You might also like
- Cellinjury 151004125508 Lva1 App6892Document147 pagesCellinjury 151004125508 Lva1 App6892Ajmal RockzzNo ratings yet
- Cellular Injury and AdaptationsDocument145 pagesCellular Injury and AdaptationsAjmal RockzzNo ratings yet
- Atrophy, Metaplasia, Cloudy Swelling 13.6.2014 CDocument21 pagesAtrophy, Metaplasia, Cloudy Swelling 13.6.2014 CPradeepNo ratings yet
- Cell Injury and AdaptationDocument18 pagesCell Injury and AdaptationNazneen ShawarNo ratings yet
- Introduction To Basic Pathology - 09.08.2023.ppt-1Document31 pagesIntroduction To Basic Pathology - 09.08.2023.ppt-1Abdur RaquibNo ratings yet
- Cellular Adaptations & Growth DisturbancesDocument27 pagesCellular Adaptations & Growth DisturbancesJames MubitahNo ratings yet
- ADAPTATIONSDocument32 pagesADAPTATIONSMahalakshmi PalanisamiNo ratings yet
- Patho-Physiology: TopicsDocument13 pagesPatho-Physiology: TopicsDURJOYNo ratings yet
- Cellular Adaptation - 2022Document49 pagesCellular Adaptation - 2022Leo Lucifer 104No ratings yet
- 6 CellularAdaptationsDocument87 pages6 CellularAdaptationsMaria MoiseencuNo ratings yet
- Lect 2 Patho SentDocument79 pagesLect 2 Patho SentPuranjay ChandelNo ratings yet
- 1 Cellular AdaptationDocument17 pages1 Cellular AdaptationReetu BaralNo ratings yet
- Cell InjuryDocument132 pagesCell InjuryAboubakar Moalim Mahad moh'dNo ratings yet
- Cell Adaptation, Injury, and DeathDocument48 pagesCell Adaptation, Injury, and DeathRizka SukmasariNo ratings yet
- Necrosis and Cellualr AdaptationDocument56 pagesNecrosis and Cellualr AdaptationEs SarveshNo ratings yet
- Cellular Adaptations and Accumulations SummaryDocument30 pagesCellular Adaptations and Accumulations Summaryzaina bookshopNo ratings yet
- 5 Adaptations&AccumulationsDocument31 pages5 Adaptations&AccumulationsDuha YousefNo ratings yet
- Cellular adaptationDocument63 pagesCellular adaptationashm1672No ratings yet
- Cellular changes in atrophy, hypertrophy, hyperplasia, metaplasia and dysplasiaDocument11 pagesCellular changes in atrophy, hypertrophy, hyperplasia, metaplasia and dysplasiaKiranNo ratings yet
- 1 Cellular Response To Injury 1Document33 pages1 Cellular Response To Injury 1Alex XanderNo ratings yet
- NewGeneral Pathology2Document305 pagesNewGeneral Pathology2Tahir AzizNo ratings yet
- Introduction To Pathology 02Document66 pagesIntroduction To Pathology 02sunday danielNo ratings yet
- PathologyDocument119 pagesPathologyDavid VijayNo ratings yet
- Cellular AdaptationDocument14 pagesCellular AdaptationAsmaNo ratings yet
- General Pathology: Cell Injury, Adaptation and NecrosisDocument305 pagesGeneral Pathology: Cell Injury, Adaptation and NecrosisTahir AzizNo ratings yet
- Cell Adaptation Types: Atrophy, Hypertrophy & HyperplasiaDocument57 pagesCell Adaptation Types: Atrophy, Hypertrophy & HyperplasiaMani JeeNo ratings yet
- Cell Adaptation: Gul Fatima/R.Ph Lecturer, SICPDocument38 pagesCell Adaptation: Gul Fatima/R.Ph Lecturer, SICPMani JeeNo ratings yet
- Cell Adaptation For Presentation by G-3Document25 pagesCell Adaptation For Presentation by G-3Misael BeleteNo ratings yet
- Altered Cell Biology: PathophysiologyDocument33 pagesAltered Cell Biology: PathophysiologyNi CaoNo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular Adaptationshaddi awanNo ratings yet
- Degenerative ChangesDocument45 pagesDegenerative ChangesAbhishek JhaNo ratings yet
