You might also like
- Commonly Used IV Cardiac Medications For Adults Pocket Reference Card PDFDocument12 pagesCommonly Used IV Cardiac Medications For Adults Pocket Reference Card PDFYannis Zoldenberg100% (1)
- Adenovirus, Influenza, RSV, CMV, Parainfluenza, EBV: Most CommonDocument2 pagesAdenovirus, Influenza, RSV, CMV, Parainfluenza, EBV: Most CommonSoojung NamNo ratings yet
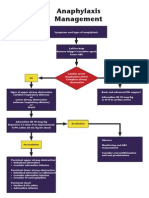
- Anaphylaxis Algorithm 2021Document1 pageAnaphylaxis Algorithm 2021Shawn Gaurav JhaNo ratings yet
- Health-Conditions Using Essential OilsDocument69 pagesHealth-Conditions Using Essential OilsHikari KoganeNo ratings yet
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 pagesPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- ASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFDocument8 pagesASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFAyu WahyuniNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis 2019Document8 pagesASCIA Guidelines Acute Management Anaphylaxis 2019Asadulla KhanNo ratings yet
- Systematic Review and Meta-Analysis MethodologyDocument7 pagesSystematic Review and Meta-Analysis MethodologyLaura Zuleta RestrepoNo ratings yet
- Work Life BalanceDocument25 pagesWork Life BalanceRamesh ArodiyaNo ratings yet
- Laporan Pendahuluan Sindrom Koroner Akut (Ska) I. Laporan PendahuluanDocument14 pagesLaporan Pendahuluan Sindrom Koroner Akut (Ska) I. Laporan PendahuluanBahiya Az ZahraNo ratings yet
- National EPI 2021 PDFDocument40 pagesNational EPI 2021 PDFyeabsira gashawNo ratings yet
- Introduction To Critical Care NursingDocument10 pagesIntroduction To Critical Care NursingAngielyn Ramos Oloraza100% (2)
- AnaphylaxisDocument39 pagesAnaphylaxisLydia Novalista100% (1)
- Penyegaran IKA 26mei2016Document79 pagesPenyegaran IKA 26mei2016arfanNo ratings yet
- Anaphylaxis & Allergic Reactions GuideDocument2 pagesAnaphylaxis & Allergic Reactions Guidemadimadi11No ratings yet
- AnaphylaxisDocument10 pagesAnaphylaxisMadyline VictoryaNo ratings yet
- Reaksi Anafilaksis: DR - Wisda Widiastuti, SPPD FK Universitas BaiturrahmahDocument26 pagesReaksi Anafilaksis: DR - Wisda Widiastuti, SPPD FK Universitas BaiturrahmahWulan afriNo ratings yet
- Poisoning II FinalDocument45 pagesPoisoning II FinalBi PinNo ratings yet
- Bronchial Asthma PDFDocument32 pagesBronchial Asthma PDFArpitha YadavalliNo ratings yet
- An A Phyla XisDocument2 pagesAn A Phyla XisNicole SolomonNo ratings yet
- 01 - Management of Critically Ill ChildrenDocument42 pages01 - Management of Critically Ill ChildrenMin MinTheinNo ratings yet
- PHC EmergencyDocument42 pagesPHC Emergencyمحمداحمد محمدنور ابايزيدNo ratings yet
- AnaphylaxisDocument1 pageAnaphylaxisherdind prayogaNo ratings yet
- Anaphylaxis - Second YearDocument3 pagesAnaphylaxis - Second YearBrian MaloneyNo ratings yet
- Anaphylactic ShockDocument25 pagesAnaphylactic ShockMaham BushraNo ratings yet
- Medical EmergenciesDocument9 pagesMedical EmergenciesThe KittyNo ratings yet
- Asthma 1Document79 pagesAsthma 1DanishMandiNo ratings yet
- Medical Emergency Part 2Document10 pagesMedical Emergency Part 2navyaNo ratings yet
- Drug Study (Aminophylline)Document2 pagesDrug Study (Aminophylline)Angel Mikaela CilladoNo ratings yet
- Algorithms - AnaphylaxisDocument1 pageAlgorithms - AnaphylaxisJude Roshan WijesiriNo ratings yet
- CMH PaedDocument33 pagesCMH PaedSowdatu Abdullah-SandyNo ratings yet
