You might also like
- Qualitative Tests For Carbohydrates: 1) Molisch TestDocument20 pagesQualitative Tests For Carbohydrates: 1) Molisch TestFRANCEEN LEANNA KATIGBAKNo ratings yet
- Mathematics-in-the-Modern-World-Module by CHEDDocument444 pagesMathematics-in-the-Modern-World-Module by CHEDFRANCEEN LEANNA KATIGBAK83% (6)
- LP maximize calculator profitsDocument12 pagesLP maximize calculator profitsFRANCEEN LEANNA KATIGBAKNo ratings yet
- Fault-Tolerance: Information Redundancy - Error Control Examples: Check Digit Computation of Bank Routing NumberDocument3 pagesFault-Tolerance: Information Redundancy - Error Control Examples: Check Digit Computation of Bank Routing NumberFRANCEEN LEANNA KATIGBAKNo ratings yet
- Glycogen Isolation and Determination ofDocument14 pagesGlycogen Isolation and Determination ofChristian De LeonNo ratings yet
- Isolation From Chicken Liver and Enzymatic Hydrolysis of GlycogenDocument2 pagesIsolation From Chicken Liver and Enzymatic Hydrolysis of GlycogenAngela ResicoNo ratings yet
- Qualitative Tests For Carbohydrates: 1) Molisch TestDocument20 pagesQualitative Tests For Carbohydrates: 1) Molisch TestFRANCEEN LEANNA KATIGBAKNo ratings yet
- Respiratory System: DR Archna Ghildiyal Associate ProfessorDocument35 pagesRespiratory System: DR Archna Ghildiyal Associate ProfessorFRANCEEN LEANNA KATIGBAKNo ratings yet
- Respiratory System: DR Archna Ghildiyal Associate ProfessorDocument35 pagesRespiratory System: DR Archna Ghildiyal Associate ProfessorFRANCEEN LEANNA KATIGBAKNo ratings yet
- The Respiratory SystemDocument58 pagesThe Respiratory SystemFRANCEEN LEANNA KATIGBAKNo ratings yet
- The Respiratory SystemDocument58 pagesThe Respiratory SystemFRANCEEN LEANNA KATIGBAKNo ratings yet
- Isolation From Chicken Liver and Enzymatic Hydrolysis of GlycogenDocument2 pagesIsolation From Chicken Liver and Enzymatic Hydrolysis of GlycogenAngela ResicoNo ratings yet
- Respiratory System: DR Archna Ghildiyal Associate ProfessorDocument35 pagesRespiratory System: DR Archna Ghildiyal Associate ProfessorFRANCEEN LEANNA KATIGBAKNo ratings yet
- Glycogen Isolation and Determination ofDocument14 pagesGlycogen Isolation and Determination ofChristian De LeonNo ratings yet
- Glycogen Isolation and Determination ofDocument14 pagesGlycogen Isolation and Determination ofChristian De LeonNo ratings yet
- Before Getting Started, Spend One Minute of Silence For Opening PrayerDocument47 pagesBefore Getting Started, Spend One Minute of Silence For Opening PrayerFRANCEEN LEANNA KATIGBAKNo ratings yet
- 0 - Cece's Study Guides Part 2Document25 pages0 - Cece's Study Guides Part 2FRANCEEN LEANNA KATIGBAK100% (6)
- Isolation From Chicken Liver and Enzymatic Hydrolysis of GlycogenDocument2 pagesIsolation From Chicken Liver and Enzymatic Hydrolysis of GlycogenAngela ResicoNo ratings yet
- Qualitative Tests For Carbohydrates: 1) Molisch TestDocument20 pagesQualitative Tests For Carbohydrates: 1) Molisch TestFRANCEEN LEANNA KATIGBAKNo ratings yet
- Mathematics in Our WorldDocument15 pagesMathematics in Our WorldFRANCEEN LEANNA KATIGBAKNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Angle of Depression Lesson for Grade 9 MathDocument6 pagesAngle of Depression Lesson for Grade 9 MathPatrick Guerra100% (1)
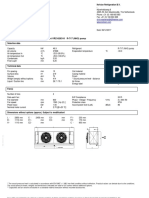
