You might also like
- Anesthesia For Genitourinary SurgeryDocument76 pagesAnesthesia For Genitourinary SurgeryWenny Eka FildayantiNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Pediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderFrom EverandPediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderNo ratings yet
- Anesthesia: A Topical Update – Thoracic, Cardiac, Neuro, ICU, and Interesting CasesFrom EverandAnesthesia: A Topical Update – Thoracic, Cardiac, Neuro, ICU, and Interesting CasesRating: 5 out of 5 stars5/5 (1)
- Preoperative Patient Assessment and Management: Roxanne Jeen L. FornollesDocument61 pagesPreoperative Patient Assessment and Management: Roxanne Jeen L. FornollesRyan FornollesNo ratings yet
- Fred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008Document53 pagesFred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008lmjeksoreNo ratings yet
- Complications of Spinal and Epidural AnesthesiaDocument45 pagesComplications of Spinal and Epidural AnesthesiashikhaNo ratings yet
- Anaesthetic Management in Laparoscopic SurgeriesDocument39 pagesAnaesthetic Management in Laparoscopic SurgeriesRaguNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Pediatric Anesthesiology Review: Clinical Cases for Self-AssessmentFrom EverandPediatric Anesthesiology Review: Clinical Cases for Self-AssessmentNo ratings yet
- Ambulatory Anaesthesia 97 1234Document58 pagesAmbulatory Anaesthesia 97 1234drsachin_uc75520% (1)
- Evidence-Based Obstetric AnesthesiaFrom EverandEvidence-Based Obstetric AnesthesiaStephen H. HalpernNo ratings yet
- Anesthesia Management For Laparoscpic SurgeryDocument33 pagesAnesthesia Management For Laparoscpic Surgerymichael0% (1)
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- Anaesthesia For Thyroid Surgery....Document46 pagesAnaesthesia For Thyroid Surgery....Parvathy R NairNo ratings yet
- AWARENESS UNDER ANESTHESIA: DEFINITION, TYPES, RISK FACTORS & PREVENTIONDocument27 pagesAWARENESS UNDER ANESTHESIA: DEFINITION, TYPES, RISK FACTORS & PREVENTIONagatakassaNo ratings yet
- Anesthesia For Bariatric SurgeryDocument47 pagesAnesthesia For Bariatric Surgerydkhiloi100% (1)
- Managing Difficult Airway in Obstetric AnesthesiaDocument3 pagesManaging Difficult Airway in Obstetric AnesthesiaRoman AureliaNo ratings yet
- Epidural Anatomy & PhysiologyDocument14 pagesEpidural Anatomy & PhysiologyAbel AxelNo ratings yet
- Graphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaFrom EverandGraphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaNo ratings yet
- Awareness in Anesthesia FinalisedDocument42 pagesAwareness in Anesthesia FinalisedLean CyNo ratings yet
- Anaesthesia Explained PDFDocument22 pagesAnaesthesia Explained PDFaksinu100% (1)
- Anesthesia For Day Care SurgeryDocument60 pagesAnesthesia For Day Care Surgerymedico_bhalla93% (15)
- Race 2019Document418 pagesRace 2019Sadia KhanNo ratings yet
- General Anesthesia - Induction - UpToDateDocument14 pagesGeneral Anesthesia - Induction - UpToDateTania Parra MoralesNo ratings yet
