You might also like
- 1.2 Nucleic Acid MetabolismDocument9 pages1.2 Nucleic Acid MetabolismHarshya RajeevanNo ratings yet
- Office of The Child Advocate Harmony Montgomery Investigative Report - May 2022Document101 pagesOffice of The Child Advocate Harmony Montgomery Investigative Report - May 2022Christopher Gavin100% (1)
- How To Start A Niche Staffing or Recruiting Business - Discover Your NicheDocument30 pagesHow To Start A Niche Staffing or Recruiting Business - Discover Your NicheDee Williams67% (3)
- Twin Hearts MeditationDocument1 pageTwin Hearts MeditationVarshaSutrave100% (3)
- Micro Microbial Mechanisms of Pathogenicity NOTESDocument6 pagesMicro Microbial Mechanisms of Pathogenicity NOTESAriane NobleNo ratings yet
- Renal Function and The Significance of Non-Protein Nitrogen CompoundsDocument12 pagesRenal Function and The Significance of Non-Protein Nitrogen CompoundsSrujana BudheNo ratings yet
- Microbiology 1.1 Immunology - Dr. FontanillaDocument115 pagesMicrobiology 1.1 Immunology - Dr. FontanillaRyn ShadowNo ratings yet
- chapter-4-ACELLULAR AND PROKARYOTIK MICROBESDocument66 pageschapter-4-ACELLULAR AND PROKARYOTIK MICROBESCza Mae ArsenalNo ratings yet
- Natural Product As AntiviralDocument30 pagesNatural Product As AntiviralMayuriNo ratings yet
- B.SC - Aquaculture Technology 2020-21 (New Course)Document26 pagesB.SC - Aquaculture Technology 2020-21 (New Course)yaswanth kumarNo ratings yet
- Gene Expression and Regulation - Mutation PDFDocument57 pagesGene Expression and Regulation - Mutation PDFEsther MathengeNo ratings yet
- Biological Ions and Oxid PhospDocument67 pagesBiological Ions and Oxid PhospRamesh KetaNo ratings yet
- Compre MolbioDocument93 pagesCompre MolbioDeniebev'z OrillosNo ratings yet
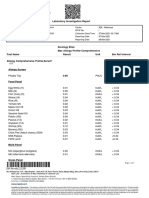
- Laboratory Investigation ReportDocument7 pagesLaboratory Investigation ReportAmarjeetNo ratings yet
- BIO 310 Midterm 2 + Final Exam PackageDocument44 pagesBIO 310 Midterm 2 + Final Exam PackageNerdy Notes Inc.No ratings yet
- 2023 02 01EatingWellAntioxidantsDocument100 pages2023 02 01EatingWellAntioxidantsCRISTINA ENENo ratings yet
- Genetic Engineering ToolsDocument73 pagesGenetic Engineering Toolsmulatu mokononNo ratings yet
- Synapse & NeurotransmissionDocument21 pagesSynapse & Neurotransmissionزين العابدين محمد عويشNo ratings yet
- MLS 422 Diagnostic MicrobiologyDocument50 pagesMLS 422 Diagnostic MicrobiologyMayowa OgunmolaNo ratings yet
- RBC MembraneDocument4 pagesRBC MembraneJustine Claire M. NamocatcatNo ratings yet
- Adaptive Spatial Image Steganography and Steganalysis Using Perceptual Modelling and Machine LearningDocument189 pagesAdaptive Spatial Image Steganography and Steganalysis Using Perceptual Modelling and Machine LearningDemaZiad100% (1)
- Molecular Biology of Viroid-Host Interactions and Disease Control StrategiesDocument13 pagesMolecular Biology of Viroid-Host Interactions and Disease Control StrategiesKhoo Ying WeiNo ratings yet
- Hematology ReviewerDocument12 pagesHematology ReviewerPatty RomeroNo ratings yet
- Cell Division-MergedDocument13 pagesCell Division-MergedJewel Gwen D. BACALINGNo ratings yet
- Monoclonal Antibody - HHMDocument44 pagesMonoclonal Antibody - HHMIsrat Jahan Surovy 2225400672No ratings yet
- EUCAST E Def 9.3.2 Mould Testing Definitive Revised 2020Document23 pagesEUCAST E Def 9.3.2 Mould Testing Definitive Revised 2020Guneyden GuneydenNo ratings yet
- 0 BooksDocument27 pages0 BooksSeyha L. AgriFoodNo ratings yet
