You might also like
- Intrathecal MorphineDocument6 pagesIntrathecal MorphineJoana MoreiraNo ratings yet
- Whole Life NutritionDocument574 pagesWhole Life NutritionPRAGATI100% (1)
- Spinal cord injury assessment and classificationsDocument3 pagesSpinal cord injury assessment and classificationsjvshinesNo ratings yet
- Surgical Management of Thyroid NeoplasmsDocument15 pagesSurgical Management of Thyroid NeoplasmsalameluNo ratings yet
- AnisocoriaDocument11 pagesAnisocoriaChaturangaNSenerathNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Principles of AnesthesiaDocument60 pagesPrinciples of AnesthesiaTakale BuloNo ratings yet
- Traumatic Brain InjuryDocument40 pagesTraumatic Brain InjuryRed DevilNo ratings yet
- Lip Cancer-Ablative and Reconstructive Surgery: ChapDocument52 pagesLip Cancer-Ablative and Reconstructive Surgery: ChapYang Lin Chen100% (1)
- Oral hypoglycemic agents: Biguanides, Sulfonylureas, α-glucosidase inhibitors and moreDocument31 pagesOral hypoglycemic agents: Biguanides, Sulfonylureas, α-glucosidase inhibitors and moreBivek Singh RathoreNo ratings yet
- Anesthesia Management For Burn PatientDocument16 pagesAnesthesia Management For Burn PatientDagne AdugnaNo ratings yet
- Case Study AppendectomyDocument39 pagesCase Study AppendectomyHomework Ping100% (1)
- What Is A Session Like?Document5 pagesWhat Is A Session Like?Ioan AndraNo ratings yet
- DIFFICULT AIRWAY ALGORITHM GUIDEDocument48 pagesDIFFICULT AIRWAY ALGORITHM GUIDEshikhaNo ratings yet
- Diabetic Neuropathy PPT Final2Document61 pagesDiabetic Neuropathy PPT Final2Jenny Juniora Ajoc100% (1)
- AFMC PrimerDocument523 pagesAFMC PrimerFajar Nurrachman100% (1)
- Apixaban for Cancer-Associated VTEDocument38 pagesApixaban for Cancer-Associated VTESupawadee KhetsinbunNo ratings yet
- Chronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultsDocument14 pagesChronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultschristineNo ratings yet
- Preoperative PreparationDocument22 pagesPreoperative Preparationjackyploes100% (1)
- Advanced AirwayDocument34 pagesAdvanced Airwayvica_christiaNo ratings yet
- Immediate Nursing Interventions for Common Medical ConditionsDocument91 pagesImmediate Nursing Interventions for Common Medical ConditionsElizalde HusbandNo ratings yet
- Guidelines For The Management of Severe Traumatic Brain Injury 4th EditionDocument62 pagesGuidelines For The Management of Severe Traumatic Brain Injury 4th EditionNailahRahmahNo ratings yet
- Spinal InjuriesDocument22 pagesSpinal InjuriesPak Budi warsonoNo ratings yet
- DR - Praful Zinzuwadia M.D.,D.ADocument40 pagesDR - Praful Zinzuwadia M.D.,D.AprafulzinzuwadiaNo ratings yet
- Dexmedetomidine: (Precedex - Abbott Laboratories)Document6 pagesDexmedetomidine: (Precedex - Abbott Laboratories)battreyNo ratings yet
- Head Trauma: Khamim Thohari Rsud DR Muhammad Soewandhie SurabayaDocument33 pagesHead Trauma: Khamim Thohari Rsud DR Muhammad Soewandhie SurabayaJessica Alexandria WuNo ratings yet
- Presentation SWINE FLUDocument40 pagesPresentation SWINE FLUdr_hammadNo ratings yet
- Special Pathology Batch '21 Viva Questions CompilationDocument20 pagesSpecial Pathology Batch '21 Viva Questions Compilationuzair akhtarNo ratings yet
- General anesthesia procedure, indications, and comparison to local anesthesiaDocument9 pagesGeneral anesthesia procedure, indications, and comparison to local anesthesiaRavi PatelNo ratings yet
- Advia 2120i Hematology SystemDocument8 pagesAdvia 2120i Hematology SystemDwitaRiadiniNo ratings yet
