You might also like
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- Presentation. 111tom AbDocument20 pagesPresentation. 111tom AbTemesgenNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Anticoagulant PresentationDocument29 pagesAnticoagulant Presentationrozha100% (2)
- Anticoagulants May BeDocument5 pagesAnticoagulants May BeAmmar magdyNo ratings yet
- AnticoagulantsDocument8 pagesAnticoagulantsRobert L G MabongaNo ratings yet
- The Pharmacology of AntithromboticsDocument14 pagesThe Pharmacology of AntithromboticsanaNo ratings yet
- Blood Pharmacology by Dr. Mayur Sayta M 910444Document21 pagesBlood Pharmacology by Dr. Mayur Sayta M 910444funzz100% (1)
- Pharmacology of Anticoagulants: Chandravathi Loke, MD, Syed S. Ali, MD, and Vandita Johari, MDDocument7 pagesPharmacology of Anticoagulants: Chandravathi Loke, MD, Syed S. Ali, MD, and Vandita Johari, MDluqmanhasansNo ratings yet
- AnticoagulantsDocument3 pagesAnticoagulantsKarthik SubramaniamNo ratings yet
- CAD Treatment with Anticoagulants, Thrombolytics & AntiplateletsDocument4 pagesCAD Treatment with Anticoagulants, Thrombolytics & AntiplateletsAbdullahIchsanNo ratings yet
- Anticoagulant TherapyDocument41 pagesAnticoagulant Therapyryan yovanNo ratings yet
- Coagulation Cascade: Anticoagulant DrugsDocument14 pagesCoagulation Cascade: Anticoagulant Drugsabdo elbahrawyNo ratings yet
- Multiple Injuries: Drug StudiesDocument10 pagesMultiple Injuries: Drug StudiesTarquin TomadaNo ratings yet
- ReviewerDocument20 pagesReviewerKC PalattaoNo ratings yet
- Agent Used in Disorder in CoagulationDocument34 pagesAgent Used in Disorder in CoagulationClinton Franda Markus SitanggangNo ratings yet
- Pharmacology II: Treatments for Blood Disorders and InflammationDocument61 pagesPharmacology II: Treatments for Blood Disorders and InflammationDiane BanuaNo ratings yet
- Antiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213Document30 pagesAntiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213JedoNo ratings yet
- UFH LMWH Fonda - 06september2020Document7 pagesUFH LMWH Fonda - 06september2020gabrimarteNo ratings yet
- Anticoagulant DrugsDocument7 pagesAnticoagulant DrugsNadia MohammadNo ratings yet
- Anti Coagulatants: Presented By:-Mr - Gorishankar Nursing Tutor (Tantia University)Document10 pagesAnti Coagulatants: Presented By:-Mr - Gorishankar Nursing Tutor (Tantia University)yogesh kumarNo ratings yet
- Haematology DrugsDocument17 pagesHaematology DrugsParyNo ratings yet
- PHM - Hematologic DrugsDocument3 pagesPHM - Hematologic DrugsJeanne Rodiño100% (3)
- Warfarin Therapy - Evolving Strategies in AnticoagulationDocument10 pagesWarfarin Therapy - Evolving Strategies in AnticoagulationarbetaNo ratings yet
- Warfarin Mechanism of ActionDocument7 pagesWarfarin Mechanism of ActionIna GrigorasNo ratings yet
- CoA Dis - RevDocument60 pagesCoA Dis - RevAzra Al AmanahNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJoyce Anne SupnetNo ratings yet
- Anti CoagulantsDocument37 pagesAnti CoagulantsMaria khurshidNo ratings yet
- Bivalirudine Drug Presentation From Nicvd DhakaDocument28 pagesBivalirudine Drug Presentation From Nicvd DhakaNavojit ChowdhuryNo ratings yet
- Anti CoagulantsDocument25 pagesAnti Coagulantsshoaib106muhammadNo ratings yet
- A Drug Study On: HeparinDocument8 pagesA Drug Study On: HeparinRaijenne VersolaNo ratings yet
- Farmakoterapi AntikoagulasiDocument20 pagesFarmakoterapi AntikoagulasiRirin AptNo ratings yet
- Pharmacology - Hematologic DrugsDocument51 pagesPharmacology - Hematologic DrugsBenjamin Joel Breboneria100% (1)
- List of AnticoagulantsDocument9 pagesList of Anticoagulantschristianz39100% (1)
