You might also like
- Laporan Kasus Peripartum Cardiomyopathy RsmiDocument29 pagesLaporan Kasus Peripartum Cardiomyopathy RsmikurniaNo ratings yet
- Secondary HLH Case Report: Highlighting Clinical ChallengesDocument11 pagesSecondary HLH Case Report: Highlighting Clinical ChallengesDr. Surya Abadi KristyoadiNo ratings yet
- Borang IshipDocument9 pagesBorang IshipUlfa RahayuNo ratings yet
- Catatan Jaga 29 April 2019Document10 pagesCatatan Jaga 29 April 2019Frizky HapsariNo ratings yet
- Kematian Obstetri DAWDocument10 pagesKematian Obstetri DAWBrian AfiffNo ratings yet
- MR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDocument23 pagesMR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDr. Surya Abadi KristyoadiNo ratings yet
- MAPPING PINERE 6, Jumat 3 Sep 2021Document5 pagesMAPPING PINERE 6, Jumat 3 Sep 2021Rina SyafritaNo ratings yet
- JEJARING DR - Rahma, DR - Dewi, DR - Herry 10-10-2021Document1 pageJEJARING DR - Rahma, DR - Dewi, DR - Herry 10-10-2021nina purnamasariNo ratings yet
- Update Mapping Zmzam Jejaring Sabtu 20 November 2021Document13 pagesUpdate Mapping Zmzam Jejaring Sabtu 20 November 2021Rina SyafritaNo ratings yet
- Pinere 1 30 Juli 2021Document1 pagePinere 1 30 Juli 2021Rina SyafritaNo ratings yet
- Mapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Document2 pagesMapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Rina SyafritaNo ratings yet
- MappingDocument4 pagesMappingRina SyafritaNo ratings yet
- Wa0001.Document39 pagesWa0001.faithdamilola460No ratings yet
- Case Study of CancerDocument8 pagesCase Study of CancerAmina TariqNo ratings yet
- Mapping Aqsa 3, Jumat Sore, 5 Mei 2023 NewDocument10 pagesMapping Aqsa 3, Jumat Sore, 5 Mei 2023 NewmushaddiqNo ratings yet
- Asalamualaikum Kakak AyukDocument4 pagesAsalamualaikum Kakak AyukIlmiah Program studi ObginNo ratings yet
- MAPPINGDocument2 pagesMAPPINGPratiwi ARHNo ratings yet
- Mapping Aqsa 1 Rs Baru, 11 Oktober 2021Document4 pagesMapping Aqsa 1 Rs Baru, 11 Oktober 2021Umar RasyidinNo ratings yet
- General Census Nov 13Document8 pagesGeneral Census Nov 13Mark Angelo PonferradoNo ratings yet
- Macabali GS2Document4 pagesMacabali GS2Christian Edward MacabaliNo ratings yet
- Presentation On UrosepsisDocument20 pagesPresentation On UrosepsisNewtan DebNo ratings yet
- UnnamedDocument8 pagesUnnamedAllison Eunice ServandoNo ratings yet
- DM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S VenkataseshanDocument50 pagesDM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S Venkataseshanvishal sidanaNo ratings yet
- Virtual Rle Simulation Phase 1 Morning ShiftDocument11 pagesVirtual Rle Simulation Phase 1 Morning ShiftRyrey Abraham PacamanaNo ratings yet
- 24 Feb 24 Distribusi Pasien Visite Besar Ilmu Bedah FK ULMDocument11 pages24 Feb 24 Distribusi Pasien Visite Besar Ilmu Bedah FK ULMWildan'z CreedNo ratings yet
- Morning Report Sunday Morning, March 8th 2020: Syt/Slr/Sth/SwiDocument25 pagesMorning Report Sunday Morning, March 8th 2020: Syt/Slr/Sth/SwimuhammadrikiNo ratings yet
- Mapping Aqsa 3 (20 Februari 2019)Document6 pagesMapping Aqsa 3 (20 Februari 2019)Egi Atika HandayaniNo ratings yet
- Mapping PDP 11 SeptDocument7 pagesMapping PDP 11 Septranti putri ayuNo ratings yet
