You might also like
- Anti-Asthmatics: Dr. Sadia Shahid PGT-Pharmacology IimcDocument30 pagesAnti-Asthmatics: Dr. Sadia Shahid PGT-Pharmacology IimcWafaa AbdullahNo ratings yet
- Modul Muskuloskeletal - NSAIDs 2017Document56 pagesModul Muskuloskeletal - NSAIDs 2017khairunnisanurainiNo ratings yet
- RespiratoryDocument2 pagesRespiratoryJohn SmithNo ratings yet
- Bronchial Asthama and COPDDocument37 pagesBronchial Asthama and COPDAyesha AlamNo ratings yet
- Generic Name: Mechanism of Action: Side Effects/ Adverse Effects: Nursing Responsibilities: Brand NameDocument3 pagesGeneric Name: Mechanism of Action: Side Effects/ Adverse Effects: Nursing Responsibilities: Brand NameMacarayo AldemaeNo ratings yet
- Anti Fungal: Dr. Dr. Nico L Lumbuun, SPFKDocument45 pagesAnti Fungal: Dr. Dr. Nico L Lumbuun, SPFKAudhrey BNo ratings yet
- Respiratory PharmacologyDocument34 pagesRespiratory PharmacologyHirpâsà MămoNo ratings yet
- FTX Infeksi JamurDocument64 pagesFTX Infeksi JamurNafisah SofiaNo ratings yet
- Antiasthmatic DrugsDocument36 pagesAntiasthmatic DrugsJannah ZahraaNo ratings yet
- DexamethasoneDocument3 pagesDexamethasoneGwyn RosalesNo ratings yet
- Albuterol Nursing Care for Bronchospasm ReliefDocument3 pagesAlbuterol Nursing Care for Bronchospasm ReliefGino B. BulanaNo ratings yet
- Class Medication MOA Side Effects: Intranasal SteroidsDocument2 pagesClass Medication MOA Side Effects: Intranasal SteroidsChron MedNo ratings yet
- E Kart DrugsDocument3 pagesE Kart DrugsNichole CastleNo ratings yet
- Bronchial Asthma: Dr. Tiko GognadzeDocument36 pagesBronchial Asthma: Dr. Tiko GognadzeibrahimNo ratings yet
- Respiratory System 60, 61Document2 pagesRespiratory System 60, 61ahmedsalah565vvvNo ratings yet
- Pharmacotherapy of Asthma and Chronic Obstructive Pulmonary DiseaseDocument47 pagesPharmacotherapy of Asthma and Chronic Obstructive Pulmonary DiseaseAriel OlshevskyNo ratings yet
- Aplastic Anemia, Megaloblastic Anemia & ITP TreatmentsDocument21 pagesAplastic Anemia, Megaloblastic Anemia & ITP TreatmentsRea Dominique CabanillaNo ratings yet
- Drug Study LadyDocument8 pagesDrug Study LadyLadybelle GototosNo ratings yet
- Saba Hanif Presentation...Document19 pagesSaba Hanif Presentation...Saba KhanNo ratings yet
- Pharmacology of Nonsteroidal Anti-Inflammatory Drugs and GlucocorticoidsDocument56 pagesPharmacology of Nonsteroidal Anti-Inflammatory Drugs and GlucocorticoidsRidhaNo ratings yet
- AsthmaDocument8 pagesAsthmaAbdul WahidNo ratings yet
- Antifungaldrugs 150519204813 Lva1 App6892Document54 pagesAntifungaldrugs 150519204813 Lva1 App6892Jennifer S ZiegenNo ratings yet
- Covid19-Drug StudyDocument7 pagesCovid19-Drug StudynicoleNo ratings yet
- Antiinflammatory Drugs: Toya AriawanDocument27 pagesAntiinflammatory Drugs: Toya Ariawanlast100% (1)
- Id card of collegeDocument72 pagesId card of collegeJagruti YadavNo ratings yet
- NSAIDSDocument19 pagesNSAIDSDonna Kelly DuranNo ratings yet
