You might also like
- The Oxygen AdvantageDocument5 pagesThe Oxygen AdvantageJOHN0% (1)
- Urinary SystemDocument42 pagesUrinary Systemlil'sookie100% (2)
- 3BIdMvM5TsW9Xy8kMzZu Baby 4-18 Mo Sleep Guide Baby Sleep Dr. 2021Document98 pages3BIdMvM5TsW9Xy8kMzZu Baby 4-18 Mo Sleep Guide Baby Sleep Dr. 2021dragana novakovic100% (1)
- Airway ManagementDocument86 pagesAirway ManagementMUKESH SUNDARARAJANNo ratings yet
- Blood Banking QuestionsDocument18 pagesBlood Banking QuestionsDefensor Pison Gringgo82% (45)
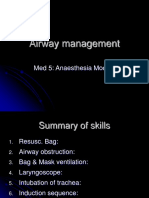
- Airway Management: Med 5: Anaesthesia ModuleDocument83 pagesAirway Management: Med 5: Anaesthesia Modulederek lauNo ratings yet
- Activity - Morning-Eveningness Questionnaire PDFDocument6 pagesActivity - Morning-Eveningness Questionnaire PDFVishal JainNo ratings yet
- Endotracheal IntubationDocument33 pagesEndotracheal IntubationReza Dyan Perdani ZeinNo ratings yet
- Exploring Science Edition © Pearson Education Limited 2008Document2 pagesExploring Science Edition © Pearson Education Limited 2008Victor Barber SanchisNo ratings yet
- Endotracheal IntubationDocument17 pagesEndotracheal IntubationShiwangi Sharma100% (1)
- Nasal Airway and Malocclucion / Orthodontic Courses by Indian Dental AcademyDocument35 pagesNasal Airway and Malocclucion / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Anatomy and Physiology of The Respiratory System (Handouts)Document5 pagesAnatomy and Physiology of The Respiratory System (Handouts)bluecindy87No ratings yet
- Management of Upper Airway DisorderDocument46 pagesManagement of Upper Airway DisorderSahana Rangarajan100% (1)
- Bms Professional Exams. Haematology - Mcqs Choose The Best Answer From A - EDocument10 pagesBms Professional Exams. Haematology - Mcqs Choose The Best Answer From A - ESAMMY100% (4)
- Anatomy and Physiology of Typhoid FeverDocument5 pagesAnatomy and Physiology of Typhoid FeverCharise Ligores67% (6)
- Airway Management Lecture-3Document28 pagesAirway Management Lecture-3maira ShahzadNo ratings yet
- CH - 3 Airway ManagementDocument45 pagesCH - 3 Airway ManagementHasnat AhmedNo ratings yet
- Sedation Airway ManagementDocument5 pagesSedation Airway ManagementMilana AndrewNo ratings yet
- AiwaryManagement 1Document72 pagesAiwaryManagement 1Giselle EstoquiaNo ratings yet
- Airway ManagementDocument11 pagesAirway Managementmegayani santosoNo ratings yet
- Basic Airway ManagementDocument98 pagesBasic Airway ManagementRani Salsabilah100% (1)
- AirwayDocument66 pagesAirwayMolina NaputriNo ratings yet
- Airway ManagementDocument29 pagesAirway Managementapi-142637023No ratings yet
- Airway Anatomy and AssessmentDocument69 pagesAirway Anatomy and AssessmentEvan Permana Putra100% (1)
- Skills Training Manual BookDocument19 pagesSkills Training Manual BookMuhammad SawalNo ratings yet
- Management of AirwaysDocument12 pagesManagement of AirwaysdyahNo ratings yet
- Airway Masterclass 2 TOTW 043 2007Document11 pagesAirway Masterclass 2 TOTW 043 2007eryxspNo ratings yet
- Basic Airway Management in AdultsDocument7 pagesBasic Airway Management in AdultsBereket temesgenNo ratings yet
- LECTURE4-Airway Management and Equipment-Dr ManaaDocument68 pagesLECTURE4-Airway Management and Equipment-Dr ManaasnezaimNo ratings yet
