You might also like
- A Simple Guide to Capillary Leak Syndrome, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Capillary Leak Syndrome, Diagnosis, Treatment and Related ConditionsNo ratings yet
- RADBIOLOGY Ievan Dred Balmores OriginalDocument15 pagesRADBIOLOGY Ievan Dred Balmores OriginalMichaela Marie DimasNo ratings yet
- Radio SensitivityDocument29 pagesRadio SensitivitykarthikhrajvNo ratings yet
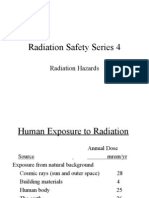
- Radiation Saftey Series 4Document26 pagesRadiation Saftey Series 4johntoblerNo ratings yet
- Radiation PoisioningDocument28 pagesRadiation PoisioningArunNo ratings yet
- Local Media8323395636333577285Document8 pagesLocal Media8323395636333577285Haimen BuisanNo ratings yet
- Science of Nuclear Energy and RadiationDocument32 pagesScience of Nuclear Energy and RadiationdrjatinNo ratings yet
- Biological Effect of RadiationDocument31 pagesBiological Effect of RadiationLokesh KandyNo ratings yet
- Biological Effects of RadiationDocument15 pagesBiological Effects of RadiationShaikh SalmanNo ratings yet
- Radiation BiologyDocument43 pagesRadiation Biologyaiimsjdh acadNo ratings yet
- Bahasa Indo Bahasa InggrisDocument17 pagesBahasa Indo Bahasa Inggrisdzy2ryr7d2No ratings yet
- Biological Effects of RadiationDocument7 pagesBiological Effects of Radiationbpvarian100% (1)
- SAR PPT 1-Program - 07Document36 pagesSAR PPT 1-Program - 07ni60No ratings yet
- Biological Effects of Radiation: Sayan Samanta BWU/BRI/21/109Document10 pagesBiological Effects of Radiation: Sayan Samanta BWU/BRI/21/109Sayan SamantaNo ratings yet
- Biological Effect of Ionizing Radiation Lecture MODIFIEDDocument58 pagesBiological Effect of Ionizing Radiation Lecture MODIFIEDHitesh RaoNo ratings yet
- Ars Physician Fact SheetDocument6 pagesArs Physician Fact SheetThiago CesarNo ratings yet
- Chapter - 2-Biological Effects of Ionizing RadiationDocument25 pagesChapter - 2-Biological Effects of Ionizing RadiationHayat MuljanaNo ratings yet
- Tourism Advantages and DisadvantagesDocument9 pagesTourism Advantages and DisadvantagessatishwararaoNo ratings yet
- Combined Diseases of Military TherapyDocument31 pagesCombined Diseases of Military TherapyDonesan GowarippriyanNo ratings yet
- Time, Dose & FractionationDocument63 pagesTime, Dose & FractionationLikhon Amin AponNo ratings yet
- PsoriasisDocument25 pagesPsoriasisAshish SNo ratings yet
- Lectures in Patient Care Management Prepared By. Rodel E. Agapito, RRT CommunicationDocument9 pagesLectures in Patient Care Management Prepared By. Rodel E. Agapito, RRT CommunicationRodel AgapitoNo ratings yet
- Biological Effects of Ionizing Radiation: En. Mohd Fahmi B Mohd YusofDocument45 pagesBiological Effects of Ionizing Radiation: En. Mohd Fahmi B Mohd YusofFahmi BestNo ratings yet
- Disease Caused by RadiationDocument17 pagesDisease Caused by RadiationHam ZaNo ratings yet
- Updated Biological Effects X Rays (2663)Document28 pagesUpdated Biological Effects X Rays (2663)AA HHNo ratings yet
- Dolquine: Rheumatoi D ArthritisDocument24 pagesDolquine: Rheumatoi D Arthritisali laftaNo ratings yet
- Radiobiology 5Document31 pagesRadiobiology 5joaNo ratings yet
- Chapter 23Document82 pagesChapter 23mohadese bideshkiNo ratings yet
- Late Effects of Cancer Treatment 1Document39 pagesLate Effects of Cancer Treatment 1Hifza BalouchNo ratings yet
- Radiation Biology LectureDocument39 pagesRadiation Biology LectureBipin UpadhyayNo ratings yet
- Sleep Disorders in The ElderlyDocument22 pagesSleep Disorders in The ElderlyJalajarani SelvaNo ratings yet
- Radiation Biology OR RadiobiologyDocument36 pagesRadiation Biology OR RadiobiologyVidhyaNo ratings yet