- 6kW V2G EV Charger Module Datasheet (2018)Document2 pages6kW V2G EV Charger Module Datasheet (2018)pysogaNo ratings yet
- Waste Management in Vienna. MA 48Document12 pagesWaste Management in Vienna. MA 484rtttt4ttt44No ratings yet
- Fesh S A0001171549 1Document7 pagesFesh S A0001171549 1ismuNo ratings yet
- Audit Keselamatan Jalan Pada Jalan Yogyakarta-Purworejo KM 35-40, Kulon Progo, YogyakartaDocument10 pagesAudit Keselamatan Jalan Pada Jalan Yogyakarta-Purworejo KM 35-40, Kulon Progo, YogyakartaSawaluddin SawalNo ratings yet
- Alaina W - Food Project ReflectionDocument1 pageAlaina W - Food Project Reflectionapi-438601399No ratings yet
- Mathematical Structures of The UniverseDocument228 pagesMathematical Structures of The UniverseMaki MajomNo ratings yet
- PR900 Operator ManualDocument21 pagesPR900 Operator ManualAlan TanNo ratings yet
- GSL DIP Phase - 1 Cooler 45kWDocument1 pageGSL DIP Phase - 1 Cooler 45kWMuhasin PallikkalNo ratings yet
- Negative Compressibility and PVT Extrapolation WarningsDocument17 pagesNegative Compressibility and PVT Extrapolation WarningsMarcelo SaezNo ratings yet
- Beneficiation of Cassiterite From Primary Tin OresDocument11 pagesBeneficiation of Cassiterite From Primary Tin OresSULMAGNo ratings yet
- El Anatsui - TransformationsDocument15 pagesEl Anatsui - TransformationsReece BriceNo ratings yet
- Miniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDocument4 pagesMiniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDenis CarlosNo ratings yet
- Detailed Lesson Plan Boyle's LawDocument9 pagesDetailed Lesson Plan Boyle's LawTeacher Derick Daet86% (7)
- Material ManagementDocument106 pagesMaterial ManagementRomi AfriansyahNo ratings yet
- Fi & EiDocument3 pagesFi & EiPrasanna S Kulkarni100% (1)
- Rational Use of AntibioticsDocument35 pagesRational Use of AntibioticsRahul SharmaNo ratings yet
- CH 2.2: Separable Equations: X F DX DyDocument9 pagesCH 2.2: Separable Equations: X F DX DyPFENo ratings yet
- Marketing 5 0Document23 pagesMarketing 5 0gmusicestudioNo ratings yet
- Measurement of Level in A Tank Using Capacitive Type Level ProbeDocument13 pagesMeasurement of Level in A Tank Using Capacitive Type Level ProbeChandra Sekar100% (1)
- MayankDocument38 pagesMayankmayank13430No ratings yet
- 22 Imobilisasi Pada Usia LanjutDocument34 pages22 Imobilisasi Pada Usia LanjutGian KalalembangNo ratings yet
- #10 VHB SGT-APT Design SummaryDocument2 pages#10 VHB SGT-APT Design SummarySenthil KumarNo ratings yet
- Char Lynn 104 2000 Series Motor Data SheetDocument28 pagesChar Lynn 104 2000 Series Motor Data Sheetsyahril boonieNo ratings yet
- ES vs SIGINT: Understanding the DifferencesDocument9 pagesES vs SIGINT: Understanding the DifferencesYasir ShigileeniNo ratings yet
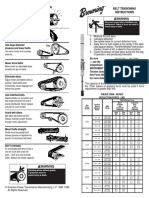
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- Mechanical Design of Turine EginesDocument51 pagesMechanical Design of Turine EginessriniNo ratings yet
- Blackmer Pump Parts ListDocument2 pagesBlackmer Pump Parts ListFelipe Ignacio PaillavilNo ratings yet
- GTA San Andreas CheatDocument9 pagesGTA San Andreas CheatHatta YanuarNo ratings yet
- MUSCULAR SYSTEM WORKSHEET Slides 1 To 4Document4 pagesMUSCULAR SYSTEM WORKSHEET Slides 1 To 4kwaiyuen ohnNo ratings yet