- ETT IntubationDocument10 pagesETT IntubationPoova RagavanNo ratings yet
- Airway Anatomy &assessmentDocument44 pagesAirway Anatomy &assessmentAya AlefeshatNo ratings yet
- Airway Management Topic 2Document8 pagesAirway Management Topic 2Lenard SakiliNo ratings yet
- Skills Laboratory: Manual Book Airway ManagementDocument25 pagesSkills Laboratory: Manual Book Airway ManagementAlif MusemNo ratings yet
- Oxygen AdministrationDocument38 pagesOxygen AdministrationKate Angelique RodriguezNo ratings yet
- Advanced Airway Management PrintableDocument8 pagesAdvanced Airway Management PrintableMiranda PermatasariNo ratings yet
- Airway Adjuncts 2Document9 pagesAirway Adjuncts 2Paul ButlerNo ratings yet
- SECTION 2 CHAPTER 4 Tracheal IntubationDocument46 pagesSECTION 2 CHAPTER 4 Tracheal IntubationRhea Andrea UyNo ratings yet
- - اطلس جهاز التخدير-30-34Document5 pages- اطلس جهاز التخدير-30-34علي الاسديNo ratings yet
- Airway ObstructionDocument32 pagesAirway ObstructionAmirrah LaurenteNo ratings yet
- Basic Anesthesia ManagementDocument78 pagesBasic Anesthesia ManagementCzar SyNo ratings yet
- Airway Management VentilationDocument13 pagesAirway Management Ventilationmariafer99No ratings yet
- Airway Management342 160121113511Document35 pagesAirway Management342 160121113511Glen DaleNo ratings yet
- Endotracheal Tube IntubationDocument5 pagesEndotracheal Tube IntubationKim Kristine D. GuillenNo ratings yet
- Respiratory Support: Intensive Care Nursery House Staff ManualDocument15 pagesRespiratory Support: Intensive Care Nursery House Staff ManualSedaka DonaldsonNo ratings yet
- Nasal ObstructionDocument6 pagesNasal Obstructionjoal510No ratings yet
- Airway Management-Dr RistiawanDocument75 pagesAirway Management-Dr RistiawanjavajavuNo ratings yet
- SuctioningDocument7 pagesSuctioningKat AlaNo ratings yet
- Tatalaksana Jalan NafasDocument49 pagesTatalaksana Jalan NafasSyaiful RochimNo ratings yet
- Respiratorydistressinthe Adultandfoal: Ashley G. BoyleDocument15 pagesRespiratorydistressinthe Adultandfoal: Ashley G. BoyleJuan Pardo CarrascoNo ratings yet
- Airway Management For ParamedicsDocument53 pagesAirway Management For ParamedicsNataliya PiletskaNo ratings yet
- Nose, Mouth, ThroutDocument78 pagesNose, Mouth, ThroutChaudhary AjayNo ratings yet
- Review of Respiratory ArrestDocument2 pagesReview of Respiratory ArrestsrimatsimhasaneshwarNo ratings yet
- Oxygen Administration ChecklistDocument3 pagesOxygen Administration ChecklistNoronisa D. CabugatanNo ratings yet
- Airway and The NurseDocument7 pagesAirway and The NursecarmenbuleandraNo ratings yet
- Procedure 400Document403 pagesProcedure 400Shilpa sharmaNo ratings yet
- Mechanical IntubationDocument5 pagesMechanical IntubationBAILEN AYNNA PEARLNo ratings yet
- Mid Oxygenation 2Document8 pagesMid Oxygenation 2Rhodessa Bhelle AntonioNo ratings yet
- Airway ManagmentDocument42 pagesAirway Managmentkader abdiNo ratings yet
- Maccon Fon TherapeuticDocument74 pagesMaccon Fon TherapeuticSM SunithaNo ratings yet
- Referat Intan FixDocument66 pagesReferat Intan FixElmo KrisnawanNo ratings yet