- RadiobiologyDocument70 pagesRadiobiologypia toledoNo ratings yet
- Lesson 1 - Cell InjuryDocument69 pagesLesson 1 - Cell InjuryAY 700No ratings yet
- Delirium Tremens: Most Serious Alcohol Withdrawal Phenomena Mortality of Up To 5%Document17 pagesDelirium Tremens: Most Serious Alcohol Withdrawal Phenomena Mortality of Up To 5%fagadgNo ratings yet
- Practice QuestionDocument36 pagesPractice QuestionAnna Kay BrownNo ratings yet
- Biological Effects - Direct and Indirect - Trần Văn TiếnDocument14 pagesBiological Effects - Direct and Indirect - Trần Văn TiếnHgwergweg GwqegwNo ratings yet
- Stochastic and Deterministic Effects of Radiation? AnswerDocument3 pagesStochastic and Deterministic Effects of Radiation? AnswerzahidNo ratings yet
- Lepromatous Leprosy in A Patient With B-Cell Lymphoma and Tubulointerstitial NephritisDocument4 pagesLepromatous Leprosy in A Patient With B-Cell Lymphoma and Tubulointerstitial NephritisDar LynnNo ratings yet
- Radpatho IntroDocument58 pagesRadpatho IntroJohn Paul MarasiganNo ratings yet
- Biologicaleffectsofradiation 220817141003 73bdb695Document10 pagesBiologicaleffectsofradiation 220817141003 73bdb695sspcontractionNo ratings yet
- 4 Early Effects of RadiationDocument50 pages4 Early Effects of RadiationAngelo RamosNo ratings yet
- Acute Lymphoblastic LeukemiaDocument3 pagesAcute Lymphoblastic LeukemiaMaria Luisa Rodriguez GarciaNo ratings yet
- Basic Radiation BiologyDocument25 pagesBasic Radiation Biologysazaki224No ratings yet
- Condition That Mimic Brain DeathDocument20 pagesCondition That Mimic Brain DeathTan Chuan Hsin100% (1)
- Radiology 72Document1 pageRadiology 72Irfan AliNo ratings yet
- Aging: The Biology of SenescenceDocument37 pagesAging: The Biology of SenescenceMaddox EdeyajNo ratings yet
- Bilogical Effects and RisksDocument33 pagesBilogical Effects and RisksVictor LusamboNo ratings yet
- LeukemiaDocument23 pagesLeukemiaMrnj MelorinNo ratings yet
- Fish and Shellfish Diseases U 2 C 1Document24 pagesFish and Shellfish Diseases U 2 C 1Thakur VeeruNo ratings yet
- Cellular AgingDocument22 pagesCellular AgingOlu FasanyaNo ratings yet
- Panel Discussion2Document26 pagesPanel Discussion2adystiNo ratings yet
- Introducing: General Cellular Effects of RadiationDocument40 pagesIntroducing: General Cellular Effects of RadiationLouella ArtatesNo ratings yet
- Basic Principles of Radiation OncologyDocument3 pagesBasic Principles of Radiation Oncologyhalf_frozen_cho6435No ratings yet
- Introducrion To PathologyDocument39 pagesIntroducrion To PathologyAyman ElsirNo ratings yet
- Bioloical Effects and Hazards of RadiationDocument19 pagesBioloical Effects and Hazards of Radiationnabawenda. joan.2019No ratings yet
- HUman Effect of RadiaitionDocument16 pagesHUman Effect of RadiaitionCrazzy PalNo ratings yet
- Radiation Units and Biological Effects of RadiationDocument67 pagesRadiation Units and Biological Effects of RadiationSivirahul100% (2)
- Surviving Leukemia and Hodgkin's Lymphoma: An Overview Of Effective Treatment MethodsFrom EverandSurviving Leukemia and Hodgkin's Lymphoma: An Overview Of Effective Treatment MethodsNo ratings yet
- Thesis MotivationDocument4 pagesThesis MotivationjoaNo ratings yet
- Questionnaire ResearchDocument4 pagesQuestionnaire ResearchjoaNo ratings yet
- Invitation Letters To Adviser Statistician and Editor CCADocument5 pagesInvitation Letters To Adviser Statistician and Editor CCAjoaNo ratings yet
- The Reproductive OrgansDocument39 pagesThe Reproductive OrgansjoaNo ratings yet
- Pe. BlancoDocument4 pagesPe. BlancojoaNo ratings yet
