You might also like
- Instructor'S Background: Animal BehaviorDocument51 pagesInstructor'S Background: Animal BehaviorMala-Maria STAVRESCU-BEDIVANNo ratings yet
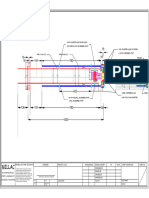
- Air System Air PipingDocument1 pageAir System Air PipingCalon KayaNo ratings yet
- Four-To-Five-Year-Olds Six-To-Seven-Year-Olds: Inefficient ModelDocument1 pageFour-To-Five-Year-Olds Six-To-Seven-Year-Olds: Inefficient ModelPedro AznicarNo ratings yet
- Čivije I KlinoviDocument6 pagesČivije I KlinoviGoran PantovicNo ratings yet
- The Origin and Scope of Behavioral Financial Economics January 18, 2017Document21 pagesThe Origin and Scope of Behavioral Financial Economics January 18, 2017econdocsNo ratings yet
- Index PERDocument21 pagesIndex PERMauricio BoteroNo ratings yet
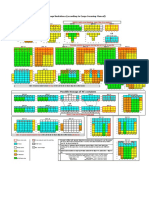
- Perkembangan Penyakit Yang Berpotensi KLB Menurut Minggu Upt Puskesmas Pasaleman Tahun 2018Document14 pagesPerkembangan Penyakit Yang Berpotensi KLB Menurut Minggu Upt Puskesmas Pasaleman Tahun 2018sudarNo ratings yet
- COVID-19 Virus Pandemic - WorldometerDocument12 pagesCOVID-19 Virus Pandemic - WorldometerAshutosh AwasthiNo ratings yet
- Econ 138: Financial and Behavioral Economics: Midterm 1: Review February 22, 2017Document47 pagesEcon 138: Financial and Behavioral Economics: Midterm 1: Review February 22, 2017econdocsNo ratings yet
- Coronavirus Cases:: View by CountryDocument19 pagesCoronavirus Cases:: View by CountryjayNo ratings yet
- Inductive Proximity Sensors: References: Pages 1/121 To 1/124 Characteristics: Pages 1/121 To 1/124Document6 pagesInductive Proximity Sensors: References: Pages 1/121 To 1/124 Characteristics: Pages 1/121 To 1/124andleralfonso7308No ratings yet
- International Health RegulationsDocument22 pagesInternational Health RegulationsYudi Jaya CahyanaNo ratings yet
- Red Dot 50yd Mod1 PDFDocument1 pageRed Dot 50yd Mod1 PDFRAYOSNo ratings yet
- ElectroswitchDocument2 pagesElectroswitchParasPatel80No ratings yet
- China Weekly Report: Aluminum Industry ChainDocument17 pagesChina Weekly Report: Aluminum Industry Chainnerolf73No ratings yet
- Seismic Design of ConcreteDocument14 pagesSeismic Design of ConcreteFunda YenersuNo ratings yet
- WD Qdos enDocument4 pagesWD Qdos enquanghuyvtNo ratings yet
- Coolant Flow Vs External RestrictionDocument2 pagesCoolant Flow Vs External RestrictionJhon Hever Benitez HernandezNo ratings yet
- Laundry AssignmentDocument5 pagesLaundry AssignmentNitish YadavNo ratings yet
- γ-Oryzanol: An Attractive Bioactive Component from Rice BranDocument22 pagesγ-Oryzanol: An Attractive Bioactive Component from Rice BranMuhammad Usman AkramNo ratings yet
- C:/DATA HPLC/PESTICIDAS/Data/07-10-2019 R4 L3.dat, DAD-CH1 220 NM C:/DATA HPLC/PESTICIDAS/Data/07-10-2019 R4 L2.dat, DAD-CH1 220 NMDocument1 pageC:/DATA HPLC/PESTICIDAS/Data/07-10-2019 R4 L3.dat, DAD-CH1 220 NM C:/DATA HPLC/PESTICIDAS/Data/07-10-2019 R4 L2.dat, DAD-CH1 220 NMadolfo olmosNo ratings yet
- Graftieaux, Michard, Grosjean - Combining PIV, POD and Vortex Identification Algorithms For The Study of Unsteady Turbulent Swirling FlowsDocument9 pagesGraftieaux, Michard, Grosjean - Combining PIV, POD and Vortex Identification Algorithms For The Study of Unsteady Turbulent Swirling FlowsAdrián NatalNo ratings yet
- Gizzard Proventriculus Health Marker Avinews Int Sept 22Document11 pagesGizzard Proventriculus Health Marker Avinews Int Sept 22mohamed helmyNo ratings yet
- WILO Yonos PARA RKA, RS 25-6Document2 pagesWILO Yonos PARA RKA, RS 25-6Mirela Paul100% (1)