- General Anesthesia: Compiled By: Asad Arslan Source: Dr. Muhammad Aun SahbDocument21 pagesGeneral Anesthesia: Compiled By: Asad Arslan Source: Dr. Muhammad Aun SahbMr. AlphaNo ratings yet
- ASCIA HP Guidelines Acute Management Anaphylaxis 2020Document8 pagesASCIA HP Guidelines Acute Management Anaphylaxis 2020Munshi KamrulNo ratings yet
- Syok Anafilaksis 1Document4 pagesSyok Anafilaksis 1Mariatun Zahro NasutionNo ratings yet
- Status Asthmaticus: Triwahju AstutiDocument41 pagesStatus Asthmaticus: Triwahju AstutirianiNo ratings yet
- Acute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxisDocument8 pagesAcute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxissigmapomalNo ratings yet
- PediatricseizureDocument2 pagesPediatricseizureRifrita Fransisca HalimNo ratings yet
- Case Study Ufc FPDocument11 pagesCase Study Ufc FPMicah MagallanoNo ratings yet
- Presentation Medical Emergencies Lancaster 010212 (Compatibility Mode)Document97 pagesPresentation Medical Emergencies Lancaster 010212 (Compatibility Mode)Ffuture DoctorrNo ratings yet
- General Measure in The Management of PoisoningDocument43 pagesGeneral Measure in The Management of PoisoningCharlotte Anne Villero TiuNo ratings yet
- 3307 Wnhs Medicalemergencies A3posterDocument1 page3307 Wnhs Medicalemergencies A3posterNovie DamayantiNo ratings yet
- Versus: By: Kathleen Desouza & Rennette GarciaDocument14 pagesVersus: By: Kathleen Desouza & Rennette GarciakatNo ratings yet
- Anaph 5Document7 pagesAnaph 5Aprilihardini Laksmi100% (1)
- Drug StudyDocument2 pagesDrug StudyMec AmilasanNo ratings yet
- Medical EmergenciesDocument40 pagesMedical EmergenciesMuhammad Azeem Khan100% (1)
- Aclspediatric BradycardiaDocument2 pagesAclspediatric BradycardiasalamredNo ratings yet
- Medical EmergencyDocument3 pagesMedical EmergencyIbrar HumayunNo ratings yet
- Anaphylaxis - DR Dina MDocument31 pagesAnaphylaxis - DR Dina MimamNo ratings yet
- Anaphylaxis Wallchart 2018Document1 pageAnaphylaxis Wallchart 2018simranNo ratings yet
- Anaphylaxis TADocument54 pagesAnaphylaxis TAUriko ZoeNo ratings yet
- Bec Quick CardsDocument14 pagesBec Quick CardsUmidagha BaghirzadaNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportPrasad Narangoda100% (1)
- Drug Handbook ICNDocument16 pagesDrug Handbook ICNGrace CotesNo ratings yet
- Asthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic EczemaDocument14 pagesAsthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic EczemaTom Mallinson100% (1)
- Anaphylaxis Anaphylactoid ReactionDocument8 pagesAnaphylaxis Anaphylactoid Reactionsringeri2No ratings yet
- Anaphylaxis: By: O. Ahmadi, MD. Professor Assistant of Esfahan Medical School, Emergency Department of Al-Zahra HospitalDocument39 pagesAnaphylaxis: By: O. Ahmadi, MD. Professor Assistant of Esfahan Medical School, Emergency Department of Al-Zahra HospitalBudi SetyanugrahaNo ratings yet
- Allergic Reactions and AnaphylaxisDocument7 pagesAllergic Reactions and Anaphylaxisiffi82No ratings yet
- AnafilaxisDocument1 pageAnafilaxisalkutbiNo ratings yet
- Ammonia Algorithm v9Document5 pagesAmmonia Algorithm v9Danielle ConcepcionNo ratings yet
- Medical Emergencies of Dental Problems (Compatibility Mode)Document49 pagesMedical Emergencies of Dental Problems (Compatibility Mode)Saadi Bin QasimNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis Dec2016Document5 pagesASCIA Guidelines Acute Management Anaphylaxis Dec2016kkkssbbNo ratings yet
- .DR V P ChandrasekaranDocument61 pages.DR V P ChandrasekaranSaif ElayanNo ratings yet