- Fixation ImpregnationDocument18 pagesFixation ImpregnationKarla Mae Tolelis - BurlatNo ratings yet
- Cointegrated VectorsDocument2 pagesCointegrated Vectorsdevikamurugan124206No ratings yet
- 2017 Vaccines in Development Product List FinalDocument39 pages2017 Vaccines in Development Product List FinalukilabosNo ratings yet
- Science Form 2-28-51Document24 pagesScience Form 2-28-51Gan Wei ShengNo ratings yet
- BasidiomycotaDocument63 pagesBasidiomycotamohanapriya.raNo ratings yet
- Yellow Blue Colorful Illustrated Education Presentation 169Document14 pagesYellow Blue Colorful Illustrated Education Presentation 169Mike Clinton BilogNo ratings yet
- CHPT 12 Intracellular Compartments Anddfd Protein SortingDocument59 pagesCHPT 12 Intracellular Compartments Anddfd Protein SortingSaurabh SrivastavaNo ratings yet
- Fish Disease BookDocument112 pagesFish Disease BookMemo KenaweeNo ratings yet
- Bacterial MetabolismDocument43 pagesBacterial MetabolismAlmoatazbellah AbdallahNo ratings yet
- Antibody EngineeringDocument14 pagesAntibody EngineeringJholina Aure ReyesNo ratings yet
- From DNA Biosensor To Gene ChipDocument6 pagesFrom DNA Biosensor To Gene ChipramzermanNo ratings yet
- Classification Animal Kingdom English 77Document8 pagesClassification Animal Kingdom English 77Aayush MalikNo ratings yet
- Class 11 Biology Chapter 8 - Revision NotesDocument10 pagesClass 11 Biology Chapter 8 - Revision NotesHARKIRIT KAUR100% (1)
- Directed Mutagenesis and Protein EngineeringDocument52 pagesDirected Mutagenesis and Protein Engineeringslowdragon2003No ratings yet
- Properties of LightDocument43 pagesProperties of LightKaezeth Jasmine AñanaNo ratings yet
- Lecture 1. Life Biological Principles and The Science of ZoologyDocument64 pagesLecture 1. Life Biological Principles and The Science of ZoologyLeopoldo ConstantinoNo ratings yet
- Biology Lab Report 2Document6 pagesBiology Lab Report 2Quynh Dang PhuongNo ratings yet
- Parasitology SAQs With AnswersDocument14 pagesParasitology SAQs With AnswersGeorge Makori100% (1)
- R DNA TechnologyDocument17 pagesR DNA TechnologyDRMEHUL DAVENo ratings yet
- IonomicsDocument48 pagesIonomicssowmyaNo ratings yet
- Beneficial Effects of The Normal FloraDocument4 pagesBeneficial Effects of The Normal FloraSyazmin KhairuddinNo ratings yet
- Marine ToxinsDocument53 pagesMarine ToxinsYrika VillasenorNo ratings yet
- cDNA Library - WikipediaDocument4 pagescDNA Library - WikipediaHkr GamingNo ratings yet
- Screening and Quantitative Determination of Drugs of Abuse in DilutedDocument13 pagesScreening and Quantitative Determination of Drugs of Abuse in DilutedleliNo ratings yet
- DBT BET JRF 2018 Solved Question Paper With Answer KeyDocument51 pagesDBT BET JRF 2018 Solved Question Paper With Answer KeyRana GhoshNo ratings yet
- Construction of Genomic LibraryDocument16 pagesConstruction of Genomic Librarysivagurunathan.P80% (5)
- Fermentation Biotech PresentationDocument19 pagesFermentation Biotech Presentationtawedzerwa masundaNo ratings yet
- STK 1233 Organic Chemistry 1: LU 5.1: Aromatic CompoundsDocument37 pagesSTK 1233 Organic Chemistry 1: LU 5.1: Aromatic CompoundsArllen Joy AlbertNo ratings yet
- CHAPTER 4 Lesson 1 VirusDocument29 pagesCHAPTER 4 Lesson 1 VirusKreizel FajaNo ratings yet
- Bacteriology HandoutDocument30 pagesBacteriology HandoutMoonyeen Jann Casera BalicNo ratings yet
- Rna InterferenceDocument10 pagesRna InterferencewaktoleNo ratings yet
- Betelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesDocument37 pagesBetelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesMuh AqwilNo ratings yet
- Tele Nos.Document56 pagesTele Nos.wgeradNo ratings yet
- MCQ of Neurochemistry and Signal Transduction-2022-FinalDocument6 pagesMCQ of Neurochemistry and Signal Transduction-2022-FinalKaif AliNo ratings yet
- Cell Biology FinalsDocument12 pagesCell Biology FinalsNellyNo ratings yet
- 202211121648018939miclolab 300Document4 pages202211121648018939miclolab 300Ajish joNo ratings yet
- Aa321020002514b RC08102020Document3 pagesAa321020002514b RC08102020Ajish joNo ratings yet
- InitiateSingleEntryPaymentSummary14 03 2022Document1 pageInitiateSingleEntryPaymentSummary14 03 2022Ajish joNo ratings yet
- InitiateSingleEntryPaymentSummary04 03 2023Document1 pageInitiateSingleEntryPaymentSummary04 03 2023Ajish joNo ratings yet
- InitiateSingleEntryPaymentSummary15 12 2022Document1 pageInitiateSingleEntryPaymentSummary15 12 2022Ajish joNo ratings yet
- Kcea 22Document4 pagesKcea 22Ajish joNo ratings yet
- Evennett Oct2008 01 Principles-Of-MicrosDocument96 pagesEvennett Oct2008 01 Principles-Of-MicrosAjish joNo ratings yet
- Bilirubin Total - Tab: 5 X 100/5 X 11 ML 12011006Document1 pageBilirubin Total - Tab: 5 X 100/5 X 11 ML 12011006Ajish joNo ratings yet
- SN 74 Ls 374Document32 pagesSN 74 Ls 374Ajish joNo ratings yet
- 63c7d630a250d IQ2223 283180 PDFDocument1 page63c7d630a250d IQ2223 283180 PDFAjish joNo ratings yet
- ST 200CLDocument2 pagesST 200CLAjish joNo ratings yet
- InitiateSingleEntryPaymentSummary06 02 2023Document1 pageInitiateSingleEntryPaymentSummary06 02 2023Ajish joNo ratings yet
- Bilirubin Direct: 5 X 100/5 X 11 ML 12011005Document1 pageBilirubin Direct: 5 X 100/5 X 11 ML 12011005Ajish joNo ratings yet
- Borishura 300 G300 GTDocument2 pagesBorishura 300 G300 GTAjish joNo ratings yet
- 1019579386-H 560 4 Page Brochure (05-2019)Document2 pages1019579386-H 560 4 Page Brochure (05-2019)Ajish joNo ratings yet
- Ureauv: 5 X 100/5 X 29 ML 12011025Document1 pageUreauv: 5 X 100/5 X 29 ML 12011025Ajish joNo ratings yet
- AutoLab AccordDocument2 pagesAutoLab AccordAjish joNo ratings yet
- InitiateSingleEntryPaymentSummary05 01 2023Document1 pageInitiateSingleEntryPaymentSummary05 01 2023Ajish joNo ratings yet
- InitiateSingleEntryPaymentSummary09 12 2022Document1 pageInitiateSingleEntryPaymentSummary09 12 2022Ajish joNo ratings yet
- G.O (RT) 386 2022Document2 pagesG.O (RT) 386 2022Ajish joNo ratings yet
- Human AnatomyDocument37 pagesHuman AnatomyAjish joNo ratings yet
- Erba EC90 Print AW 430 LIT-30-001 2022 1Document4 pagesErba EC90 Print AW 430 LIT-30-001 2022 1Ajish joNo ratings yet
- Nulyte Smart Electrolyte AnalyzerDocument2 pagesNulyte Smart Electrolyte AnalyzerAjish joNo ratings yet
- Quote in The RDFHJKDocument5 pagesQuote in The RDFHJKAjish joNo ratings yet
- Protable Ultra Sound AlokaDocument4 pagesProtable Ultra Sound AlokaAjish joNo ratings yet
- Cal and QC Storage (68 Items)Document26 pagesCal and QC Storage (68 Items)Ajish joNo ratings yet
- Lab Settings Malabar Dental College New 04.03.2022Document4 pagesLab Settings Malabar Dental College New 04.03.2022Ajish joNo ratings yet
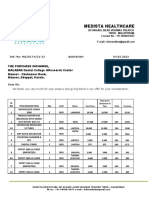
- Redcell Biomedicals: Room No:64/1378-D6, Leela Arcade, Sasthrinagar Colony East Nadakkavu, Eranjipalam Po, Calicut-673006Document4 pagesRedcell Biomedicals: Room No:64/1378-D6, Leela Arcade, Sasthrinagar Colony East Nadakkavu, Eranjipalam Po, Calicut-673006Ajish joNo ratings yet