- Warfarin Guide for Blood Clot PreventionDocument6 pagesWarfarin Guide for Blood Clot PreventionVidya ShankarNo ratings yet
- Verapamil PDFDocument13 pagesVerapamil PDFddandan_2No ratings yet
- Mid Human Pharma 23-24Document6 pagesMid Human Pharma 23-24Linh NguyễnNo ratings yet
- DIS HeparinDocument4 pagesDIS HeparinRebecca ChenNo ratings yet
- Heparin - ClinicalKeyDocument85 pagesHeparin - ClinicalKeydayannaNo ratings yet
- Anticoagulation 2013 Surgery OxfordDocument5 pagesAnticoagulation 2013 Surgery OxfordSanjaya SenevirathneNo ratings yet
- Comparison of Warfarin and Heparin For Thromboprophylaxes Based Upon There Safety, Efficacy and TolerabilityDocument55 pagesComparison of Warfarin and Heparin For Thromboprophylaxes Based Upon There Safety, Efficacy and Tolerabilitysaleemandsons4210No ratings yet
- AntiarrhythmiaDocument29 pagesAntiarrhythmiaDRx Raju ChandranNo ratings yet
- John Hommer E. Dy, MD.: Diplomate in Internal MedicineDocument56 pagesJohn Hommer E. Dy, MD.: Diplomate in Internal MedicinehommercuteNo ratings yet
- Angioplasty Platelet BlockersDocument4 pagesAngioplasty Platelet BlockersjoanneNo ratings yet
- Principles of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocument36 pagesPrinciples of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby Liew100% (1)
- AnticoagulantDocument34 pagesAnticoagulantAslam Baltee100% (1)
- Pos NoacDocument40 pagesPos NoacSanjeev Harry Budhooram100% (1)
- Principles of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocument36 pagesPrinciples of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby LiewNo ratings yet
- Warfarin and Newer Agents What The or - 2016 - Oral and Maxillofacial Surgery CDocument7 pagesWarfarin and Newer Agents What The or - 2016 - Oral and Maxillofacial Surgery CjoseluisNo ratings yet
- Anticoagulants: Dr. Hassan Mohamed EnowDocument37 pagesAnticoagulants: Dr. Hassan Mohamed EnowFatimaNo ratings yet
- Pharmacology and Toxicology - Anticoagulants - Medical LibraryDocument8 pagesPharmacology and Toxicology - Anticoagulants - Medical Libraryjean PiedraNo ratings yet
- Anticoagulant, Fibrinolytic, and Antiplatelet DrugsDocument22 pagesAnticoagulant, Fibrinolytic, and Antiplatelet DrugsVera Waty100% (1)
- Drugs Used in Disorders of CoagulationDocument61 pagesDrugs Used in Disorders of CoagulationDUEÑAS, MARIELNo ratings yet
- Warfarin: Prof DR Shah MuradDocument63 pagesWarfarin: Prof DR Shah Muradshahmurad653376No ratings yet
- Warfarin Therapy Management: ScopeDocument9 pagesWarfarin Therapy Management: ScopesastiraNo ratings yet
- Aspectos Prácticos Nuevos Anticoagulantes Am Jour Hem 2011Document5 pagesAspectos Prácticos Nuevos Anticoagulantes Am Jour Hem 2011jose_esteban_pena_duranNo ratings yet
- Anticoagulants and Antiplatelet Drugs: Mechanisms and Clinical UsesDocument25 pagesAnticoagulants and Antiplatelet Drugs: Mechanisms and Clinical UsesIdrissa John Sebeh ContehNo ratings yet
- DabigatranDocument6 pagesDabigatranNayelis SalasNo ratings yet
- 34 Drugs Used in Coagulation and Bleeding DisordersDocument94 pages34 Drugs Used in Coagulation and Bleeding DisordersJeanneNo ratings yet
- EnoxaparinDocument2 pagesEnoxaparinBianca Andrea RagazaNo ratings yet
- Kuliah Blok NBS 2020Document115 pagesKuliah Blok NBS 2020Ida Bagus Putu SwabawaNo ratings yet
- Antiparkinson Pharma 2020Document26 pagesAntiparkinson Pharma 2020Ida Bagus Putu SwabawaNo ratings yet
- Antipsychotics HandoutDocument25 pagesAntipsychotics HandoutTeddy Kurniady ThaherNo ratings yet
- Soebandiri Division of Hematology & Medic Oncology Departement of Medicine Airlangga University of MedicineDocument23 pagesSoebandiri Division of Hematology & Medic Oncology Departement of Medicine Airlangga University of MedicineLaura ChandraNo ratings yet