- ANGKADocument1 pageANGKAira feraNo ratings yet
- Student Assessment Score GraphsDocument2 pagesStudent Assessment Score Graphsapi-431967040No ratings yet
- United States: Coronavirus CasesDocument11 pagesUnited States: Coronavirus Caseshervé louisNo ratings yet
- PIIS000709122030893XDocument3 pagesPIIS000709122030893XLarissaCarvalhoNo ratings yet
- Dutch Cone Penetration TestDocument5 pagesDutch Cone Penetration TestKobelNo ratings yet
- Hyosung Manual de Taller GT650-S-RDocument122 pagesHyosung Manual de Taller GT650-S-RLandrich Trosky100% (1)
- Column DetailDocument1 pageColumn DetaillakhanNo ratings yet
- PC 695SR 18 EUDocument32 pagesPC 695SR 18 EUДима ТукачNo ratings yet
- PC200LC-8 S - N A90301-Up - K0930-01a0 Cab Travel PPC Valve Body (1 - 2) PDFDocument1 pagePC200LC-8 S - N A90301-Up - K0930-01a0 Cab Travel PPC Valve Body (1 - 2) PDFEider Arturo Garcia OsorioNo ratings yet
- Parts Manual (EN) : Read The Operators Manual Before Using The MachineDocument22 pagesParts Manual (EN) : Read The Operators Manual Before Using The MachineVüsal 1No ratings yet
- Camera Housing - Revision 4-Layout3Document1 pageCamera Housing - Revision 4-Layout3Aldrin GallardoNo ratings yet
- Tab ArchitectsDocument13 pagesTab ArchitectsJorgeMariscalNo ratings yet
- FP Choker enDocument1 pageFP Choker envpn1 vpn1No ratings yet
- Sprinkler Items (TPMC)Document21 pagesSprinkler Items (TPMC)duleesha oshanNo ratings yet
- Wright 1996Document7 pagesWright 1996susiloNo ratings yet
- MDFI RDOHandgunZeroTarget 25ydDocument1 pageMDFI RDOHandgunZeroTarget 25ydJorge DutraNo ratings yet
- Red Dot 50ydDocument1 pageRed Dot 50ydbeetho1990No ratings yet
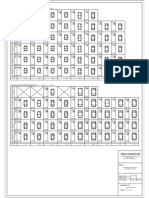
- Denah L1.L2Document1 pageDenah L1.L2Soibada NatarboraNo ratings yet
- Essential Biology Unit 18Document4 pagesEssential Biology Unit 18Poornima AthikariNo ratings yet
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Document7 pagesWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Sekar Inggar R0% (1)
- Kurva BB Anak Perempuan Menurut UsiaTBDocument7 pagesKurva BB Anak Perempuan Menurut UsiaTBAnindya YolandhaNo ratings yet
- Girl 2 - 5 Tahun - WHODocument3 pagesGirl 2 - 5 Tahun - WHOPatime Nekomata NibinoNo ratings yet
- Harus Diperhatikan Utk PoliDocument5 pagesHarus Diperhatikan Utk PoliBiyta BatubaraNo ratings yet
- WXseries Manual 2021 CompressionDocument187 pagesWXseries Manual 2021 CompressionAlexandre RodriguesNo ratings yet
- Normal Probability DistributionsDocument72 pagesNormal Probability Distributionsyeshwanth sunnapuNo ratings yet
- ISO ORTHO ModelDocument1 pageISO ORTHO Modelavishal ramNo ratings yet
- Case Study - Gearbox FailureDocument16 pagesCase Study - Gearbox FailureRateesh VenugopalanNo ratings yet
- Case Study - Gearbox FailureDocument16 pagesCase Study - Gearbox FailureRateesh VenugopalanNo ratings yet
- Proceq GPR Live - Grid Paper - 4inDocument1 pageProceq GPR Live - Grid Paper - 4inmohammad loai sabbaghNo ratings yet
- The Islamia University of Bahawalpur 9020899-0 The Islamia University of Bahawalpur 9020899-0 The Islamia University of Bahawalpur 9020899-0 The Islamia University of Bahawalpur 9020899-0Document1 pageThe Islamia University of Bahawalpur 9020899-0 The Islamia University of Bahawalpur 9020899-0 The Islamia University of Bahawalpur 9020899-0 The Islamia University of Bahawalpur 9020899-0Fahad RazzaqNo ratings yet
- Performance Lawn EquipmentDocument7 pagesPerformance Lawn EquipmentnurainNo ratings yet
