You might also like
- The Final Trimester: A Guide to Everything to Expect in the Third Trimester of Pregnancy and ChildbirthFrom EverandThe Final Trimester: A Guide to Everything to Expect in the Third Trimester of Pregnancy and ChildbirthRating: 5 out of 5 stars5/5 (1)
- Mom's Guide to Diastasis Recti: A Program for Preventing and Healing Abdominal Separation Caused by PregnancyFrom EverandMom's Guide to Diastasis Recti: A Program for Preventing and Healing Abdominal Separation Caused by PregnancyNo ratings yet
- Labor and Delivery TopicsDocument44 pagesLabor and Delivery TopicsAngela Joy AmparadoNo ratings yet
- Normal Labor and DeliveryDocument142 pagesNormal Labor and DeliveryRosalie RoselloNo ratings yet
- Intrapartum PeriodDocument19 pagesIntrapartum Periodanon_915924422No ratings yet
- Maternal and Child Care Skills for Labor and DeliveryDocument61 pagesMaternal and Child Care Skills for Labor and DeliveryboinkjilijoyNo ratings yet
- Stages of Labor: Definition, Signs, and OnsetDocument73 pagesStages of Labor: Definition, Signs, and OnsetBharat ThapaNo ratings yet
- Normal Labour 400lDocument102 pagesNormal Labour 400lAbdullahi Suleiman MakaNo ratings yet
- 1st and 2nd Stage of LabourDocument137 pages1st and 2nd Stage of Labournixon odoyoNo ratings yet
- Intrapartum Care: Maternal and Child Nursing NUR 362Document24 pagesIntrapartum Care: Maternal and Child Nursing NUR 362Keith Nester Arines LavinNo ratings yet
- Normal Labour: 4 Mbbs Class Esut College of Medicine 2013Document77 pagesNormal Labour: 4 Mbbs Class Esut College of Medicine 2013nonny100% (1)
- Intrapartal Period: Methods of Pain ManagementDocument7 pagesIntrapartal Period: Methods of Pain Managementdarkscaler100% (2)
- 4-Gynae Obs PT 24-04-2020Document35 pages4-Gynae Obs PT 24-04-2020DaniJaralNo ratings yet
- Stages of LaborDocument51 pagesStages of LaborZeen_Zeen_Fern_3128100% (4)
- Normal Labour and Birth Uoh 2023Document159 pagesNormal Labour and Birth Uoh 2023Caamir Dek HaybeNo ratings yet
- Normal Labour and Birth UohDocument148 pagesNormal Labour and Birth UohCaamir Dek HaybeNo ratings yet
- Intrapartal - Theories of LaborDocument21 pagesIntrapartal - Theories of LaborJan Oliver YaresNo ratings yet
- Crisanto Cajang Mariecor Enriquez Kathleen Jayne Ramos Kathleen Kayla Baguioen Rosemarie Joy JucutanDocument58 pagesCrisanto Cajang Mariecor Enriquez Kathleen Jayne Ramos Kathleen Kayla Baguioen Rosemarie Joy JucutanGary PicarNo ratings yet
- LabourDocument55 pagesLabourRobert Chileshe100% (1)
- NCM 107 - SL - Mat - 1Document100 pagesNCM 107 - SL - Mat - 1marilexdomagsangNo ratings yet
- Process of Labor and Delivery (Intrapartum)Document55 pagesProcess of Labor and Delivery (Intrapartum)Corpus, Irene Zen P.100% (2)
- Updated NCM 107 Lecture Week 7Document27 pagesUpdated NCM 107 Lecture Week 7Quencee CalaycayNo ratings yet
- LABOUR & DELIVERY STAGESDocument19 pagesLABOUR & DELIVERY STAGESahmed shorshNo ratings yet
- Presented By:-Ms. Annu Panchal Nursing TutorDocument11 pagesPresented By:-Ms. Annu Panchal Nursing Tutorangel panchalNo ratings yet
- Normal Labor Essential Factors Elements of Uterine Contractions & Physiology of 1 Stage of LaborDocument88 pagesNormal Labor Essential Factors Elements of Uterine Contractions & Physiology of 1 Stage of LaborAswathy Aswathy100% (1)