- Bleeding Disorder (Paediatrics)Document95 pagesBleeding Disorder (Paediatrics)Nurul Afiqah Mohd YusoffNo ratings yet
- Anesthesia for Laparoscopic SurgeryDocument32 pagesAnesthesia for Laparoscopic SurgeryKelvin Tuazon100% (2)
- Anaesthesia For Infants and ChildrenDocument9 pagesAnaesthesia For Infants and Childrenapi-142637023No ratings yet
- Csbpr7 Acute Stroke Management Module Final Eng 2022Document161 pagesCsbpr7 Acute Stroke Management Module Final Eng 2022Vigneshwara NagarajanNo ratings yet
- TIVA - Copy (2) - Copy-1Document34 pagesTIVA - Copy (2) - Copy-1Keerthikumar Parvatha100% (2)
- A Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical CasesDocument5 pagesA Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical Casesnethra nitinNo ratings yet
- Anti Viral DrugsDocument70 pagesAnti Viral DrugsDereje DZ100% (2)
- Pinguecula and Pterygium GuideDocument5 pagesPinguecula and Pterygium GuideandrewNo ratings yet
- Pregnancy and Lactation FinalDocument65 pagesPregnancy and Lactation Finalakemifunabasi100% (5)
- Premedicantdrugs1 170216071329Document49 pagesPremedicantdrugs1 170216071329Sagar BhardwajNo ratings yet
- Laboratory Evaluation of PlateletsDocument28 pagesLaboratory Evaluation of PlateletsTom Anthony TonguiaNo ratings yet
- IPM for Okra PestsDocument21 pagesIPM for Okra PestsParry Grewal100% (1)
- Intravenous Anesthetic Agents: by Miss Maidah MehtabDocument49 pagesIntravenous Anesthetic Agents: by Miss Maidah MehtabLuqman QadirNo ratings yet
- Assessing and Preventing Delirium in Hospitalized PatientsDocument34 pagesAssessing and Preventing Delirium in Hospitalized PatientsVishala MishraNo ratings yet
- PropofolDocument27 pagesPropofolRoberto Carlos Castillo LopezNo ratings yet
- Optimizing Acute Pain Management: A Guide To Multimodal Analgesia and Quality ImprovementDocument10 pagesOptimizing Acute Pain Management: A Guide To Multimodal Analgesia and Quality ImprovementAgus HendraNo ratings yet
- Intrathecal Morphine Single DoseDocument25 pagesIntrathecal Morphine Single DoseVerghese GeorgeNo ratings yet
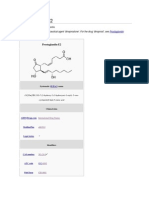
- Prostaglandin E2Document7 pagesProstaglandin E2Tanasescu MariusNo ratings yet
- Tonsillitis BK (LR)Document57 pagesTonsillitis BK (LR)Tiffany NurzamanNo ratings yet
- Vitamin A and XerophthalmiaDocument29 pagesVitamin A and XerophthalmiaJayashree IyerNo ratings yet
- Brain Abscess: Mohd Roslee Bin Abd GhaniDocument36 pagesBrain Abscess: Mohd Roslee Bin Abd GhaniSaha DirllahNo ratings yet
- Open Fracture Raju3Document72 pagesOpen Fracture Raju3Chowdhury Iqbal MahmudNo ratings yet
- General Anaesthesia OverviewDocument21 pagesGeneral Anaesthesia OverviewKamel HadyNo ratings yet
- SugamadexDocument4 pagesSugamadexashish4285No ratings yet
- Parotid EctomyDocument33 pagesParotid EctomyAgung Anom Arie WiradanaNo ratings yet
- Post Op DeliriumDocument26 pagesPost Op DeliriumKannan GNo ratings yet
- Analgesia For Labor and Vaginal DeliveryDocument21 pagesAnalgesia For Labor and Vaginal DeliveryLouije MombzNo ratings yet
- Effective communication in general practiceDocument15 pagesEffective communication in general practiceprofarmah6150No ratings yet
- TRACHOMA: CAUSES, SYMPTOMS, AND CONTROLDocument16 pagesTRACHOMA: CAUSES, SYMPTOMS, AND CONTROLabidmc110404No ratings yet
- Conscious sedation techniques and risksDocument84 pagesConscious sedation techniques and risksKhaled GharaibehNo ratings yet
- Assessment of Postoperative Fever BMJDocument40 pagesAssessment of Postoperative Fever BMJMario Guzmán GutiérrezNo ratings yet