- WEEKLY REPORT 1nov-7 NovDocument12 pagesWEEKLY REPORT 1nov-7 NovsilanandacahyaNo ratings yet
- Lapsus Krisis TiroidDocument37 pagesLapsus Krisis TiroidariceghaNo ratings yet
- Morning Report: 2 March 2021 Night ShiftDocument16 pagesMorning Report: 2 March 2021 Night ShiftWilujeng AnggrainiNo ratings yet
- Type Ii Diabetes: Presented by Thomas Eipe Pharmd InternDocument31 pagesType Ii Diabetes: Presented by Thomas Eipe Pharmd InternThomas EipeNo ratings yet
- Pedia NotesDocument4 pagesPedia NotesDana CastroNo ratings yet
- Pomr Dewi 190919Document6 pagesPomr Dewi 190919emjehNo ratings yet
- ObstetriDocument50 pagesObstetriBobziRazvidiNo ratings yet
- 2nd Case Scenario BronchitisDocument5 pages2nd Case Scenario BronchitisKasandra Dawn Moquia BerisoNo ratings yet
- Surgery PortDocument5 pagesSurgery Portabenezer g/kirstosNo ratings yet
- Mappimg Kamar 1 Dan 5Document4 pagesMappimg Kamar 1 Dan 5Satrya DitaNo ratings yet
- Rina Mapping TerbaruDocument2 pagesRina Mapping TerbaruRina SyafritaNo ratings yet
- Shafa 17 MeiDocument1 pageShafa 17 Meinina purnamasariNo ratings yet
- General Census Nov 27Document8 pagesGeneral Census Nov 27Mark Angelo PonferradoNo ratings yet
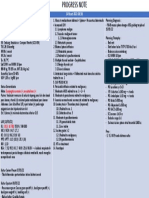
- Progress Note 14 Maret Ny.S - 26Document1 pageProgress Note 14 Maret Ny.S - 26Ika AyuNo ratings yet
- Cue and Clue PL Idx PDX PTX Pmo&Ed: Mrs. C /79 Yo/Incovit Ward Subjective Non PharmacologyDocument12 pagesCue and Clue PL Idx PDX PTX Pmo&Ed: Mrs. C /79 Yo/Incovit Ward Subjective Non PharmacologyIka AyuNo ratings yet
- Mapping Aqsa 2 Senin Pagi, 12 Juni 2023-2Document12 pagesMapping Aqsa 2 Senin Pagi, 12 Juni 2023-2Caesar RiayatsyahNo ratings yet
- Aqsha 3 (Penyakit Dalam Wanita)Document6 pagesAqsha 3 (Penyakit Dalam Wanita)difa fatayaNo ratings yet
- Mapping Aqsa 2 Senin SORE UPDATE TERBARU, 12 Juni 2023Document12 pagesMapping Aqsa 2 Senin SORE UPDATE TERBARU, 12 Juni 2023Caesar RiayatsyahNo ratings yet
- Patient Profile Form Department of Pharmacy Practice Nargund College of Pharmacy, BangaloreDocument2 pagesPatient Profile Form Department of Pharmacy Practice Nargund College of Pharmacy, BangaloreRaju NiraulaNo ratings yet
- Morning Report: Rsau Dr. M. Munir Lanud Abd. SalehDocument10 pagesMorning Report: Rsau Dr. M. Munir Lanud Abd. SalehQonita Prasta AgustiaNo ratings yet
- General Census Nov 7Document5 pagesGeneral Census Nov 7Mark Angelo PonferradoNo ratings yet
- DepartmentDocument7 pagesDepartmentmubarek abdurohemanNo ratings yet
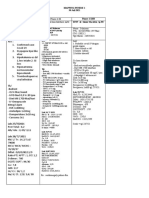
- Dokter Ruangan:dr. Gabriel P Bed 2.1.1: Identitas Keluhan Pemeriksaan Lab/ Penunjang Diagnosa Terapi PerencanaanDocument26 pagesDokter Ruangan:dr. Gabriel P Bed 2.1.1: Identitas Keluhan Pemeriksaan Lab/ Penunjang Diagnosa Terapi Perencanaanx22xNo ratings yet
- Recurrent TonsilitisDocument16 pagesRecurrent TonsilitisAyen FornollesNo ratings yet
- Residents Notes LumbaoDocument3 pagesResidents Notes LumbaoRizielle MendozaNo ratings yet
- Mapping Jejaring Sabtu, 6 Mei 2023Document18 pagesMapping Jejaring Sabtu, 6 Mei 2023mushaddiqNo ratings yet
- Duty Ricky CKD R.28 NewDocument4 pagesDuty Ricky CKD R.28 NewRicky Cornelius TariganNo ratings yet
