You might also like
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Vital SignsDocument45 pagesVital SignsQashqar & GB FolksNo ratings yet
- This Learning Unit Is Developed To Provide The Trainees The Necessary Information Regarding The Following Contents Taking Patient's Vital SignsDocument30 pagesThis Learning Unit Is Developed To Provide The Trainees The Necessary Information Regarding The Following Contents Taking Patient's Vital Signsworkukid16No ratings yet
- Cardiovascular History Taking and Physical ExaminationsDocument35 pagesCardiovascular History Taking and Physical ExaminationsEndalk AsfawNo ratings yet
- demonstration on bp (1)Document7 pagesdemonstration on bp (1)pritidinda3070No ratings yet
- Cardiovascular Assessment DDocument8 pagesCardiovascular Assessment Davinash dhameriyaNo ratings yet
- Osce Notes - Rac - Safina AdatiaDocument35 pagesOsce Notes - Rac - Safina AdatiaTraventure 2000No ratings yet
- Chapter 07 Taking Vital SignsDocument22 pagesChapter 07 Taking Vital SignsNephNo ratings yet
- Vital SignDocument40 pagesVital SignYoelBagusGiarto0% (1)
- RLE 2 - Lecture On Vital SignsDocument59 pagesRLE 2 - Lecture On Vital SignsIrah Joy MarianoNo ratings yet
- Taking Vital Signs of A PatientDocument28 pagesTaking Vital Signs of A PatientkavithsamuelNo ratings yet
- 6 - CH 27-Vital SignsDocument62 pages6 - CH 27-Vital SignsmohannadaudehNo ratings yet
- Blood Pressure MeasurementDocument84 pagesBlood Pressure MeasurementDalia Ali El EbeedyNo ratings yet
- Faqs BayonetoDocument37 pagesFaqs BayonetoLianne BayonetoNo ratings yet
- CardiacassessmentDocument40 pagesCardiacassessmentsasNo ratings yet
- KN 4@enzl 8 Ha 4 B 6 CC 9 eDocument26 pagesKN 4@enzl 8 Ha 4 B 6 CC 9 eRamzen Raphael DomingoNo ratings yet
- Critical Care and Small Bowel ObstructionDocument16 pagesCritical Care and Small Bowel Obstructionsofea zamriNo ratings yet
- Meet Personal Care Needs Through Vital Signs SupportDocument45 pagesMeet Personal Care Needs Through Vital Signs SupportRodel AgapitoNo ratings yet
- Cardiovascular 4416Document5 pagesCardiovascular 4416api-3703191No ratings yet
- HANDOUTS Brain SurgeryDocument3 pagesHANDOUTS Brain SurgerynieltresNo ratings yet
- Vital Signs: Understanding Body Temperature, Pulse, Respiration Rate & Blood PressureDocument69 pagesVital Signs: Understanding Body Temperature, Pulse, Respiration Rate & Blood PressureSamantha SunglaoNo ratings yet
- Vital Signs/'Document30 pagesVital Signs/'Monika MinhasNo ratings yet
- Cardiopulmon ARY Resuscitation: by Karen Ruth M.SC Nursing 1st Year 220240417Document17 pagesCardiopulmon ARY Resuscitation: by Karen Ruth M.SC Nursing 1st Year 220240417swatiNo ratings yet
- Anatomy and Pathophysiology G3Document17 pagesAnatomy and Pathophysiology G3Elva Borlado BilocuraNo ratings yet
- Cardiovascular Assessment (1) - StudentsDocument70 pagesCardiovascular Assessment (1) - Studentsraima ayazNo ratings yet
- Module 2 Full SlidesDocument69 pagesModule 2 Full SlidesMaria Du-PastoralNo ratings yet
- Vital Signs and TestingDocument47 pagesVital Signs and TestingRegina Garrard100% (1)
- Cvs ExaminationDocument21 pagesCvs Examinationwizborrlyzo006No ratings yet
- Assessing Pulse TechniquesDocument29 pagesAssessing Pulse TechniquesRaRe TVNo ratings yet
- Fundamentals Vital Signs ReviewDocument94 pagesFundamentals Vital Signs Reviewymitchell7No ratings yet
- Vital Signs and Oxygen AdministrationDocument11 pagesVital Signs and Oxygen AdministrationCrisha Shane BoticarioNo ratings yet