- Asma Bronkial & Copd: Bagian Farmakologi Fakultas Kedokteran Universitas TadulakoDocument38 pagesAsma Bronkial & Copd: Bagian Farmakologi Fakultas Kedokteran Universitas TadulakoPutri PrimandiniNo ratings yet
- Drugs for Bronchial Asthma: B2 Agonists, Corticosteroids, PDE InhibitorsDocument15 pagesDrugs for Bronchial Asthma: B2 Agonists, Corticosteroids, PDE InhibitorsShahid Hameed100% (1)
- Drug 25Document17 pagesDrug 25carol_gigliotti24100% (1)
- Drug StudyDocument5 pagesDrug Studyboxed juiceNo ratings yet
- AsthmaDocument42 pagesAsthma7w2b96qznkNo ratings yet
- Respiratory System Pharmacology NotesDocument15 pagesRespiratory System Pharmacology NotesAli Rahimi100% (1)
- Methylprednisolone Drug Profile and Nursing ConsiderationsDocument4 pagesMethylprednisolone Drug Profile and Nursing ConsiderationsadryananestesiNo ratings yet
- Bp1 Sgd1: TopicsDocument7 pagesBp1 Sgd1: TopicsAlan Joseph BaldovinoNo ratings yet
- 4 AutacoidsDocument9 pages4 AutacoidsAli EllaffiNo ratings yet
- Notes - Lec 20 - Antimycobacterial AgentsDocument14 pagesNotes - Lec 20 - Antimycobacterial AgentsChesmar MacapalaNo ratings yet
- Pharmacology of Drugs Used in Bronchial Asthma & COPDDocument84 pagesPharmacology of Drugs Used in Bronchial Asthma & COPDdfngjlnNo ratings yet
- Lecture 7. Antifungal AgentsDocument30 pagesLecture 7. Antifungal AgentsyomifNo ratings yet
- Drugs in Treatment of Bronchial AsthmaDocument46 pagesDrugs in Treatment of Bronchial AsthmaNikita JangraNo ratings yet
- Antifungal Drugs 3Document54 pagesAntifungal Drugs 3Mikee MeladNo ratings yet
- 1.Antifungal Drug Derma Presentation .Done[1]Document38 pages1.Antifungal Drug Derma Presentation .Done[1]sahghanshyam9160No ratings yet
- Respiratory SystemDocument27 pagesRespiratory SystemSowndariyaNo ratings yet
- Asthma and RenalDocument9 pagesAsthma and RenalHlaSoe WinNo ratings yet
- Asma Felino TratamientoDocument7 pagesAsma Felino TratamientoRenzo Alessandro Pacherres NietoNo ratings yet
- Drug For Systemic Mycoses: Systemic Mycoses Can Be Subdivided Into Two CategoriesDocument39 pagesDrug For Systemic Mycoses: Systemic Mycoses Can Be Subdivided Into Two CategoriesCurex QANo ratings yet
- Top 200 Expanded 1Document27 pagesTop 200 Expanded 1Dean HarperNo ratings yet
- Paracetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Document1 pageParacetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Jesse James Advincula EdjecNo ratings yet
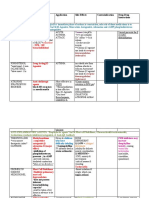
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNo ratings yet
- NSAIDsDocument12 pagesNSAIDsjelly100% (1)
- 3 Analgesic Anitpyretic InfamDocument10 pages3 Analgesic Anitpyretic InfamAnonymous dRAu54No ratings yet
- 2020 Drugs On Pain (Analgesics) - DENTISTRYDocument28 pages2020 Drugs On Pain (Analgesics) - DENTISTRYVisayan Alliah GailNo ratings yet
- Drug StudyDocument25 pagesDrug StudyRoland YusteNo ratings yet
- HNN215 Drug Diary GuideDocument10 pagesHNN215 Drug Diary GuideMaddison MitchellNo ratings yet
- Asthma MedicationDocument2 pagesAsthma MedicationAlexandra AlexaNo ratings yet