- Update On The Management of LaryngospasmDocument6 pagesUpdate On The Management of LaryngospasmGede Eka Putra NugrahaNo ratings yet
- Pre-hospital care and assessment of smoke inhalation injuryDocument5 pagesPre-hospital care and assessment of smoke inhalation injurypaulineorrNo ratings yet
- Caudal BlockDocument6 pagesCaudal BlockAshish PandeyNo ratings yet
- Failed Spinal Anaesthesia Mechanisms, Management and PreventionDocument6 pagesFailed Spinal Anaesthesia Mechanisms, Management and Preventiondrhemantt1279No ratings yet
- Hyperglycemic Hyperosmolar StateDocument17 pagesHyperglycemic Hyperosmolar StateAqila Mumtaz50% (2)
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- BMJ-Neonatal Jaundice PDFDocument54 pagesBMJ-Neonatal Jaundice PDFkhacthuanprovipNo ratings yet
- Intravenous Regonal Anaesthesia Biers BlockDocument2 pagesIntravenous Regonal Anaesthesia Biers BlockOkenabirhieNo ratings yet
- Skeletal Muscle RelaxantsDocument11 pagesSkeletal Muscle RelaxantsAhmed Al-ArwaliNo ratings yet
- Propofol: Present by The StudentDocument7 pagesPropofol: Present by The StudentAli dhyaaNo ratings yet
- 1.1 Fundamentals of The Nervous SystemDocument18 pages1.1 Fundamentals of The Nervous Systemno nameNo ratings yet
- Evaluation and Management of Autonomic Nervous System DisordersDocument10 pagesEvaluation and Management of Autonomic Nervous System DisordersbpppbbNo ratings yet
- Abdurrehman's Resume for Biotechnology CareerDocument2 pagesAbdurrehman's Resume for Biotechnology CareerQasim KhanNo ratings yet
- n360 wk06 Mini Care Plan - Patient ADocument2 pagesn360 wk06 Mini Care Plan - Patient Aapi-272566401No ratings yet
- COVID-19 Reflection - Pengosro, YzahDocument5 pagesCOVID-19 Reflection - Pengosro, Yzahyzah graceNo ratings yet
- نماذج انجليزي مع الحلول - الطب - جامعة حضرموتDocument45 pagesنماذج انجليزي مع الحلول - الطب - جامعة حضرموتSuliemanNo ratings yet
- Robert Murphy DissertationDocument6 pagesRobert Murphy DissertationPaperWritingCompanyCanada100% (1)
- Vestibular NeuritisDocument2 pagesVestibular NeuritisElsa Nabila YumezaNo ratings yet
- Catharanthus RoseusDocument7 pagesCatharanthus RoseusMilind SagarNo ratings yet
- Citología Cervical Screening ACOGDocument11 pagesCitología Cervical Screening ACOGEduardo SasintuñaNo ratings yet
- Ijms 19 00311Document26 pagesIjms 19 00311Hidayat ArifinNo ratings yet
- The Beer Geek Handbook - Living A Life Ruled by Beer (2016)Document58 pagesThe Beer Geek Handbook - Living A Life Ruled by Beer (2016)zaratustra21No ratings yet
- Patient With Neutropenia Risk For Infection Related To Inadequate Secondary Defenses (Leukopenia, Neutropenia), Altered Response To MicrobialDocument2 pagesPatient With Neutropenia Risk For Infection Related To Inadequate Secondary Defenses (Leukopenia, Neutropenia), Altered Response To MicrobialICa MarlinaNo ratings yet
- Effectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisDocument9 pagesEffectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisrebeca paulinoNo ratings yet
- Nutrients and Their Functions in Maintaining HealthDocument6 pagesNutrients and Their Functions in Maintaining Healthuma crespoNo ratings yet
- PSORIASISDocument9 pagesPSORIASISDianne BernardoNo ratings yet
- MSDS Disel FuelDocument12 pagesMSDS Disel FuelMatthew Pham-EvansNo ratings yet
- 17.national Malaria Case Management Guideline 14 January 2022 UnderDocument61 pages17.national Malaria Case Management Guideline 14 January 2022 UnderTizazu BayihNo ratings yet