- Radiobiology 5Document31 pagesRadiobiology 5joaNo ratings yet
- Radiobiology 4Document24 pagesRadiobiology 4joaNo ratings yet
- Radiobiology 7Document25 pagesRadiobiology 7joaNo ratings yet
- 1 - Introduction To Clinical Hematology IDocument26 pages1 - Introduction To Clinical Hematology IJulliene DadoleNo ratings yet
- Blood Transfusion GuidelineDocument402 pagesBlood Transfusion GuidelineAdam Razi0% (1)
- Platelet CasesDocument13 pagesPlatelet CasesRaheel IftikharNo ratings yet
- PRP Review TemplateDocument15 pagesPRP Review TemplatedermoNo ratings yet
- Blood Clotting NotesDocument12 pagesBlood Clotting NotesFateh MohammadNo ratings yet
- Advances in Bioengineering PDFDocument384 pagesAdvances in Bioengineering PDFFernan David MartinezNo ratings yet
- Phlebotomy TestDocument11 pagesPhlebotomy TestRaquel Girón75% (4)
- Cardiovascular Disease and Diabetes: The Vulnerable Patient: Katharina Hess, Nikolaus Marx, and Michael LehrkeDocument10 pagesCardiovascular Disease and Diabetes: The Vulnerable Patient: Katharina Hess, Nikolaus Marx, and Michael Lehrkekrungi21No ratings yet
- Platelet-Rich Plasma (PRP) : What Is PRP and What Is Not PRP?Document4 pagesPlatelet-Rich Plasma (PRP) : What Is PRP and What Is Not PRP?Amanda PutriNo ratings yet
- Folleto PFA 100 SiemensDocument4 pagesFolleto PFA 100 SiemensSantiagoAFNo ratings yet
- Vitamin K TOFDocument5 pagesVitamin K TOFNanank Akhiruddin SyamsaNo ratings yet
- Transfusion in TraumaDocument28 pagesTransfusion in TraumaSyeda Nasra ShahNo ratings yet
- Immunohematology Notes Donor Screening Component Preparation Transfusion Reactions HDNDocument20 pagesImmunohematology Notes Donor Screening Component Preparation Transfusion Reactions HDNprnfbmsdqnNo ratings yet
- Myelo Blog PDFDocument158 pagesMyelo Blog PDFNino GumbanNo ratings yet
- Pathology NotesDocument29 pagesPathology NotesMK100% (1)
- Blood Banking - System RequirementsDocument24 pagesBlood Banking - System RequirementsJira Jinn ChuaNo ratings yet
- Blood Pharmacology PDFDocument13 pagesBlood Pharmacology PDFManikanta GupthaNo ratings yet
- Hematology 2 LaboratoryDocument11 pagesHematology 2 LaboratoryChristine BadilloNo ratings yet
- Diff Count SopDocument14 pagesDiff Count Soppesh4geoNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument14 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- ASRA Guidelines For CNBDocument66 pagesASRA Guidelines For CNBAshiyan IrfanNo ratings yet
- Patient Evaluat-WPS OfficeDocument109 pagesPatient Evaluat-WPS OfficeCounselor Optimus EduconNo ratings yet
- Mechanisms of Coagulation and Fibrinolysis (Autosaved)Document60 pagesMechanisms of Coagulation and Fibrinolysis (Autosaved)Tom Anthony TonguiaNo ratings yet
- MLS 12aa: Hematology 2 (Laboratory) : Module 2: Bleeding Time and Clottinfg TimeDocument9 pagesMLS 12aa: Hematology 2 (Laboratory) : Module 2: Bleeding Time and Clottinfg TimeRuphele Anne Quitag100% (1)
- L2-SURG-Hemostasis, Surgical Bleeding, - Transfusion (Aug2521)Document8 pagesL2-SURG-Hemostasis, Surgical Bleeding, - Transfusion (Aug2521)Marc Lyndon CafinoNo ratings yet
- HematologyDocument58 pagesHematologyAchmad DainuriNo ratings yet
- Goodnough, Shander & Brecher, 2003Document9 pagesGoodnough, Shander & Brecher, 2003Jetco LawNo ratings yet
- Hematologic Principles SGD PDFDocument5 pagesHematologic Principles SGD PDFJolaine ValloNo ratings yet
- Basic Principles of HemostasisDocument5 pagesBasic Principles of HemostasisSean Matthew100% (1)
- Scientific Discussion: 1/45 EMEA 2004Document45 pagesScientific Discussion: 1/45 EMEA 2004rabikantNo ratings yet