- Clinical Conference 21 August 2022: Eria (New Case)Document16 pagesClinical Conference 21 August 2022: Eria (New Case)mujahidah nursinNo ratings yet
- Leukosit: Positif Protein: Positif (+2) Urobilinogen: Positif Darah:positif Sedimen Urine: Leukosit: 25-50 Eritrosit: 100-130 Epitel: 1-3 Lain-LainDocument3 pagesLeukosit: Positif Protein: Positif (+2) Urobilinogen: Positif Darah:positif Sedimen Urine: Leukosit: 25-50 Eritrosit: 100-130 Epitel: 1-3 Lain-Lainifanda80No ratings yet
- Shafa 10.10.2021Document5 pagesShafa 10.10.2021nina purnamasariNo ratings yet
- Maping Pinere 1, Jum'at 24 September 2021: TH THDocument2 pagesMaping Pinere 1, Jum'at 24 September 2021: TH THRina SyafritaNo ratings yet
- Case Report: Peripartum Cardiomyopath YDocument2 pagesCase Report: Peripartum Cardiomyopath Ykiritokazuto35No ratings yet
- Pregnancy and Heart DiseaseDocument60 pagesPregnancy and Heart DiseaseAndi Suchy Qumala SarieNo ratings yet
- SelfEsteem PDFDocument2 pagesSelfEsteem PDFkiritokazuto35No ratings yet
- Faktor Risiko Occupational DermatosisDocument8 pagesFaktor Risiko Occupational Dermatosiskiritokazuto35No ratings yet
- M Kaavya Sree Balaji Medical College and Hospital IndiaDocument33 pagesM Kaavya Sree Balaji Medical College and Hospital Indiakiritokazuto35No ratings yet
- Jadwal Jaga Dokter Internsip Bulan September Periode I 2021Document1 pageJadwal Jaga Dokter Internsip Bulan September Periode I 2021kiritokazuto35No ratings yet
- BC 7 DDocument6 pagesBC 7 Dkiritokazuto35No ratings yet
- Adolescent Psychology: What To Be On The Look Out ForDocument9 pagesAdolescent Psychology: What To Be On The Look Out ForPromita MaitraNo ratings yet
- Teori Pomr 27 Nov 2019 Inpartu Fase AktifDocument4 pagesTeori Pomr 27 Nov 2019 Inpartu Fase Aktifkiritokazuto35No ratings yet
- Wms Main Pocket Guide 2017Document29 pagesWms Main Pocket Guide 2017justrudinNo ratings yet
- Pem Be Rita HuanDocument244 pagesPem Be Rita Huanwilliam williamNo ratings yet
- Step 1: Are The Results of The Study Valid?: Full Spectrum of Patients - Those With MildDocument4 pagesStep 1: Are The Results of The Study Valid?: Full Spectrum of Patients - Those With Mildkiritokazuto35No ratings yet
- Asthma Children Full GuidelineDocument17 pagesAsthma Children Full Guidelinemuhammad iqbalNo ratings yet
- ACR HandoutDocument1 pageACR Handoutkiritokazuto35No ratings yet
- Atrial Septal Defects: Imaging Conference December 10, 2008 Angela Morello, M.DDocument49 pagesAtrial Septal Defects: Imaging Conference December 10, 2008 Angela Morello, M.Dkiritokazuto35No ratings yet
- Diagnosis and Treatment of Lumbar Disc Herniation With RadiculopathyDocument100 pagesDiagnosis and Treatment of Lumbar Disc Herniation With RadiculopathyHelenNo ratings yet
- Jurnal Urter TraumaDocument14 pagesJurnal Urter Traumakiritokazuto35No ratings yet
- IPD 6 - Dr. Andi, SPJPDocument34 pagesIPD 6 - Dr. Andi, SPJPkiritokazuto35No ratings yet
- Presentation 3Document4 pagesPresentation 3kiritokazuto35No ratings yet
- Jurnal Urter TraumaDocument14 pagesJurnal Urter Traumakiritokazuto35No ratings yet
- Local Anaesthetics Mcqs From LouisDocument6 pagesLocal Anaesthetics Mcqs From LouisAmreen Khan100% (1)