- Neuraxial Anaesthesia: DR Ali Rahman Assistant Professor - Anaesthesiology Department (RMDC)Document27 pagesNeuraxial Anaesthesia: DR Ali Rahman Assistant Professor - Anaesthesiology Department (RMDC)fahadali2000No ratings yet
- Anesthesia For ElderlyDocument27 pagesAnesthesia For ElderlyApril Joy CalayagNo ratings yet
- REGIONAL ANESTHESIA TECHNIQUESDocument36 pagesREGIONAL ANESTHESIA TECHNIQUESMay Anne BuenafeNo ratings yet
- Anesthesia PresentationDocument19 pagesAnesthesia PresentationJohnyNo ratings yet
- Context Sensitive Half Time (CSHT) - The Lay Medical ManDocument3 pagesContext Sensitive Half Time (CSHT) - The Lay Medical Manpradeep danielNo ratings yet
- Anesthesia For Laparoscopic SurgeryDocument38 pagesAnesthesia For Laparoscopic SurgeryMohamed Satti AbdalsadigNo ratings yet
- Physics principles for anesthesiologistsDocument97 pagesPhysics principles for anesthesiologistszeedansmNo ratings yet
- Failed Spinal AnaesthesiaDocument10 pagesFailed Spinal Anaesthesian12345678n100% (1)
- Anesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaDocument3 pagesAnesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaJhevilin RMNo ratings yet
- Day Care AnesthesiaDocument68 pagesDay Care AnesthesiaSri Sruthi PichikaNo ratings yet
- Epidural AnaesthesiaDocument13 pagesEpidural AnaesthesiajuniorebindaNo ratings yet
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- Conduct of AnaesthesiaDocument30 pagesConduct of AnaesthesiaAnirban PalNo ratings yet
- Obestetrics GynecologyDocument203 pagesObestetrics GynecologySwamynadh Gandhi ReddiNo ratings yet
- ANESTHESIA-Pediatrics Airway SyndromesDocument12 pagesANESTHESIA-Pediatrics Airway SyndromeshollyuNo ratings yet
- Regional Anesthesia - FinalDocument46 pagesRegional Anesthesia - Finalvan016_bunnyNo ratings yet
- Day Case Anaesthesia - My Presentation.Document62 pagesDay Case Anaesthesia - My Presentation.roselinekhadija100% (4)
- Joint Replacement Anesthesia ManagementDocument55 pagesJoint Replacement Anesthesia ManagementRaguNo ratings yet
- Brachial Plexus Block TechniquesDocument13 pagesBrachial Plexus Block TechniquesAnkit Shah100% (1)
- NMJ Blocking Agents GuideDocument69 pagesNMJ Blocking Agents Guidevvb_frndNo ratings yet
- Thsesis TopicsDocument17 pagesThsesis Topicsvvb_frndNo ratings yet
- Factors Affectin Block HeightDocument37 pagesFactors Affectin Block HeightshikhaNo ratings yet
- Pediatric AnesthesiaDocument15 pagesPediatric Anesthesiamichael100% (6)
- Anesthesia Considerations For Neuromuscular DiseaseDocument42 pagesAnesthesia Considerations For Neuromuscular Diseasesamrox54No ratings yet
- Basic Pharmacology of Anesthesia DrugsDocument42 pagesBasic Pharmacology of Anesthesia Drugsansuh22100% (1)
- Anesthetic Consideration in Hypertensive PatientDocument11 pagesAnesthetic Consideration in Hypertensive PatientYosiAsmaraNo ratings yet
- Thoraxic Region Nerve Block - ESADocument35 pagesThoraxic Region Nerve Block - ESAMaraNo ratings yet
- Spinal Anesthesia - Technique - UpToDateDocument37 pagesSpinal Anesthesia - Technique - UpToDateSamir Perez CasadiegoNo ratings yet
- Anesthesia Machine: Ventilator, Vaporizer & Scavenging SystemDocument76 pagesAnesthesia Machine: Ventilator, Vaporizer & Scavenging SystemMohmmed MousaNo ratings yet
