You might also like
- Urinary InfectionDocument33 pagesUrinary InfectionNithish SNo ratings yet
- Tuberculosos MeningititsDocument14 pagesTuberculosos MeningititsFerina UNo ratings yet
- Medications: Medication Name Generic/Trade Classification Pregnancy CategoryDocument8 pagesMedications: Medication Name Generic/Trade Classification Pregnancy CategoryapalestiNo ratings yet
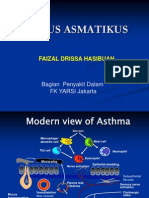
- Status Asmatikus FDH2012Document31 pagesStatus Asmatikus FDH2012Shabrina Ghassani Roza0% (1)
- Dengue: Subjective FindingsDocument5 pagesDengue: Subjective FindingsRaghu VenkatNo ratings yet
- SOAP NoteDocument26 pagesSOAP Noteapi-376765485% (13)
- EnuresisDocument26 pagesEnuresisAlexNo ratings yet
- Fabella NotesDocument96 pagesFabella NotesAndrassy Twinkle AlineaNo ratings yet
- Case PCAPDocument2 pagesCase PCAPNina Anne ParacadNo ratings yet
- Instruction: Stay Home / Stay Alert / Stay Safe / Control Virus / Win CovidDocument6 pagesInstruction: Stay Home / Stay Alert / Stay Safe / Control Virus / Win Covidrenugadevi_dNo ratings yet
- Final Exam Flash Cards - PDocument37 pagesFinal Exam Flash Cards - PReut shapiraNo ratings yet
- Case Presentation: BY 13QO320Document15 pagesCase Presentation: BY 13QO320Sandeep ChakravarthyNo ratings yet
- Morning Case Report: October 4th 2011Document22 pagesMorning Case Report: October 4th 2011Felicia adeline ChristianNo ratings yet
- Annexure - II Product DevelopmentDocument50 pagesAnnexure - II Product DevelopmentLife PearlNo ratings yet
- Receipts OSCE IM4Document4 pagesReceipts OSCE IM4Григорий КовалицкийNo ratings yet
- PneumoniaDocument12 pagesPneumoniaLia Pertiwi100% (1)
- Acute Exacerbation On Chronic Obstructive Pulmonary DisorderDocument30 pagesAcute Exacerbation On Chronic Obstructive Pulmonary DisorderFitri NurullahNo ratings yet
- Clinical Case Ent by Dr. NiazDocument37 pagesClinical Case Ent by Dr. NiazSiddiqur Rahman AkashNo ratings yet
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Document9 pagesO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNo ratings yet
- ASA Physical Status ClassificationDocument5 pagesASA Physical Status Classificationpolushky100% (1)
- Analgesics Content (AutoRecovered)Document11 pagesAnalgesics Content (AutoRecovered)ELISION OFFICIAL100% (1)
- Drug CardDocument2 pagesDrug CardHannahNo ratings yet
- Systemic Lupus Erythematosus: Anisa Zulfa F. Rachma Malina Tiara Dewi Salindri PratamaDocument48 pagesSystemic Lupus Erythematosus: Anisa Zulfa F. Rachma Malina Tiara Dewi Salindri PratamaasriNo ratings yet
- AleeshaDocument14 pagesAleeshaMayankNo ratings yet
- Department of Pharmacology: Clinical Case SheetsDocument34 pagesDepartment of Pharmacology: Clinical Case SheetsAyushmanNo ratings yet
- Central Neuraxial Blocks: Dr. Anilkumar T.K. Anaesthetist, NMC Hospital, Abudhabi, UAEDocument39 pagesCentral Neuraxial Blocks: Dr. Anilkumar T.K. Anaesthetist, NMC Hospital, Abudhabi, UAEansa1997No ratings yet
- Caz ClinicDocument15 pagesCaz ClinicAlina Maria DucaNo ratings yet
- Case Study TBDocument4 pagesCase Study TBRahmawatifNo ratings yet
- CASE PRESENTATION PneumoniaDocument13 pagesCASE PRESENTATION PneumoniaHari Singh RathoreNo ratings yet
- Lupus: Therapy T.Document10 pagesLupus: Therapy T.Sharifah ManuelNo ratings yet
- Acute Viral Syndrome: Case Presentation OnDocument22 pagesAcute Viral Syndrome: Case Presentation OnSafoora RafeeqNo ratings yet
- ConnectorDocument4 pagesConnectoryetaung8No ratings yet
- Pedi Pearls 2 - Scrubed PDFDocument46 pagesPedi Pearls 2 - Scrubed PDFthomasfx10100% (1)
- Drug Book On EmergencyDocument21 pagesDrug Book On EmergencyDimpal Choudhary100% (4)
- Alergi Case PresentationDocument17 pagesAlergi Case Presentationinne triaramafitaNo ratings yet
- Case - Parkinson's DiseaseDocument13 pagesCase - Parkinson's DiseaseAbin PNo ratings yet
- Analgesics ContentDocument11 pagesAnalgesics ContentELISION OFFICIALNo ratings yet
- Wa0010.Document14 pagesWa0010.TusharNo ratings yet
- DrugsDocument5 pagesDrugsdeepika kushwah100% (1)
- DrugsDocument5 pagesDrugsdeepika kushwahNo ratings yet
- FormularyDocument123 pagesFormularyMuhammad Shakeel100% (3)
- Care Plan: Patient' S BiodataDocument11 pagesCare Plan: Patient' S BiodataAnonymous xoEdtD91% (35)
- Elsharnoby Pediatric Made Easy Up Load Waheed Tantawy 2014Document160 pagesElsharnoby Pediatric Made Easy Up Load Waheed Tantawy 2014Emad AdelNo ratings yet