- Why Is Research Important - NHS GroupDocument8 pagesWhy Is Research Important - NHS GroupRoxan PacsayNo ratings yet
- Eye Eye Assessment Assessment and Care and CareDocument126 pagesEye Eye Assessment Assessment and Care and CareBern NerquitNo ratings yet
- A03 - Mr. Pradeep Kumar Tripathi - FPSC George Town 18/1A, A.N. Jha Marg Georgetown, Allahabad, UpDocument6 pagesA03 - Mr. Pradeep Kumar Tripathi - FPSC George Town 18/1A, A.N. Jha Marg Georgetown, Allahabad, UpSanjay GuptaNo ratings yet
- KSCST PresentationDocument44 pagesKSCST PresentationAkshay SavvasheriNo ratings yet
- Ergonomic Factors in Construction Industry: A Literature ReviewDocument14 pagesErgonomic Factors in Construction Industry: A Literature ReviewdhanarajNo ratings yet
- 61Document11 pages61Mohammed Issa SalehNo ratings yet
- Nursing Process: Franco L. Razon, Man, RN Divine Word College of Legazpi College of NursingDocument72 pagesNursing Process: Franco L. Razon, Man, RN Divine Word College of Legazpi College of NursingFranco RazonNo ratings yet
- I-Stat 1 Quick Reference Guide 716942-00l CompressedDocument7 pagesI-Stat 1 Quick Reference Guide 716942-00l Compressedنجلاء الطلحيNo ratings yet
- Are You Planning To Buy or Rent A Home Built Before 1978?Document60 pagesAre You Planning To Buy or Rent A Home Built Before 1978?Maria FloresNo ratings yet
- KP Astrology Rules of PredictionDocument4 pagesKP Astrology Rules of PredictionRajeshNo ratings yet
- Subject: PsychopharmacologyDocument11 pagesSubject: PsychopharmacologyAli IjazNo ratings yet
- Lab # 5 Use Case and Activity Diagram: ObjectivesDocument7 pagesLab # 5 Use Case and Activity Diagram: ObjectivesmexiweNo ratings yet
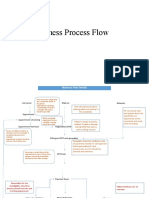
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Impaired Posture and MovementDocument40 pagesImpaired Posture and MovementMohamed Magdy ElMeligieNo ratings yet
- Rickets - A Brief View With Homoeopathic ApproachDocument32 pagesRickets - A Brief View With Homoeopathic ApproachDr. Sandeep Anwane100% (1)
- Common Skin Diseases in Africa: An Illustrated GuideDocument85 pagesCommon Skin Diseases in Africa: An Illustrated GuideJohn EnioladeNo ratings yet
- Abnormal PsychologyDocument33 pagesAbnormal PsychologyChristie SabgaNo ratings yet
- Lost Prehistorica Lost Prehistorica. Lost Creatures CombinedDocument157 pagesLost Prehistorica Lost Prehistorica. Lost Creatures CombinedVassilis Tsipopoulos100% (8)
- Intrebari Interviu Asistent MedicalDocument3 pagesIntrebari Interviu Asistent MedicalanaNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Lung Cancer Report Sample High enDocument1 pageLung Cancer Report Sample High enSiddhesh PawarNo ratings yet
- NCM 107 REVIEWER - Docx 1Document41 pagesNCM 107 REVIEWER - Docx 1kyanicoaguillanaNo ratings yet
- The Emergence of India's Pharmaceutical IndustryDocument41 pagesThe Emergence of India's Pharmaceutical Industryvivekgupta2jNo ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- PuppetryDocument183 pagesPuppetryÉva Hegedüsné50% (2)
- Contingency PlanDocument1 pageContingency PlanPramod Bodne100% (3)
- Dheeraj DumirDocument11 pagesDheeraj DumirAnonymous CR8v7xb0No ratings yet
- Moth Balls: Safety Data SheetDocument9 pagesMoth Balls: Safety Data SheethafilrediandikaNo ratings yet