- Nursing Management During Stages of Labor and Delivery UpdatedDocument40 pagesNursing Management During Stages of Labor and Delivery UpdatedCharlmagne LinnamNo ratings yet
- Government College of Nursing:, Jodhpur (Raj.)Document6 pagesGovernment College of Nursing:, Jodhpur (Raj.)priyankaNo ratings yet
- Normal LaborDocument8 pagesNormal LaborNishaThakuri100% (2)
- Normal Labour July 2013Document13 pagesNormal Labour July 2013Logan MakolaNo ratings yet
- Obstetric & Gynecology Nursing: Topic-Physiological Changes During LabourDocument54 pagesObstetric & Gynecology Nursing: Topic-Physiological Changes During LabourBhumi ChouhanNo ratings yet
- Stages of LaborDocument5 pagesStages of Laborchrisanne09No ratings yet
- LabourDocument47 pagesLabourAnas H HijaziNo ratings yet
- Physiology of LaborDocument96 pagesPhysiology of LaborSaloni GanganNo ratings yet
- LaborDocument19 pagesLaborAMARDEEP KUMARNo ratings yet
- LaborDocument45 pagesLaborDakayu Amin LugitNo ratings yet
- Post-Partal Care GuideDocument174 pagesPost-Partal Care GuideBriana Louise HernandezNo ratings yet
- 10.theories of LaborDocument18 pages10.theories of LaborJulia Ramos100% (1)
- Stages of LaborDocument43 pagesStages of LaborMASII100% (1)
- Normal Labor and DeliveryDocument77 pagesNormal Labor and DeliveryLouis Carlos RoderosNo ratings yet
- Complications With The Power of LaborDocument8 pagesComplications With The Power of LaborEdrea Aquino MendezNo ratings yet
- 15 Signs Stages of LaborDocument84 pages15 Signs Stages of LaborDorothy Jane OrdinarioNo ratings yet
- Dra Juson Labor & DeliveryDocument153 pagesDra Juson Labor & DeliveryaringkinkingNo ratings yet
- Labor and Delivery CompleteDocument120 pagesLabor and Delivery Completegallegomarjorie16No ratings yet
- Intranatal CareDocument32 pagesIntranatal CareMnm Ikljh100% (1)
- Abnormal LaborDocument114 pagesAbnormal LaborMohammad AlrefaiNo ratings yet
- Management of First Stage of LabourDocument35 pagesManagement of First Stage of LabourPragati BholeNo ratings yet
- Process of LabourDocument6 pagesProcess of LabourAnnapurna Dangeti100% (1)
- n3633 MM Module 1 Unit 1Document71 pagesn3633 MM Module 1 Unit 1jonscastro450No ratings yet
- Abnormal Uterine Action GuideDocument27 pagesAbnormal Uterine Action Guidetanmai noolu100% (1)
- Intrapartal PeriodDocument6 pagesIntrapartal PeriodKelsey MacaraigNo ratings yet
- Wln-Normal LabourDocument45 pagesWln-Normal LabourEmmanuel MukukaNo ratings yet
- Normal Labor Process in 4 StagesDocument19 pagesNormal Labor Process in 4 StagesNishaThakuri100% (1)
- Signs of Labor and Theories of OnsetDocument13 pagesSigns of Labor and Theories of Onsetmamsh KlangNo ratings yet
- First Stage of Labour ExplainedDocument5 pagesFirst Stage of Labour ExplainedSucharita PandaNo ratings yet
- Stages of Labor & Leopold's Maneuver First Stage: Dilating StageDocument11 pagesStages of Labor & Leopold's Maneuver First Stage: Dilating StagePanJan BalNo ratings yet
- Normal Labour in Obstetric2Document17 pagesNormal Labour in Obstetric2Tejasvi ChavdaNo ratings yet
- Normal LaborDocument14 pagesNormal LaborJorge De VeraNo ratings yet
- Intrapartal Complications - JeceliDocument70 pagesIntrapartal Complications - JeceliJeceli A. NoblezaNo ratings yet
- Labor and DeliveryDocument99 pagesLabor and DeliverymaribeeNo ratings yet
- ARTS9 NCRomantic ARTDocument60 pagesARTS9 NCRomantic ARTAngela Joy AmparadoNo ratings yet