- Diara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineDocument19 pagesDiara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineJara RogacionNo ratings yet
- Med-Surg Exam #3 Study GuideDocument43 pagesMed-Surg Exam #3 Study GuideCaitlyn BilbaoNo ratings yet
- RCSI Clinical Examinations in Medicine 2018-19Document189 pagesRCSI Clinical Examinations in Medicine 2018-19Rebecca MarshallNo ratings yet
- 4-BLOOD-PRESSURE-TAKING (2)Document38 pages4-BLOOD-PRESSURE-TAKING (2)Danica DaniotNo ratings yet
- Vital Signs Study Guide Packet 2 Ex 1Document8 pagesVital Signs Study Guide Packet 2 Ex 1Emily StoicovyNo ratings yet
- Vital SignsDocument63 pagesVital SignsAlvin JavierNo ratings yet
- Define Blood Pressure FinalDocument11 pagesDefine Blood Pressure FinalNowshad T 1 8 1 0 2 6No ratings yet
- Vital Signs: Body Temperature, Pulse, Respiration, Blood PressureDocument31 pagesVital Signs: Body Temperature, Pulse, Respiration, Blood PressureYathziel Meow100% (4)
- 03 Vital Signs Assessment NEWDocument38 pages03 Vital Signs Assessment NEWAhmad SobihNo ratings yet
- History and Examinatoin of The Cardiovascular SystemDocument47 pagesHistory and Examinatoin of The Cardiovascular Systemmawada abdallaNo ratings yet
- Vital SignDocument45 pagesVital SignGabbe HutapeaNo ratings yet
- Thoracic Trauma - Navy - PSPD 2021Document45 pagesThoracic Trauma - Navy - PSPD 2021Naavy LaksmonoNo ratings yet
- Disusun Oleh: 1.maya Fujiyanti 2.defina 3.rismayanti WidiyaningsihDocument10 pagesDisusun Oleh: 1.maya Fujiyanti 2.defina 3.rismayanti WidiyaningsihDefina 17No ratings yet
- MTE DR Mefri Cardiac ExaminationDocument36 pagesMTE DR Mefri Cardiac ExaminationMuhammad Thariq Isnaini100% (1)
- Vital SignsDocument44 pagesVital SignstabiNo ratings yet
- 52pengkajian Gawat DaruratDocument47 pages52pengkajian Gawat DaruratBintari PutriNo ratings yet
- Chest Pain: (See Also Harrison's Principles of Internal Medicine, 17 Edition, Chapter 13)Document10 pagesChest Pain: (See Also Harrison's Principles of Internal Medicine, 17 Edition, Chapter 13)Marwan M.No ratings yet
- Assisting Lumbar Puncture: By: Bonifacio P. Marilao Jr. Kirstine Anne Camille F. NuezDocument25 pagesAssisting Lumbar Puncture: By: Bonifacio P. Marilao Jr. Kirstine Anne Camille F. NuezTheSweetpea501No ratings yet
- Lumbar Puncture: CME 9/12/2019 by Sharon JesiccaDocument18 pagesLumbar Puncture: CME 9/12/2019 by Sharon JesiccaSharon J StephenNo ratings yet
- Measuring BPDocument39 pagesMeasuring BPMaaz KhanNo ratings yet
- Freemedicalbooks 4 DownloadDocument98 pagesFreemedicalbooks 4 Downloadموسى التميميNo ratings yet
- 1 - Vital SignsDocument27 pages1 - Vital Signshawdeng xalitNo ratings yet
- How To Take The Vital Signs of TheDocument19 pagesHow To Take The Vital Signs of TheDanielle ReginaldoNo ratings yet
- Pediatric ConceptDocument19 pagesPediatric ConceptAntonio Intia IVNo ratings yet
- Monitoring Blood Pressure: Presentation By:-Vansh Purohit Class:-Vii A Bangur Public School Guided By:-Shri Rajat SirDocument22 pagesMonitoring Blood Pressure: Presentation By:-Vansh Purohit Class:-Vii A Bangur Public School Guided By:-Shri Rajat Sirpurohit_manishNo ratings yet
- Critical CareDocument21 pagesCritical Carepaulzilicous.artNo ratings yet
- Cardiognic Pulmonary EdemaDocument41 pagesCardiognic Pulmonary EdemaDeepak BenjaminNo ratings yet
- Heart FailureDocument21 pagesHeart FailureJazzy Kathlene Dumable0% (1)
- CRT Exam Review Guide Chapter 11Document11 pagesCRT Exam Review Guide Chapter 11Dharlyn MungcalNo ratings yet