- 5 Emergency Drugs (Zacarias)Document7 pages5 Emergency Drugs (Zacarias)Joheina Cyndril L. ZacariasNo ratings yet
- Case On Diabetic Foot UlcerDocument24 pagesCase On Diabetic Foot Ulcerdimple alluriNo ratings yet
- Bulandos BSN3-1 Duty Drug StudyDocument5 pagesBulandos BSN3-1 Duty Drug StudyRolan BulandosNo ratings yet
- MR BP Dan AsphyxiaDocument29 pagesMR BP Dan AsphyxiaRizky FajriNo ratings yet
- Drug Dosage Calculation Handout For BSN CompletionDocument7 pagesDrug Dosage Calculation Handout For BSN CompletionchicktankNo ratings yet
- Brand NameDocument8 pagesBrand NameChristine Joy CamachoNo ratings yet
- EpilepsyDocument30 pagesEpilepsyabirami pNo ratings yet
- Dosis MimsDocument21 pagesDosis MimsYulia Putri CarlianaNo ratings yet
- Case Presentation 1Document16 pagesCase Presentation 112 E 36 Yatri PatelNo ratings yet
- Common Orofacial Pain Disorders - KN 3.24.18 IAEGDDocument99 pagesCommon Orofacial Pain Disorders - KN 3.24.18 IAEGDTayyuba AslamNo ratings yet
- Long PrescriptionsDocument27 pagesLong PrescriptionsSwaraj SKNo ratings yet
- Pediatric Status Epilepticus Pathway-FINALDocument5 pagesPediatric Status Epilepticus Pathway-FINALvural kesikNo ratings yet
- Morning Report Tension Type HeadacheDocument12 pagesMorning Report Tension Type HeadacheLintan FarzNo ratings yet
- Ortho 009 Orthopedic-InfectionsDocument20 pagesOrtho 009 Orthopedic-InfectionsJezreelyan VillanuevaNo ratings yet
- Liver AbscessDocument3 pagesLiver AbscessStephanie Pe100% (1)
- ADA en TBCDocument6 pagesADA en TBCNorma Ruth Aguilar CarbajalNo ratings yet
- Lymphangitis: Sclerosing of The PenisDocument4 pagesLymphangitis: Sclerosing of The PenisNick IlyéNo ratings yet
- BurnsDocument25 pagesBurnsJyotirmayeeNo ratings yet
- Ipo 21 1 043Document3 pagesIpo 21 1 043Y.rajuNo ratings yet
- PBL 1 Aspergillus - G1Document14 pagesPBL 1 Aspergillus - G1Rahmi Syarafina HakimNo ratings yet
- Culture MediaDocument3 pagesCulture MediaMicNo ratings yet
- A Review On: Salmonellosis and Its Economic and Public Health SignificanceDocument13 pagesA Review On: Salmonellosis and Its Economic and Public Health Significanceamanmalako50No ratings yet
- Binda BIO3219 Lab5Document12 pagesBinda BIO3219 Lab5Ronaldo BindaNo ratings yet
- Fdocuments - in General Microbiology Spotters by DR Sudheer Kher MD Hod MicrobiologyDocument32 pagesFdocuments - in General Microbiology Spotters by DR Sudheer Kher MD Hod MicrobiologyOppo VivoNo ratings yet
- Spotting PSMDocument60 pagesSpotting PSMAmanNo ratings yet
- New Case - Firza Humaira RespiDocument21 pagesNew Case - Firza Humaira RespiHardiyanti HermanNo ratings yet
- Lecture 18 - Introduction in Medical MicrobiologyDocument42 pagesLecture 18 - Introduction in Medical MicrobiologyAstri Ggamjong Xiao LuNo ratings yet
- Plant Viruses As Molecular PathogensDocument557 pagesPlant Viruses As Molecular PathogensDare SpartuNo ratings yet
- Fyne Elyka RebosuraSeptember 12Document11 pagesFyne Elyka RebosuraSeptember 12Fyne ElykaNo ratings yet
- Hygiene and Human HealthDocument69 pagesHygiene and Human HealthRalu OroszNo ratings yet
- MPSC Exams of OphthalmologyDocument7 pagesMPSC Exams of OphthalmologyHussein AliNo ratings yet
- N Hemanth ReddyDocument41 pagesN Hemanth Reddydiksha singhNo ratings yet
- PRAC 1 ID Biohazard v1Document8 pagesPRAC 1 ID Biohazard v1Amalia YusofNo ratings yet
- The Masque of The Red Death - READING and VOCABULARYDocument8 pagesThe Masque of The Red Death - READING and VOCABULARYDalglehys TorresNo ratings yet
- Designing and Constructing TeacherDocument8 pagesDesigning and Constructing TeacherKristel NaborNo ratings yet
- Lesson 3 Responses To Altered Ventilatory FunctionDocument136 pagesLesson 3 Responses To Altered Ventilatory FunctionMonasque PamelaNo ratings yet
- MalnutritionDocument43 pagesMalnutritionsharm1208100% (3)
- Microbiology MCQ QuestionsDocument4 pagesMicrobiology MCQ QuestionsNWH Adams LabNo ratings yet
- Nursing Care Plan: Histolytica, ADocument4 pagesNursing Care Plan: Histolytica, AkristennemarieNo ratings yet
- DLL-Q4W6-Compose Effective ParagraphsDocument6 pagesDLL-Q4W6-Compose Effective ParagraphsRiezel Joy M. SumauangNo ratings yet
- Health Facts 2020Document19 pagesHealth Facts 2020haikal11No ratings yet
- Reading - Age With Moderate DehydrationDocument8 pagesReading - Age With Moderate DehydrationSophia IbuyanNo ratings yet
- MicrobiologyDocument40 pagesMicrobiologyRasty Baku100% (1)