- Pharmacology of CNS: Prajogo Wibowo Faculty of Medicine Hang Tuah UniversityDocument37 pagesPharmacology of CNS: Prajogo Wibowo Faculty of Medicine Hang Tuah UniversityIda Bagus Putu SwabawaNo ratings yet
- Heatstroke Sun Stroke Acute Management and PreventionDocument44 pagesHeatstroke Sun Stroke Acute Management and PreventionDedy SavradinataNo ratings yet
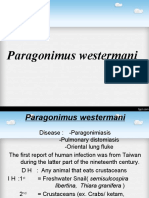
- Kuliah Paragonimus WestermaniDocument17 pagesKuliah Paragonimus WestermaniIda Bagus Putu SwabawaNo ratings yet
- Kuliah Paragonimus WestermaniDocument17 pagesKuliah Paragonimus WestermaniIda Bagus Putu SwabawaNo ratings yet
- Antianxiety, Mood Disorder and Antipsychotic MedicationsDocument74 pagesAntianxiety, Mood Disorder and Antipsychotic MedicationsIda Bagus Putu SwabawaNo ratings yet
- Male InfertilityDocument17 pagesMale InfertilityIda Bagus Putu SwabawaNo ratings yet
- Anti Diuretic Hormone Dr. EricDocument28 pagesAnti Diuretic Hormone Dr. EricIda Bagus Putu SwabawaNo ratings yet
- SeasicknessDocument14 pagesSeasicknessIda Bagus Putu SwabawaNo ratings yet
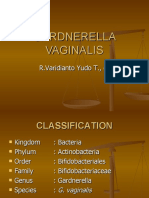
- (Kating) Gardnerella (Saphir Fkuht's Conflicted Copy 2018-01-19)Document15 pages(Kating) Gardnerella (Saphir Fkuht's Conflicted Copy 2018-01-19)Ida Bagus Putu SwabawaNo ratings yet
- Löffler SyndromeDocument9 pagesLöffler SyndromeIda Bagus Putu SwabawaNo ratings yet
- Human Rights Violations During 2020 Elections Fueled Rise in AbstentionsDocument16 pagesHuman Rights Violations During 2020 Elections Fueled Rise in AbstentionsIda Bagus Putu SwabawaNo ratings yet
- Premature Ejaculation PETERDocument10 pagesPremature Ejaculation PETERIda Bagus Putu SwabawaNo ratings yet
- Löffler SyndromeDocument9 pagesLöffler SyndromeIda Bagus Putu SwabawaNo ratings yet
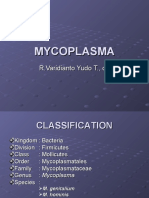
- (Kating) MycoplasmaDocument19 pages(Kating) MycoplasmaIda Bagus Putu SwabawaNo ratings yet
- Neisseria Gonorrhoeae: Classification, Epidemiology and Treatment of GonorrheaDocument27 pagesNeisseria Gonorrhoeae: Classification, Epidemiology and Treatment of GonorrheaAkhmad Ikhwan BaidlowiNo ratings yet
- (KATING) Haemophilus DucreyiDocument16 pages(KATING) Haemophilus DucreyiIda Bagus Putu SwabawaNo ratings yet
- Type 1 Diabetes in Very Young ChildrenDocument14 pagesType 1 Diabetes in Very Young ChildrenIda Bagus Putu SwabawaNo ratings yet
- Uu Ikd 8 Gel 1 Lab KompDocument6 pagesUu Ikd 8 Gel 1 Lab KompIda Bagus Putu SwabawaNo ratings yet
- Fear of Hypoglycemia in Children and Adolescents and Their Parents With DM Type 1Document14 pagesFear of Hypoglycemia in Children and Adolescents and Their Parents With DM Type 1Ida Bagus Putu SwabawaNo ratings yet
- The Anatomical Pearls On Digestive SystemDocument8 pagesThe Anatomical Pearls On Digestive SystemIda Bagus Putu SwabawaNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseIda Bagus Putu Swabawa100% (1)
- (Kating) ChlamydiaDocument22 pages(Kating) ChlamydiaIda Bagus Putu SwabawaNo ratings yet
- ReferensiDocument1 pageReferensiIda Bagus Putu SwabawaNo ratings yet
- Eradication & ControlDocument24 pagesEradication & ControlIda Bagus Putu SwabawaNo ratings yet
- The Abdominal Wall 2014 With DelDocument23 pagesThe Abdominal Wall 2014 With DelIda Bagus Putu SwabawaNo ratings yet
- Mayo ClinicDocument338 pagesMayo Clinicrajkumarss87No ratings yet
- Aspirin Therapy Risks and PreventionDocument19 pagesAspirin Therapy Risks and PreventionSaiful MukminNo ratings yet
- Clopidogrel - ClinicalKeyDocument79 pagesClopidogrel - ClinicalKeydayannaNo ratings yet