- 038 AnaphylaxisDocument5 pages038 AnaphylaxisabbuahmedibbuNo ratings yet
- Case Study: Lumbar Spondylosis L3/L4 Related With L4/L5 Spinal StenosisDocument22 pagesCase Study: Lumbar Spondylosis L3/L4 Related With L4/L5 Spinal StenosisJohanes Rully BagaskaNo ratings yet
- Respiratory Diseases Summary MBBSDocument70 pagesRespiratory Diseases Summary MBBSIhsan PutraNo ratings yet
- ASV - Treatment Protocol.Document5 pagesASV - Treatment Protocol.Kayalvizhi ThirumalNo ratings yet
- Perinatal APRILDocument18 pagesPerinatal APRILSanjeewa KumaraNo ratings yet
- Severe Sepsis & Septic ShockDocument37 pagesSevere Sepsis & Septic ShockSanjeewa KumaraNo ratings yet
- Sepsis & Septic ShockDocument6 pagesSepsis & Septic ShockSanjeewa KumaraNo ratings yet
- Bronchial Asthma ManagementDocument14 pagesBronchial Asthma ManagementSanjeewa KumaraNo ratings yet
- Letter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Document10 pagesLetter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Cristina EneNo ratings yet
- DENTAL EXAMINATION - Transcript - TaggedDocument6 pagesDENTAL EXAMINATION - Transcript - Taggedpereiraortiz.tahinaNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyDocument100 pagesAneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyAndi rahma AnugrahNo ratings yet
- The Hidden Truths of The BellyDocument20 pagesThe Hidden Truths of The BellyRaimundo SousaNo ratings yet
- 3996 11820 1 SMDocument8 pages3996 11820 1 SMindah rahmaNo ratings yet
- Form 5 Cambridge VocabularyDocument7 pagesForm 5 Cambridge Vocabulary41 SHI YING WONGNo ratings yet
- National Health ProgrammesDocument12 pagesNational Health ProgrammesManpreet KaurNo ratings yet
- Guias DM1 PDFDocument127 pagesGuias DM1 PDFLalo LozanoNo ratings yet
- Grade 8 Health Q1Document21 pagesGrade 8 Health Q1Jayhia Malaga JarlegaNo ratings yet
- Name: Subject: Science Date: Sheet: The Immune SystemDocument1 pageName: Subject: Science Date: Sheet: The Immune SystemLibros Pdf100% (1)
- Operational Definition of TermsDocument1 pageOperational Definition of TermsJohn Lery SurellNo ratings yet
- Q A 1Document48 pagesQ A 1ChannelGNo ratings yet
- ? - Pedia MidtermsDocument18 pages? - Pedia Midtermsysabel.mendozaNo ratings yet
- Reproductive Health MCQs IDocument10 pagesReproductive Health MCQs IMahendhiran MariappanNo ratings yet
- Charles D Giordano CRNA, MSN (Major USAFR)Document51 pagesCharles D Giordano CRNA, MSN (Major USAFR)saritha OrugantiNo ratings yet
- LF0125A - Package Insert - Comfilcon A - Biofinity - Sphere Toric MultifocalDocument5 pagesLF0125A - Package Insert - Comfilcon A - Biofinity - Sphere Toric MultifocalSanela BajramovicNo ratings yet
- Hippo EM Board Review - Renal & GU Written SummaryDocument15 pagesHippo EM Board Review - Renal & GU Written Summarykaylawilliam01No ratings yet
- Adv Tech Stand Neurosurg 2011 (37) 213Document31 pagesAdv Tech Stand Neurosurg 2011 (37) 213Emilia MoreiroNo ratings yet
- Coauthors of Lifestyle Medicine BookDocument71 pagesCoauthors of Lifestyle Medicine Booknobertrotich12No ratings yet
- Mental Status Examination DefinitionsDocument8 pagesMental Status Examination DefinitionsCelebrity HubNo ratings yet
- Seed HealthTestingDocument9 pagesSeed HealthTestingMd. Sajjad HossenNo ratings yet
- Malaria Combat in ItalyDocument3 pagesMalaria Combat in ItalyBinh Pham ThanhNo ratings yet
- The Spine FrequenciesDocument2 pagesThe Spine Frequencieschris adiNo ratings yet