- Touch Screen TechnologyDocument9 pagesTouch Screen TechnologyAjish joNo ratings yet
- Quality of Service Agreement For IserviceDocument3 pagesQuality of Service Agreement For IserviceAjish joNo ratings yet
- Amiodarone Guideline For Use and MonitoringDocument8 pagesAmiodarone Guideline For Use and MonitoringTania NicolaescuNo ratings yet
- Anorectal Malformations: DR BenakDocument22 pagesAnorectal Malformations: DR Benakbenak shivalingappaNo ratings yet
- Ma 4001 Lyo 5 DcuiDocument2 pagesMa 4001 Lyo 5 DcuirestandcleanaguachicaNo ratings yet
- CHED Regional Memorandum No. 3, S. 2021Document6 pagesCHED Regional Memorandum No. 3, S. 2021Amy uretaNo ratings yet
- Flottec PAX CollectorDocument8 pagesFlottec PAX Collectorrodolfom664No ratings yet
- 80D CertificateDocument2 pages80D Certificateuppada.89No ratings yet
- 2021 Covid19 Report - Swabhiman, BhubaneswarDocument36 pages2021 Covid19 Report - Swabhiman, BhubaneswarDr Sruti MohapatraNo ratings yet
- NP5 Sample QuestionsDocument7 pagesNP5 Sample QuestionsIvan LouiseNo ratings yet
- Film Review The Sugar FilmDocument1 pageFilm Review The Sugar FilmRhyl Jife Paglumotan MaantosNo ratings yet
- Centurion Lead Acid Battery, Wet, Non Spillable Sds 01898 03042018Document7 pagesCenturion Lead Acid Battery, Wet, Non Spillable Sds 01898 03042018Munya BengezaNo ratings yet
- Indications and Use of Therapeutic Phlebotomy in Polycythemia Vera - Which Role For ErythrocytapheresisDocument3 pagesIndications and Use of Therapeutic Phlebotomy in Polycythemia Vera - Which Role For ErythrocytapheresisYuendri IrawantoNo ratings yet
- Mayor's Speech: Valuing DiversityDocument20 pagesMayor's Speech: Valuing Diversityian rex desolocNo ratings yet
- Frank Straub ResumeDocument6 pagesFrank Straub ResumeInlanderChrisNo ratings yet
- MethergineDocument2 pagesMethergineKureaa Oh100% (1)
- Nihms 991190Document14 pagesNihms 991190Samuel Idrogo AlfaroNo ratings yet
- Occupational Health in Indonesia: Astrid Sulistomo Dep. of Community Medicine FmuiDocument99 pagesOccupational Health in Indonesia: Astrid Sulistomo Dep. of Community Medicine FmuiDea MaharaniNo ratings yet
- Gross Anatomy PDFDocument55 pagesGross Anatomy PDFDeborah RochaNo ratings yet
- Aster Cmi - BrochureDocument4 pagesAster Cmi - BrochureholysaatanNo ratings yet
- Political DoctrinesDocument7 pagesPolitical DoctrinesJohn Allauigan MarayagNo ratings yet
- Cowpea Isoflavones and PCOSDocument6 pagesCowpea Isoflavones and PCOSAamer SyedNo ratings yet
- St. Mary's Stories That Span The AgesDocument2 pagesSt. Mary's Stories That Span The AgesLATIMDNo ratings yet
- A Longitudinal Fissure Separates The Human Brain Into Two Distinct Cerebral HemisphereDocument3 pagesA Longitudinal Fissure Separates The Human Brain Into Two Distinct Cerebral Hemisphereamandashn96No ratings yet
- Basic Ethical Concepts To Ethical Principles: C. Personalized SexualityDocument14 pagesBasic Ethical Concepts To Ethical Principles: C. Personalized SexualitySophia BonifacioNo ratings yet
- Philippine Health Information System: Crispinita A. Valdez Director, Information Management ServiceDocument22 pagesPhilippine Health Information System: Crispinita A. Valdez Director, Information Management ServiceJuly AlliveNo ratings yet
- FolicartDocument12 pagesFolicartDiana-Elena ComandasuNo ratings yet
- IPC Self AssessmentDocument9 pagesIPC Self AssessmentquesterNo ratings yet
- Pharma For StudentsDocument23 pagesPharma For StudentsDominic Reambonanza0% (1)