- CRT Exam Review Guide Chapter 10Document20 pagesCRT Exam Review Guide Chapter 10Dharlyn MungcalNo ratings yet
- CRT Exam Review Guide Chapter 8Document10 pagesCRT Exam Review Guide Chapter 8Dharlyn MungcalNo ratings yet
- CRT Exam Review Guide Chapter 15Document27 pagesCRT Exam Review Guide Chapter 15Dharlyn MungcalNo ratings yet
- CRT Exam Review Guide Chapter 8Document10 pagesCRT Exam Review Guide Chapter 8Dharlyn MungcalNo ratings yet
- Chapter 34 Emergency Cardiovascular SystemDocument24 pagesChapter 34 Emergency Cardiovascular SystemDharlyn MungcalNo ratings yet
- Sin Tax Reform in The Philippines: Transforming Public Finance, Health, and Governance For More Inclusive DevelopmentDocument149 pagesSin Tax Reform in The Philippines: Transforming Public Finance, Health, and Governance For More Inclusive DevelopmentDharlyn MungcalNo ratings yet
- FEU Review Pre Board Exam 2016 PathophysioDocument8 pagesFEU Review Pre Board Exam 2016 PathophysioDharlyn MungcalNo ratings yet
- Chapter 41 Respiratory Failure and The Need For Ventilatory SupportDocument18 pagesChapter 41 Respiratory Failure and The Need For Ventilatory SupportDharlyn MungcalNo ratings yet
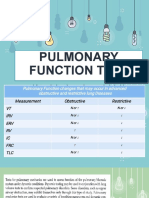
- Pulmonary Function TestDocument56 pagesPulmonary Function TestDharlyn MungcalNo ratings yet
- Copy-Of-Chapter 39 Lung Expansion TherapyDocument21 pagesCopy-Of-Chapter 39 Lung Expansion TherapyMaxinne GorospeNo ratings yet
- FEU Review Pre Board Exam 2016 NeoPediaDocument9 pagesFEU Review Pre Board Exam 2016 NeoPediaDharlyn MungcalNo ratings yet
- The Respirator Y System: Mungcal, Dharlynette RTRPDocument158 pagesThe Respirator Y System: Mungcal, Dharlynette RTRPDharlyn MungcalNo ratings yet
- AO No. 278Document4 pagesAO No. 278Dharlyn MungcalNo ratings yet
- Quality Assurance for Pulmonary Function Testing (PFTDocument26 pagesQuality Assurance for Pulmonary Function Testing (PFTDharlyn MungcalNo ratings yet
- Pulmonary Function Tests ExplainedDocument142 pagesPulmonary Function Tests ExplainedDharlyn MungcalNo ratings yet
- RT Curriculum MapDocument7 pagesRT Curriculum MapDharlyn MungcalNo ratings yet
- Pulmo Management Week 1Document160 pagesPulmo Management Week 1Dharlyn MungcalNo ratings yet
- Cardiovascular System: Mungcal, Dharlynette RTRPDocument77 pagesCardiovascular System: Mungcal, Dharlynette RTRPDharlyn MungcalNo ratings yet
- THE CIRCULATORY SYSTEMDocument47 pagesTHE CIRCULATORY SYSTEMDharlyn MungcalNo ratings yet
- FinalsDocument65 pagesFinalsDharlyn MungcalNo ratings yet
- Comprehensive Respiratory InterviewDocument36 pagesComprehensive Respiratory InterviewDharlyn MungcalNo ratings yet
- The Respiratory System: Mungcal, Dharlynette RTRPDocument85 pagesThe Respiratory System: Mungcal, Dharlynette RTRPDharlyn MungcalNo ratings yet
- Common Cardiopulmonary SymptomsDocument73 pagesCommon Cardiopulmonary SymptomsDharlyn MungcalNo ratings yet
- Evaluation of The AirwayDocument12 pagesEvaluation of The AirwayDharlyn MungcalNo ratings yet
- The Comprehensive Respiratory Therapist Exam Review - Entry and Advanced Levels, 5e (PDFDrive)Document673 pagesThe Comprehensive Respiratory Therapist Exam Review - Entry and Advanced Levels, 5e (PDFDrive)Dharlyn MungcalNo ratings yet
- Patient Safety, Communication and RecordkeepingDocument49 pagesPatient Safety, Communication and RecordkeepingDharlyn MungcalNo ratings yet
- Stress Brain PlasticityDocument15 pagesStress Brain PlasticityLilian Cerri MazzaNo ratings yet
