghozyNo ratings yet
- The Following Guidelines Must Be Implemented:: Omicron VariantDocument13 pagesThe Following Guidelines Must Be Implemented:: Omicron VariantLdrrmo RamonNo ratings yet
- Covid19 Antigen LectureDocument20 pagesCovid19 Antigen LectureUSI- CAMANO, JAY C.No ratings yet
- Quiz Core Uc2 and Uc3Document2 pagesQuiz Core Uc2 and Uc3Ghe marNo ratings yet
- Guía Rápida StanfordDocument6 pagesGuía Rápida StanfordDr. Victor Adolfo RochaNo ratings yet
- 1.nurse Preparedness Training Against 3rd Wave of CovidDocument52 pages1.nurse Preparedness Training Against 3rd Wave of CovidyeshumasihNo ratings yet
- Aden Covid-19 Protocol 26-5-2020 (ASIA) 22-1Document14 pagesAden Covid-19 Protocol 26-5-2020 (ASIA) 22-1محمدرزازالتبعيNo ratings yet
- MOHW COVID-19 Draft Discharge Protocol From Isolation Facilities-V 6 December 2021) ) DcsDocument9 pagesMOHW COVID-19 Draft Discharge Protocol From Isolation Facilities-V 6 December 2021) ) DcsAriel E. Delgado RodriguezNo ratings yet
- Final Redbook External CirculationDocument155 pagesFinal Redbook External CirculationdocsaravananNo ratings yet
- John Taylor Case Study ENP and EPPDocument11 pagesJohn Taylor Case Study ENP and EPPAhata Sham NewazNo ratings yet
- POGS-PSMFM Interim Guidelines On Labor and Delivery For COVID EditedDocument20 pagesPOGS-PSMFM Interim Guidelines On Labor and Delivery For COVID EditedMacky YongcoNo ratings yet
- Recommendations For Covid 19 PCR TestingDocument4 pagesRecommendations For Covid 19 PCR TestingDipa Zoda Helfando100% (1)
- Probable Case of Sars-Cov-2 Infection A B C DDocument1 pageProbable Case of Sars-Cov-2 Infection A B C Dkezivana10No ratings yet
- Lessons From Wuhan COVID 19 03 12 2020 - RevisedDocument51 pagesLessons From Wuhan COVID 19 03 12 2020 - RevisedZishanNo ratings yet
- Sexual Orientation, Gender Identity and Expression: "Toni Gee"Document21 pagesSexual Orientation, Gender Identity and Expression: "Toni Gee"Lapuyan Rural Health UnitNo ratings yet
- Municipal Ordinance Bans Smoking in Public PlacesDocument11 pagesMunicipal Ordinance Bans Smoking in Public PlacesLapuyan Rural Health UnitNo ratings yet
- 6 Strategic PlanningDocument10 pages6 Strategic PlanningLapuyan Rural Health UnitNo ratings yet
- Mission and Vision Values, Goals and ObjectivesDocument18 pagesMission and Vision Values, Goals and ObjectivesLapuyan Rural Health UnitNo ratings yet
- Zep 14624Document4 pagesZep 14624Jorge AguirreNo ratings yet
- Therapeutic Modal: Automatic Rotating Pronation Beds: Name Institutional Affiliation Course Instructor DateDocument8 pagesTherapeutic Modal: Automatic Rotating Pronation Beds: Name Institutional Affiliation Course Instructor DateErick kiraguNo ratings yet
- CPR MFR Internal F&R ChallengeDocument13 pagesCPR MFR Internal F&R Challengedwi rahwatiNo ratings yet
- Cyanide Fact Sheet 7-22-04Document4 pagesCyanide Fact Sheet 7-22-04Izzati HanisNo ratings yet
- MASTERY TEST 1 MedSurgDocument11 pagesMASTERY TEST 1 MedSurgHan NahNo ratings yet
- Barang Mendekati Ed 2024Document4 pagesBarang Mendekati Ed 2024Tesa Yuli DenisaNo ratings yet
- Parental Consent and Waiver FormDocument1 pageParental Consent and Waiver FormNicole J. CentenoNo ratings yet
- CPR PPT FinalDocument83 pagesCPR PPT FinalSimran Josan100% (1)
- Occupational Lung Disease. Diagnosis and Communication - Fact or Fiction?Document1 pageOccupational Lung Disease. Diagnosis and Communication - Fact or Fiction?Zali AhmadNo ratings yet
- Angelbiss ManualDocument51 pagesAngelbiss ManualSineepa PLOYNo ratings yet
- Klüber Klübersynth Gem 4-220 N Msds enDocument9 pagesKlüber Klübersynth Gem 4-220 N Msds enJadou RzkNo ratings yet
- Resmed - Vpap-Iv ST User-GuideDocument24 pagesResmed - Vpap-Iv ST User-GuideJef RobboNo ratings yet
- Bronchial Hygiene or Airway Clearance TechniquesDocument139 pagesBronchial Hygiene or Airway Clearance TechniquesPiyush Salgaonkar100% (1)
- PTB Case-StudyDocument64 pagesPTB Case-StudyBeverly DatuNo ratings yet
- Focus Charting (F-DAR) : How To Do Focus Charting or F-DAR: Matt Vera, BSN, R.NDocument10 pagesFocus Charting (F-DAR) : How To Do Focus Charting or F-DAR: Matt Vera, BSN, R.NShiena Mae PelagioNo ratings yet
- CT Evaluation of Congenital and AcquiredDocument14 pagesCT Evaluation of Congenital and AcquiredChavdarNo ratings yet
- Survanta PiDocument10 pagesSurvanta PiBas BaylonNo ratings yet
- TracheostomyDocument29 pagesTracheostomyFemi AustinNo ratings yet
- Sodium HexametaphosphateDocument7 pagesSodium Hexametaphosphatekim verdanaNo ratings yet
- Module 12 - Health Conditions RajDocument6 pagesModule 12 - Health Conditions RajRajesh MakwanaNo ratings yet
- Airway ManagementDocument106 pagesAirway ManagementAna-Maria BotarNo ratings yet
- Ventilador Mekics PDFDocument4 pagesVentilador Mekics PDFBalam CaballeroNo ratings yet
- Risk Factors For Severe COVID 19Document3 pagesRisk Factors For Severe COVID 19drsaleemNo ratings yet
- 6b. XII - MIPA - PROCEDURE TEXT - SSDocument5 pages6b. XII - MIPA - PROCEDURE TEXT - SSMuhammad Zidan IlhamiNo ratings yet
- Material Safety Data Sheet: 1. Chemical Product and Company IdentificationDocument11 pagesMaterial Safety Data Sheet: 1. Chemical Product and Company Identificationabdulrahman abduNo ratings yet
- AUTOSOL - Chrome & Metal Polish - EXP Aug 2025Document5 pagesAUTOSOL - Chrome & Metal Polish - EXP Aug 2025brianNo ratings yet
- Antimonium TartaricumDocument5 pagesAntimonium TartaricumSuhas IngaleNo ratings yet
- Prepared By:: Nisha Ghimire Sushmita Poudel Aliza Poudel Devi Rana Namuna KarkiDocument33 pagesPrepared By:: Nisha Ghimire Sushmita Poudel Aliza Poudel Devi Rana Namuna KarkiPerry BearNo ratings yet
- INSTRUMENTS For UGDocument22 pagesINSTRUMENTS For UGPugazhenthi CNo ratings yet
- P1 RleDocument34 pagesP1 RleMary Jean GicaNo ratings yet