- MV Coneste Stowage Limitations & ReefersDocument2 pagesMV Coneste Stowage Limitations & ReefersSergiyNo ratings yet
- Floor 4 - Teaching Studios + ToiletsDocument1 pageFloor 4 - Teaching Studios + Toiletsdulshan costaNo ratings yet
- Floor 4 - Teaching Studios + ToiletsDocument1 pageFloor 4 - Teaching Studios + Toiletsdulshan costaNo ratings yet
- EPAS 11 - Q1 - W1 - Mod1Document45 pagesEPAS 11 - Q1 - W1 - Mod1Alberto A. FugenNo ratings yet
- DLP - Light Science 7Document6 pagesDLP - Light Science 7Samara M. SalacayanNo ratings yet
- Aleutia Solar Container ClassroomDocument67 pagesAleutia Solar Container ClassroomaleutiaNo ratings yet
- Microsmart GEODTU Eng 7Document335 pagesMicrosmart GEODTU Eng 7Jim JonesjrNo ratings yet
- Eggermont 2019 ABRDocument15 pagesEggermont 2019 ABRSujeet PathakNo ratings yet
- Sept Dec 2018 Darjeeling CoDocument6 pagesSept Dec 2018 Darjeeling Conajihah zakariaNo ratings yet
- PC Model Answer Paper Winter 2016Document27 pagesPC Model Answer Paper Winter 2016Deepak VermaNo ratings yet
- 2022 Mable Parker Mclean Scholarship ApplicationDocument2 pages2022 Mable Parker Mclean Scholarship Applicationapi-444959661No ratings yet
- Technology Based Project: Special Track 1)Document14 pagesTechnology Based Project: Special Track 1)Kim ChiquilloNo ratings yet
- Teaching Profession - Educational PhilosophyDocument23 pagesTeaching Profession - Educational PhilosophyRon louise PereyraNo ratings yet
- Science 4 Diagnostic/Achievement TestDocument5 pagesScience 4 Diagnostic/Achievement TestGe PebresNo ratings yet
- MMS - IMCOST (RANJAN) Managing Early Growth of Business and New Venture ExpansionDocument13 pagesMMS - IMCOST (RANJAN) Managing Early Growth of Business and New Venture ExpansionDhananjay Parshuram SawantNo ratings yet
- QuexBook TutorialDocument14 pagesQuexBook TutorialJeffrey FarillasNo ratings yet
- Literatura Tecnica 3Document10 pagesLiteratura Tecnica 3Christian PerezNo ratings yet
- Phytotherapy On CancerDocument21 pagesPhytotherapy On CancerSiddhendu Bhattacharjee100% (1)
- Nanolithography - Processing Methods PDFDocument10 pagesNanolithography - Processing Methods PDFNilesh BhardwajNo ratings yet
- Application Form InnofundDocument13 pagesApplication Form InnofundharavinthanNo ratings yet
- Pg2022 ResultDocument86 pagesPg2022 ResultkapilNo ratings yet
- Advanced Chemical Engineering Thermodynamics (Cheg6121) : Review of Basic ThermodynamicsDocument74 pagesAdvanced Chemical Engineering Thermodynamics (Cheg6121) : Review of Basic ThermodynamicsetayhailuNo ratings yet
- W25509 PDF EngDocument11 pagesW25509 PDF EngNidhi SinghNo ratings yet
- Sources of Hindu LawDocument9 pagesSources of Hindu LawKrishnaKousikiNo ratings yet
- SOL LogicDocument21 pagesSOL LogicJa RiveraNo ratings yet
- Desktop 9 QA Prep Guide PDFDocument15 pagesDesktop 9 QA Prep Guide PDFPikine LebelgeNo ratings yet
- Comparison Between CompetitorsDocument2 pagesComparison Between Competitorsritesh singhNo ratings yet
- Core ValuesDocument1 pageCore ValuesIan Abel AntiverosNo ratings yet
- Recitation Math 001 - Term 221 (26166)Document36 pagesRecitation Math 001 - Term 221 (26166)Ma NaNo ratings yet
- 1 - 2020-CAP Surveys CatalogDocument356 pages1 - 2020-CAP Surveys CatalogCristiane AokiNo ratings yet
- Progressive Muscle RelaxationDocument4 pagesProgressive Muscle RelaxationEstéphany Rodrigues ZanonatoNo ratings yet
- Epson Stylus Pro 7900/9900: Printer GuideDocument208 pagesEpson Stylus Pro 7900/9900: Printer GuideJamesNo ratings yet
- Food ResourcesDocument20 pagesFood ResourceshiranNo ratings yet