- Hospitalized 67-Year-Old Black Woman MIDocument2 pagesHospitalized 67-Year-Old Black Woman MIMaria Jessica DumdumNo ratings yet
- PVS PDF H.Gul PDFDocument34 pagesPVS PDF H.Gul PDFUbaid ullah khanNo ratings yet
- CH 14 Lymphatic Practice ExDocument10 pagesCH 14 Lymphatic Practice ExSharina Marie CoderaNo ratings yet
- Screening Models for Centrally and Peripherally Acting Muscle RelaxantsDocument32 pagesScreening Models for Centrally and Peripherally Acting Muscle RelaxantsGeethika GummadiNo ratings yet
- CCU NCP Week 2Document4 pagesCCU NCP Week 2April Kate BanagodosNo ratings yet
- The Vascular System Allows For The Transport of Water, Minerals, and SugarsDocument7 pagesThe Vascular System Allows For The Transport of Water, Minerals, and SugarsHasan AlzaghalNo ratings yet
- Respiratory AlkalosisDocument17 pagesRespiratory AlkalosisGhen CanosaNo ratings yet
- Digestive and Respiratory System ExamDocument3 pagesDigestive and Respiratory System ExamAnonymous zGjXogXNo ratings yet
- Q3 Science 10 Module 3Document26 pagesQ3 Science 10 Module 3Rizalyn Patalinghug100% (1)
- CHF: Exercise Therapy for Heart Failure ManagementDocument20 pagesCHF: Exercise Therapy for Heart Failure ManagementJoeNo ratings yet
- 5e LINGERING INJURY TABLEDocument1 page5e LINGERING INJURY TABLEPhongbui0% (1)
- Acute Myocardial InfarctionDocument3 pagesAcute Myocardial InfarctionKrizel Anne DeriNo ratings yet
- Physical Education and Health 4 ModuleDocument38 pagesPhysical Education and Health 4 ModuleLouise ArellanoNo ratings yet
- 18 ExcretionDocument70 pages18 ExcretionqingxuguNo ratings yet
- Chronic Inappropriate Sinus Tachycardia (Lopera)Document5 pagesChronic Inappropriate Sinus Tachycardia (Lopera)Raymond BernardusNo ratings yet
- Optimizing Red Blood Cell Transfusion Practice: S. D. Surgenor, M. Hampers, and H. L. CorwinDocument10 pagesOptimizing Red Blood Cell Transfusion Practice: S. D. Surgenor, M. Hampers, and H. L. CorwinnadaNo ratings yet
- AR06894-Vigileo UserManual 1LRDocument31 pagesAR06894-Vigileo UserManual 1LRsec.ivbNo ratings yet
- Emergency Cardiovascular Life SupportDocument88 pagesEmergency Cardiovascular Life SupportMARK JOSHUA CRUZNo ratings yet
- HSC Biology: Maintaining BalanceDocument44 pagesHSC Biology: Maintaining BalanceMarcius MosesNo ratings yet
- Yoshida Et Al-2019-Intensive Care MedicineDocument4 pagesYoshida Et Al-2019-Intensive Care MedicineEduardo SemblanoNo ratings yet
- The Phoenix Protocol Dry Fasting For Rapid Healing and Radical Life Extension (August Dunning) (Z-Library)Document124 pagesThe Phoenix Protocol Dry Fasting For Rapid Healing and Radical Life Extension (August Dunning) (Z-Library)amitlkoyogaNo ratings yet
- Conduction of Cardiac ImpulseDocument18 pagesConduction of Cardiac Impulserera_avisNo ratings yet
- The Brain and Nervous System (Psychology) Unit 14: An Academic ReportDocument7 pagesThe Brain and Nervous System (Psychology) Unit 14: An Academic ReportOlatokunbo SinaayomiNo ratings yet
- BIOLOGY- HOMEOSTASIS REGULATIONDocument16 pagesBIOLOGY- HOMEOSTASIS REGULATIONJuliana NorNo ratings yet
- ECG Notes - 1 PDFDocument78 pagesECG Notes - 1 PDFAzizan HannyNo ratings yet
- ATLS PretestDocument133 pagesATLS Pretestmarcelina100% (1)
- CJM SepsisDocument1 pageCJM Sepsisapi-688564858No ratings yet
- PE 104 Notes - Final-1Document22 pagesPE 104 Notes - Final-1Cheryl GabianaNo ratings yet
- Guruji Pranayama SadhanaDocument9 pagesGuruji Pranayama SadhanaTito AlhoNo ratings yet