- Pathology (3) Adaptation and Cellular DepostitionDocument50 pagesPathology (3) Adaptation and Cellular Depostitionnurul dwi ratihNo ratings yet
- 4-Hyperplasia Part 2-1Document48 pages4-Hyperplasia Part 2-1Ali GamalNo ratings yet
- Pathology Cell InjuryDocument57 pagesPathology Cell InjuryMajd MustafaNo ratings yet
- Cell Damage - 1 - N (3)Document48 pagesCell Damage - 1 - N (3)Sultan SalmanNo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular AdaptationsElena PoriazovaNo ratings yet
- Cellular responses to stress and toxic insultsDocument29 pagesCellular responses to stress and toxic insultsMK100% (1)
- Cell Adaptation: Presenter Amon Facilitator Prof Amos MwakigonjaDocument26 pagesCell Adaptation: Presenter Amon Facilitator Prof Amos MwakigonjaNtobi ThomasNo ratings yet
- Cellular Adaptation To StressDocument31 pagesCellular Adaptation To StressMuhammad Umar QureshiNo ratings yet
- Hyperplasia and HypertrophyDocument16 pagesHyperplasia and HypertrophyPradeepNo ratings yet
- SHS 301 Lect-2Document29 pagesSHS 301 Lect-2AAZEEN ALINo ratings yet
- Cellular Adaptation and Cell InjuryDocument99 pagesCellular Adaptation and Cell Injuryyohannes adebabayNo ratings yet
- Adaptation of Cellular Growth & Differentiation: Presented By: Dr. Hrudi Sundar SahooDocument28 pagesAdaptation of Cellular Growth & Differentiation: Presented By: Dr. Hrudi Sundar SahooEdsel Ian S. FuentesNo ratings yet
- Cellular AdaptationsDocument19 pagesCellular AdaptationssnehagptNo ratings yet
- Cellular AdaptationsDocument18 pagesCellular Adaptationspanditji0294No ratings yet
- Cellular Response To Stress and Noxious StimuliDocument31 pagesCellular Response To Stress and Noxious StimuliWinda Syahfitri HasibuanNo ratings yet
- Lesson 1 - Cell InjuryDocument69 pagesLesson 1 - Cell InjuryAY 700No ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular AdaptationsVirli AnaNo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular AdaptationsAya KinugasaNo ratings yet
- Cellular Adaptations in Growth and DifferentiationDocument32 pagesCellular Adaptations in Growth and Differentiationvinoedhnaidu_rajagopalNo ratings yet
- Pathology Slides 2023 (B&B) [Medicalstudyzone.com]Document249 pagesPathology Slides 2023 (B&B) [Medicalstudyzone.com]Carol de AndradeNo ratings yet
- PATHOPHYSIOLOGYDocument27 pagesPATHOPHYSIOLOGYBhavya agarwalNo ratings yet
- 1 - Cellular AdaptationsDocument62 pages1 - Cellular Adaptationsaimi BatrisyiaNo ratings yet
- Pujasari - Adaptation, Injury, & Death of CellsDocument24 pagesPujasari - Adaptation, Injury, & Death of CellsEfa FathurohmiNo ratings yet
- Disturbances of Growth Asnan Sphinx 6 PDFDocument20 pagesDisturbances of Growth Asnan Sphinx 6 PDFmina hishamNo ratings yet
- Cellular Injury, Adaptation and Cell DeathDocument8 pagesCellular Injury, Adaptation and Cell DeathJessica Febrina Wuisan100% (1)
- A) Cell Atrophy:: Cellular AdaptationDocument7 pagesA) Cell Atrophy:: Cellular AdaptationHamid AlyadumiNo ratings yet
- L2 Patho Cell Response to Injury 1 (Basic of Disease) (1)Document28 pagesL2 Patho Cell Response to Injury 1 (Basic of Disease) (1)mohamedelkomy4400No ratings yet
- Cellular Responses To Stress and Toxic Insults PDFDocument11 pagesCellular Responses To Stress and Toxic Insults PDFDental TutorNo ratings yet
- Cell Membrane Therapy: Clinical Practice in Brain, Liver and Cardiovascular DiseasesFrom EverandCell Membrane Therapy: Clinical Practice in Brain, Liver and Cardiovascular DiseasesNo ratings yet