- NGT LavageDocument2 pagesNGT LavageAngela Joy AmparadoNo ratings yet
- Placenta PreviaDocument43 pagesPlacenta PreviaAngela Joy AmparadoNo ratings yet
- Hirchsprung PDFDocument25 pagesHirchsprung PDFAngela Joy AmparadoNo ratings yet
- Heart Disease During PregnancyDocument39 pagesHeart Disease During PregnancyAngela Joy AmparadoNo ratings yet
- Cmca LectureDocument21 pagesCmca LectureAngela Joy AmparadoNo ratings yet
- Disseminated Intravascular CoagulationDocument15 pagesDisseminated Intravascular CoagulationAngela Joy AmparadoNo ratings yet
- DIABETES MELLITUS IN PREGNANCYDocument38 pagesDIABETES MELLITUS IN PREGNANCYAngela Joy AmparadoNo ratings yet
- Health Care Ethics Research PrinciplesDocument60 pagesHealth Care Ethics Research PrinciplesAngela Joy AmparadoNo ratings yet
- Walang Pamagat Na DokumentoDocument11 pagesWalang Pamagat Na DokumentoAngela Joy AmparadoNo ratings yet
- Nursing Informatics Topic OutlineDocument23 pagesNursing Informatics Topic OutlineAngela Joy AmparadoNo ratings yet
- Nursing InformaticsDocument25 pagesNursing InformaticsAngela Joy AmparadoNo ratings yet
- Doh Programs Related To Family Health 2Document19 pagesDoh Programs Related To Family Health 2AnonymousTarget100% (1)
- Chapter 09 AntibioticsDocument77 pagesChapter 09 AntibioticsAngela Joy AmparadoNo ratings yet
- Chapter 14 AntineoplasticDocument37 pagesChapter 14 AntineoplasticAngela Joy AmparadoNo ratings yet
- Chapter 13 AntihilminticDocument20 pagesChapter 13 AntihilminticAngela Joy AmparadoNo ratings yet
- Chapter 16 Anti InflammDocument36 pagesChapter 16 Anti InflammAngela Joy AmparadoNo ratings yet
- LITE Unit 3Document60 pagesLITE Unit 3Angela Joy AmparadoNo ratings yet
- Postpartum Period 1Document93 pagesPostpartum Period 1Angela Joy AmparadoNo ratings yet
- Final Project in Ncm107 - Amparado, Angela Joy D.Document14 pagesFinal Project in Ncm107 - Amparado, Angela Joy D.Angela Joy AmparadoNo ratings yet
- Postpartum Period 1Document93 pagesPostpartum Period 1Angela Joy AmparadoNo ratings yet
- LITE Unit 1Document136 pagesLITE Unit 1Angela Joy AmparadoNo ratings yet
- Pregnancy Myths and Beliefs DebunkedDocument14 pagesPregnancy Myths and Beliefs DebunkedAngela Joy AmparadoNo ratings yet
- GE ELECT 3 – Living in the IT Era | 1st Sem, AY 2022-2023Document80 pagesGE ELECT 3 – Living in the IT Era | 1st Sem, AY 2022-2023Angela Joy AmparadoNo ratings yet
- Final Project in Ncm107 - Amparado, Angela Joy D - 2dDocument14 pagesFinal Project in Ncm107 - Amparado, Angela Joy D - 2dAngela Joy AmparadoNo ratings yet
- KMC ChecklistDocument2 pagesKMC ChecklistAngela Joy AmparadoNo ratings yet
- Evolution of Programming LanguagesDocument33 pagesEvolution of Programming LanguagesAngela Joy AmparadoNo ratings yet
- ICT 9 L03 Starting A C ProgramDocument23 pagesICT 9 L03 Starting A C ProgramAngela Joy AmparadoNo ratings yet
- How to Improve Your Self-Motivation Through Self-Confidence, Positive Thinking, Goal Setting and EnvironmentDocument21 pagesHow to Improve Your Self-Motivation Through Self-Confidence, Positive Thinking, Goal Setting and EnvironmentRose Anne100% (1)
- Thermogravimetric Analysis - TGA: Analyzing & TestingDocument20 pagesThermogravimetric Analysis - TGA: Analyzing & TestingRusitaDessyNo ratings yet
- Bonding BB1Document3 pagesBonding BB1DeveshNo ratings yet