- Ilovepdf MergedDocument6 pagesIlovepdf Mergedharsh.patel180772No ratings yet
- Pulse OximetryDocument7 pagesPulse OximetryEmerson De SilvaNo ratings yet
- Benumof Anatomia Via AereaDocument11 pagesBenumof Anatomia Via AereaMaria RicardoNo ratings yet
- Brachycephalic Syndrome in DogsDocument7 pagesBrachycephalic Syndrome in DogsUmesh GopalanNo ratings yet
- Airway and Ventilatory ManagementDocument8 pagesAirway and Ventilatory ManagementAshen DissanayakaNo ratings yet
- Airway ManagementDocument5 pagesAirway ManagementPoova RagavanNo ratings yet
- Airway ManagementDocument38 pagesAirway ManagementyafetNo ratings yet
- Assisting in The Insertion of An Oral Airway and Endotracheal TubeDocument8 pagesAssisting in The Insertion of An Oral Airway and Endotracheal TubePatricia Feb De Los SantosNo ratings yet
- First Two Steps Are Discussed in This SectionDocument26 pagesFirst Two Steps Are Discussed in This SectionArchanaShenoyNo ratings yet
- Biology PPT 11Document11 pagesBiology PPT 11agarwalabhinav050No ratings yet
- The Science of SleepDocument3 pagesThe Science of SleepRuxandra MariaNo ratings yet
- Tracing-Copd For Respiratory AcidosisDocument4 pagesTracing-Copd For Respiratory Acidosisjoyrena ochondraNo ratings yet
- KAYLA H. LOPEZ OPST Template 2Document3 pagesKAYLA H. LOPEZ OPST Template 2Raynard MaestradoNo ratings yet
- Apheresis: (Principle & Clinical Applications)Document35 pagesApheresis: (Principle & Clinical Applications)aprinalNo ratings yet
- Burns NCPDocument8 pagesBurns NCPJM AsentistaNo ratings yet
- DapusDocument2 pagesDapusAmalia Sholihah MukhtarNo ratings yet
- Chapter 2 Science Form 4Document26 pagesChapter 2 Science Form 4Shafie Buyamin100% (2)
- (Pengkajian Pola Tidur) Psqi PDFDocument2 pages(Pengkajian Pola Tidur) Psqi PDFSri KuspartianingsihNo ratings yet
- NEET UG Biology Cockroach Comparative StudyDocument8 pagesNEET UG Biology Cockroach Comparative StudyYogesh MishraNo ratings yet
- Pengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten GianyarDocument9 pagesPengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten GianyaryanuarNo ratings yet
- 10 Quality Indicators For Blood Bank: Adverse Transfusion Reaction Rate %Document2 pages10 Quality Indicators For Blood Bank: Adverse Transfusion Reaction Rate %Toni StarkNo ratings yet
- Functions of The Human Respiratory System: What's inDocument4 pagesFunctions of The Human Respiratory System: What's injoyNo ratings yet
- Pediatric Sleep Disorders PDFDocument70 pagesPediatric Sleep Disorders PDFMalay P. Khamnuengkhuan100% (1)
- PowerPoint Presentation Resp and CircDocument7 pagesPowerPoint Presentation Resp and CircRobelle RelativoNo ratings yet
- Repiratory System: Presented by Group 3: Lacap, Lopez, Medina, MarceloDocument8 pagesRepiratory System: Presented by Group 3: Lacap, Lopez, Medina, MarceloAj LacapNo ratings yet
- 13 The Respiratory SystemDocument4 pages13 The Respiratory SystemPMG BrightNo ratings yet
- 4 Pics: 1 Word: Science 9Document9 pages4 Pics: 1 Word: Science 9Jan Matthew NuezNo ratings yet
- Biochem Experiment 3Document3 pagesBiochem Experiment 3Julius Memeg PanayoNo ratings yet
- History of Blood BankingDocument4 pagesHistory of Blood BankingShaira AlcantaraNo ratings yet