- Management of Antithrombotic Therapy For Neuraxial and Peripheral Nerve ProceduresDocument3 pagesManagement of Antithrombotic Therapy For Neuraxial and Peripheral Nerve Proceduresjojobod100% (1)
- Paediatric Anaesthesia PDFDocument33 pagesPaediatric Anaesthesia PDFMarcelitaTaliaDuwiriNo ratings yet
- AnaesthesiaDocument44 pagesAnaesthesiamadmaxmaxmus50% (2)
- Anaesthesia in Obese PatientsDocument72 pagesAnaesthesia in Obese PatientsPraveen RamasamyNo ratings yet
- Epidural AnesthesiaDocument5 pagesEpidural AnesthesiaImran MukhlessNo ratings yet
- I STATDocument24 pagesI STATPraveen RamasamyNo ratings yet
- Neonatal Resuscitation: Presented By: Dr. Harish Uppala Chairperson: Dr. Kousalya Moderator: Dr. HemnathDocument23 pagesNeonatal Resuscitation: Presented By: Dr. Harish Uppala Chairperson: Dr. Kousalya Moderator: Dr. HemnathPraveen RamasamyNo ratings yet
- Physiology of One Lung Ventilation Technique (OLVDocument59 pagesPhysiology of One Lung Ventilation Technique (OLVPraveen RamasamyNo ratings yet
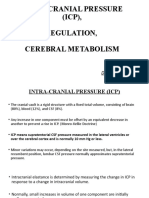
- Managing Intracranial Pressure (ICP) Through Cerebral Metabolism RegulationDocument18 pagesManaging Intracranial Pressure (ICP) Through Cerebral Metabolism RegulationPraveen RamasamyNo ratings yet
- Antifibrinolytic Therapy For Y2K+1: Ray Tople, M.D. Anesthesia and Operative Service BamcDocument34 pagesAntifibrinolytic Therapy For Y2K+1: Ray Tople, M.D. Anesthesia and Operative Service BamcPraveen RamasamyNo ratings yet
- Aortic StenosisDocument19 pagesAortic StenosisPraveen RamasamyNo ratings yet
- Aortic StenosisDocument19 pagesAortic StenosisPraveen RamasamyNo ratings yet
- Neuraxial Analgesia & Anticoagulation: Charles E Smith MDDocument53 pagesNeuraxial Analgesia & Anticoagulation: Charles E Smith MDPraveen RamasamyNo ratings yet
- Antico Agne Ur AxialDocument27 pagesAntico Agne Ur AxialPraveen RamasamyNo ratings yet
- Neuraxial Analgesia & Anticoagulation: Charles E Smith MDDocument53 pagesNeuraxial Analgesia & Anticoagulation: Charles E Smith MDPraveen RamasamyNo ratings yet
- Antico Agne Ur AxialDocument27 pagesAntico Agne Ur AxialPraveen RamasamyNo ratings yet
- Antifibrinolytic Therapy for Cardiothoracic SurgeryDocument34 pagesAntifibrinolytic Therapy for Cardiothoracic SurgeryPraveen RamasamyNo ratings yet
- Anaesthetic Challenges in Complex Maxillofacial Trauma - ADocument18 pagesAnaesthetic Challenges in Complex Maxillofacial Trauma - APraveen RamasamyNo ratings yet
- Anesthesia For Neurosurg2Document42 pagesAnesthesia For Neurosurg2Praveen RamasamyNo ratings yet
- Anaesthesia in Obese PatientsDocument72 pagesAnaesthesia in Obese PatientsPraveen RamasamyNo ratings yet
- NsaidsDocument3 pagesNsaidsShayan ShayanNo ratings yet
- Ischemic Heart Disease 19.9.90Document27 pagesIschemic Heart Disease 19.9.90Hamidreza GoodarzynejadNo ratings yet
- PHARMACOLOGYDocument36 pagesPHARMACOLOGYjanr123456100% (1)
- Web EIJ223 V19i1 May2023 FiligraneDocument105 pagesWeb EIJ223 V19i1 May2023 FiligraneChay AlcantaraNo ratings yet
- Tranexamic Acid 500mg IV q8Document3 pagesTranexamic Acid 500mg IV q8Anjeleeka OcampoNo ratings yet