- Periodontal DiseaseDocument4 pagesPeriodontal Diseasemojako_badboysNo ratings yet
- 2) Coa-Vitamin-Dsm-Lot # XW91707139-146 PDFDocument16 pages2) Coa-Vitamin-Dsm-Lot # XW91707139-146 PDFNaeem AnjumNo ratings yet
- How to Compost at Home: A Guide to the BasicsDocument10 pagesHow to Compost at Home: A Guide to the BasicsYeo Choon SengNo ratings yet
- Slide BP Texas City RefineryDocument20 pagesSlide BP Texas City Refineryamaleena_muniraNo ratings yet
- Etymology: StructureDocument2 pagesEtymology: StructureNaga VNo ratings yet
- Subsea Cable Floats: Rising To Your Undersea ChallengesDocument1 pageSubsea Cable Floats: Rising To Your Undersea ChallengesMAURICIO DE LOS SANTOS HERNANDEZNo ratings yet
- Dgca Module 06 Part 02Document15 pagesDgca Module 06 Part 02Deepak Choudhary DCNo ratings yet
- Midterm MMMDocument2 pagesMidterm MMMasdfghjkl zxcvbnmNo ratings yet
- Klubermatic Lubricant DispensersDocument13 pagesKlubermatic Lubricant Dispenserstatankise100% (1)
- Beta Analytic Presentation at NNFCC Conference - Linking Bio-Based Materials To Renewable Energy ProductionDocument25 pagesBeta Analytic Presentation at NNFCC Conference - Linking Bio-Based Materials To Renewable Energy ProductionBeta AnalyticNo ratings yet
- Medical Certificate: (Coaches, Assistant Coaches, Chaperone)Document1 pageMedical Certificate: (Coaches, Assistant Coaches, Chaperone)Keith Marinas Serquina100% (1)
- University of Groningen MagazineDocument14 pagesUniversity of Groningen MagazineKhanh Phuong PhamNo ratings yet
- RA 6541 National Building Code of The PH StandPipeDocument5 pagesRA 6541 National Building Code of The PH StandPipejungzki jungzkiNo ratings yet
- Cavab - kartı - numune (копия) (копия) (копия) (копия)Document2 pagesCavab - kartı - numune (копия) (копия) (копия) (копия)Javid NovruzovNo ratings yet
- 可汗语法48篇(明志教育推荐) PDFDocument163 pages可汗语法48篇(明志教育推荐) PDFtellmewhour100% (2)
- Installation Manual - ClimateWell SolarChiller - v9 - 33 - 4 - ENDocument31 pagesInstallation Manual - ClimateWell SolarChiller - v9 - 33 - 4 - ENtxaelo100% (1)
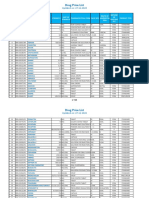
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- Antibiotic Susceptibility TestDocument5 pagesAntibiotic Susceptibility Testfarhanna8100% (3)
- Format Bahasa Inggeris UPSR 2016 ENGLISH (013) Section ADocument33 pagesFormat Bahasa Inggeris UPSR 2016 ENGLISH (013) Section AVINOTININo ratings yet
- Cases Digest on Adoption, Guardianship and Related LawsDocument2 pagesCases Digest on Adoption, Guardianship and Related LawsGillian BrionesNo ratings yet
- Letter From Springfield Mayor Sarno To License Commission Re: Late Night Hours.Document12 pagesLetter From Springfield Mayor Sarno To License Commission Re: Late Night Hours.Patrick JohnsonNo ratings yet
- Welfare Schemes in TelanganaDocument46 pagesWelfare Schemes in TelanganaNare ChallagondlaNo ratings yet
- MaryamDocument1 pageMaryamHAIZA FATHIMANo ratings yet
- Sattvik Brochure - Print VersionDocument6 pagesSattvik Brochure - Print Versionudiptya_papai2007No ratings yet
- Service Manual For High Efficiency High Ambient Amazon 20180726Document400 pagesService Manual For High Efficiency High Ambient Amazon 20180726Syedimam100% (1)
- F 856 - 97 - Rjg1ni05nw - PDFDocument7 pagesF 856 - 97 - Rjg1ni05nw - PDFRománBarciaVazquezNo ratings yet
- Sibling RivalryDocument2 pagesSibling Rivalrycarlokim14No ratings yet