- Solutions: Spheres, Cones and CylindersDocument13 pagesSolutions: Spheres, Cones and CylindersKeri-ann MillarNo ratings yet
- NSX 100-630 User ManualDocument152 pagesNSX 100-630 User Manualagra04100% (1)
- Casestudy3 Hbo MaDocument2 pagesCasestudy3 Hbo Ma132345usdfghjNo ratings yet
- Fashion Cycle StepsDocument2 pagesFashion Cycle Stepssaranya narenNo ratings yet
- Hydrocarbon: Understanding HydrocarbonsDocument9 pagesHydrocarbon: Understanding HydrocarbonsBari ArouaNo ratings yet
- English Extra Conversation Club International Women's DayDocument2 pagesEnglish Extra Conversation Club International Women's Dayevagloria11No ratings yet
- True False Survey FinalDocument2 pagesTrue False Survey Finalwayan_agustianaNo ratings yet
- Kennedy 1945 Bibliography of Indonesian Peoples and CulturesDocument12 pagesKennedy 1945 Bibliography of Indonesian Peoples and CulturesJennifer Williams NourseNo ratings yet
- Rotational Equilibrium SimulationDocument3 pagesRotational Equilibrium SimulationCamille ManlongatNo ratings yet
- Hanwha Engineering & Construction - Brochure - enDocument48 pagesHanwha Engineering & Construction - Brochure - enAnthony GeorgeNo ratings yet
- WEEK 8. - Gen Math-PortfolioDocument12 pagesWEEK 8. - Gen Math-PortfolioOreo ProductionsNo ratings yet
- Polygenic InheritanceDocument13 pagesPolygenic InheritanceSandeep Kumar RaghuvanshiNo ratings yet
- Project Report On AdidasDocument33 pagesProject Report On Adidassanyam73% (37)
- PropensityModels PDFDocument4 pagesPropensityModels PDFSarbarup BanerjeeNo ratings yet
- Fehniger Steve-Pump VibrationDocument35 pagesFehniger Steve-Pump VibrationSheikh Shoaib100% (1)
- Laws of ThermocoupleDocument3 pagesLaws of ThermocoupleMourougapragash SubramanianNo ratings yet
- 02 MortarsDocument2 pages02 MortarsTarun kumar DigarseNo ratings yet
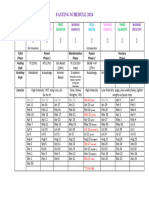
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- (PDF) Biochemistry and Molecular Biology of Plants: Book DetailsDocument1 page(PDF) Biochemistry and Molecular Biology of Plants: Book DetailsArchana PatraNo ratings yet
- Hisar CFC - Approved DPRDocument126 pagesHisar CFC - Approved DPRSATYAM KUMARNo ratings yet
- Bal - 2011 - The New HRM in The 21st Century - A Strategic ViewDocument15 pagesBal - 2011 - The New HRM in The 21st Century - A Strategic ViewJoaquínMartínezMiñoNo ratings yet
- DLL Grade7 First 1solutions ConcentrationDocument5 pagesDLL Grade7 First 1solutions ConcentrationJaneth de JuanNo ratings yet
- Complete Guide To E-Commerce TechnologyDocument420 pagesComplete Guide To E-Commerce Technologypilatus100% (4)
- 266 009-336Document327 pages266 009-336AlinaE.BarbuNo ratings yet
- Smoktech Vmax User ManualDocument9 pagesSmoktech Vmax User ManualStella PapaNo ratings yet
- Useful Relations in Quantum Field TheoryDocument30 pagesUseful Relations in Quantum Field TheoryDanielGutierrez100% (1)
- S06 - 1 THC560 DD311Document128 pagesS06 - 1 THC560 DD311Canchari Pariona Jhon AngelNo ratings yet
- Aos Warscroll Fimir WarriorsDocument1 pageAos Warscroll Fimir WarriorsGuido Sebastián AlvarezNo ratings yet
- Olympic Ayres Magic LyricsDocument1 pageOlympic Ayres Magic Lyricsjackliddy96No ratings yet
- CBT QuestionsDocument20 pagesCBT Questionsmohammed amjad ali100% (1)


















































![Pathology Slides 2023 (B&B) [Medicalstudyzone.com]](https://imgv2-2-f.scribdassets.com/img/document/722116788/149x198/9036bf21f0/1712849031?v=1)