- Flfghfuid Elefghgfhctrolytes Cheat SheetDocument1 pageFlfghfuid Elefghgfhctrolytes Cheat SheetRăzvan RoșcaNo ratings yet
- Understanding your blood test resultsDocument5 pagesUnderstanding your blood test resultsAhmed Tolba0% (1)
- INTRODUCTION A Cerebrovascular Accident (CVA), An Ischemic Stroke or "BrainDocument30 pagesINTRODUCTION A Cerebrovascular Accident (CVA), An Ischemic Stroke or "BrainCherie May100% (5)
- Peritonitis and Abdominal Sepsis: Background, Anatomy, PathophysiologyDocument16 pagesPeritonitis and Abdominal Sepsis: Background, Anatomy, PathophysiologyTias SubagioNo ratings yet
- Download ebook Atlas Of Retinal Oct Optical Coherence Tomography Pdf full chapter pdfDocument67 pagesDownload ebook Atlas Of Retinal Oct Optical Coherence Tomography Pdf full chapter pdfcharles.schmidt276100% (24)
- Health Impact of Air PollutionDocument15 pagesHealth Impact of Air Pollutionapi-304969581No ratings yet
- Cardiac Monitoring Pocket CardDocument2 pagesCardiac Monitoring Pocket Cardpurplefeather_14100% (1)
- Unit 7 Cardiac (S)Document78 pagesUnit 7 Cardiac (S)Cheyenne SchimpfNo ratings yet
- Magdy El-Masry Prof. of Cardiology Tanta UniversityDocument55 pagesMagdy El-Masry Prof. of Cardiology Tanta UniversityPrabJot SinGhNo ratings yet
- Dual Antiplatelet Therapy Vs Alteplase For Patients With Minor NondisablingDocument10 pagesDual Antiplatelet Therapy Vs Alteplase For Patients With Minor Nondisablingbetongo Bultus Ocultus XVNo ratings yet
- Hypertensive Heart Disease: A Proposed Clinical ClassificationDocument2 pagesHypertensive Heart Disease: A Proposed Clinical ClassificationireneaureliaNo ratings yet
- Diabetic Patient With Liver DiseaseDocument17 pagesDiabetic Patient With Liver DiseaseSiti Ika FitrasyahNo ratings yet
- 2020 Article 479Document5 pages2020 Article 479Anida HasnaNo ratings yet
- Lung Ultrasound Made Easy Step-By-Step GuideDocument48 pagesLung Ultrasound Made Easy Step-By-Step GuideEL SHITA100% (1)
- AHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementDocument38 pagesAHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementPratik TripathiNo ratings yet
- The Morning Blood Pressure Surge: A Dynamic and Challenging ConceptDocument4 pagesThe Morning Blood Pressure Surge: A Dynamic and Challenging ConceptneilNo ratings yet
- Nursing Care of Clients Before and After CABGDocument46 pagesNursing Care of Clients Before and After CABGshejila c hNo ratings yet
- Underwriting Cheat Sheet For WMDocument106 pagesUnderwriting Cheat Sheet For WMAleah DatukonNo ratings yet
- Hemolytic Anemia IntrinsicDocument14 pagesHemolytic Anemia IntrinsicSophia Gail ChingNo ratings yet
- DiltiazemDocument2 pagesDiltiazemE100% (1)
- MCN Lec - 2ND SemDocument29 pagesMCN Lec - 2ND SemALYSSA NICOLE GINESNo ratings yet
- Health Assessment ChecklistDocument14 pagesHealth Assessment ChecklistLindy JaneNo ratings yet
- Neuro SensoryDocument37 pagesNeuro Sensorybill jonsNo ratings yet
- MNG - D1 - 1. Clinical Guideline of Acute Stroke (WHO)Document42 pagesMNG - D1 - 1. Clinical Guideline of Acute Stroke (WHO)Shelin ClarissaNo ratings yet
- Acute Kidney InjuryDocument64 pagesAcute Kidney InjuryBIAN ALKHAZMARINo ratings yet