- DM + Gangren PedisDocument61 pagesDM + Gangren Pedismegadama0No ratings yet
- Ischemic Stroke Management by The Nurse PR - 2019 - The Journal For Nurse PractDocument9 pagesIschemic Stroke Management by The Nurse PR - 2019 - The Journal For Nurse PractLina SafitriNo ratings yet
- Management of Bleeding Disorders in The Dental PraDocument5 pagesManagement of Bleeding Disorders in The Dental Praamoon almNo ratings yet
- Treatments in Ischemic StrokeDocument18 pagesTreatments in Ischemic StrokeFercho MedNo ratings yet
- Medication Instructions Prior To SurgeryDocument11 pagesMedication Instructions Prior To Surgeryhohj100% (1)
- D-dimer and platelet aggregation predict thrombotic risk in PADDocument8 pagesD-dimer and platelet aggregation predict thrombotic risk in PADlidawatiNo ratings yet
- Kawasaki DiseaseDocument33 pagesKawasaki Diseasejoshianandk100% (2)
- Benefit and Risks of Clopidogrel Vs Aspirin Monotherapy After Recent Ischemic StrokDocument13 pagesBenefit and Risks of Clopidogrel Vs Aspirin Monotherapy After Recent Ischemic StrokRichardNo ratings yet
- Clopidogrel Drug StudyDocument1 pageClopidogrel Drug StudyNicole Soo89% (9)
- Peripheral Artery DiseaseDocument45 pagesPeripheral Artery DiseaseIchwan ZuantoNo ratings yet
- International Journal of Cardiology June 2021 Issue 1Document241 pagesInternational Journal of Cardiology June 2021 Issue 1Fareesha KhanNo ratings yet
- Perioperative Management of Oral Antithrombotics in Dentistry and Oral Surgery: Part 2Document12 pagesPerioperative Management of Oral Antithrombotics in Dentistry and Oral Surgery: Part 2mariajnavarro2505No ratings yet
- 18 Consultative HematologyDocument40 pages18 Consultative HematologyJose Luis Gutierrez RamirezNo ratings yet
- Jambi Cardiology Update WorkshopDocument3 pagesJambi Cardiology Update WorkshopFahrurrozi SyarifNo ratings yet
- Dual Antiplatelet Therapy Using Cilostazol For SecondaryDocument10 pagesDual Antiplatelet Therapy Using Cilostazol For SecondarySyed Shabbir HaiderNo ratings yet
- Antiplatelet Therapy For The Secondary Prevention of Ischemic Stroke - UpToDateDocument13 pagesAntiplatelet Therapy For The Secondary Prevention of Ischemic Stroke - UpToDateSuci WijayaNo ratings yet
- Book ReviewsDocument7 pagesBook Reviewsrahman10191871No ratings yet
- Common Drugs With Effective Off-Label UsesDocument10 pagesCommon Drugs With Effective Off-Label Usesredwan_rnNo ratings yet
- New Drugs and Technologies: PrasugrelDocument10 pagesNew Drugs and Technologies: PrasugrelDewi FitrianaNo ratings yet
- Reduce CVD Risk with AntihypertensivesDocument4 pagesReduce CVD Risk with AntihypertensivesMohamedNo ratings yet
- SICH MGMTDocument12 pagesSICH MGMTLennon Ponta-oyNo ratings yet
- Clinical Guide To The Use of Antithrombotic Drugs in Coronary Artery Disease - D. Angiolli, Et. Al., (Informa, 2008) WW PDFDocument306 pagesClinical Guide To The Use of Antithrombotic Drugs in Coronary Artery Disease - D. Angiolli, Et. Al., (Informa, 2008) WW PDFSergiu PlescaNo ratings yet
- Antiplatelet Therapy For Acute StrokeDocument10 pagesAntiplatelet Therapy For Acute StrokeInstalasi OK RSI JombangNo ratings yet
- Summary of Product CharacteristicsDocument24 pagesSummary of Product Characteristicsddandan_2No ratings yet
- AHA 2018 Guidelines for CKD TherapyDocument78 pagesAHA 2018 Guidelines for CKD Therapyaditya ratna utariNo ratings yet
- Clopidogrel: 26% More Effective than AspirinDocument30 pagesClopidogrel: 26% More Effective than AspirinMuhammad Yolandi SumadioNo ratings yet
- BMJ k5108 FullDocument10 pagesBMJ k5108 Fulldana irnandaNo ratings yet
![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-1-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)