- 4.l - Respiratory System Pharmacology by IGMRIDocument13 pages4.l - Respiratory System Pharmacology by IGMRIclaw foreSK TeamNo ratings yet
- Bronchial AsthmaDocument43 pagesBronchial AsthmaAmar BimavarapuNo ratings yet
- Anti-Fungal Drugs Guide for Mycosis TreatmentDocument6 pagesAnti-Fungal Drugs Guide for Mycosis Treatmentbilal ahmadNo ratings yet
- Name of Drug Dosage/Route Mechanism of Action/ Classification Indication/Contraindication Side/Adverse Effects Nursing ConsiderationsDocument3 pagesName of Drug Dosage/Route Mechanism of Action/ Classification Indication/Contraindication Side/Adverse Effects Nursing ConsiderationsMonica Gagarin CortezNo ratings yet
- Group 1 RRLSDocument4 pagesGroup 1 RRLScyrusarckreibagoNo ratings yet
- Remedies in TortDocument4 pagesRemedies in TortAhmad Irtaza Adil100% (2)
- Kinsey Crimes and ConsequencesDocument370 pagesKinsey Crimes and ConsequencesMirela ZahNo ratings yet
- Corporate Finance I - Lecture 7bDocument20 pagesCorporate Finance I - Lecture 7bSandra BempongNo ratings yet
- AP10 - Q2 - Mod3 - Mga Dahilan at Epekto NG Migrasyon PDFDocument1 pageAP10 - Q2 - Mod3 - Mga Dahilan at Epekto NG Migrasyon PDFZyral Alliyah SantiagoNo ratings yet
- Liturgical Music For LentDocument11 pagesLiturgical Music For LentShirly Benedictos100% (1)
- (E6) Exercise For Unit 6Document2 pages(E6) Exercise For Unit 6Lê Cẩm YênNo ratings yet
- Meridian Analysis Energy DeviceDocument4 pagesMeridian Analysis Energy Devicehistory APNo ratings yet
- Signal Processing and Linear Systems I: Introduction To Fourier TransformsDocument18 pagesSignal Processing and Linear Systems I: Introduction To Fourier Transformsomar471No ratings yet
- Olweus Research HistoryDocument2 pagesOlweus Research Historykso87100% (1)
- 20 Common Defense Mechanisms for AnxietyDocument8 pages20 Common Defense Mechanisms for AnxietyAbhishek NegiNo ratings yet
- 2017 Normal EnglishDocument854 pages2017 Normal EnglishÂnuda M ĞalappaththiNo ratings yet
- Vinaytech - Power Bi - Demo - Conclusion - Important - TermsDocument19 pagesVinaytech - Power Bi - Demo - Conclusion - Important - TermsSsNo ratings yet
- Action PlanDocument3 pagesAction PlanMaki BalisiNo ratings yet
- Lira PDFDocument2 pagesLira PDFNairi Zadikian100% (1)
- The Examiner of Alternative MedicineDocument4 pagesThe Examiner of Alternative MedicineLee Ming HinNo ratings yet
- Financial Times Europe 14 November 2023Document18 pagesFinancial Times Europe 14 November 2023Nikola JovanovNo ratings yet
- PSMB Certified Trainer Curriculum StructureDocument19 pagesPSMB Certified Trainer Curriculum StructureFlankerSparrowNo ratings yet
- Petronas Approved Medical Examiner List 2017 (Latest Updated Version)Document4 pagesPetronas Approved Medical Examiner List 2017 (Latest Updated Version)Zulfadli RaniNo ratings yet
- Soal PAS 2019 Kelas X IPA-IPS FIXDocument8 pagesSoal PAS 2019 Kelas X IPA-IPS FIXJessica JolieNo ratings yet
- Ameama Zubair 70080433 Poem: Goe, and Catche A Falling Star: Poem: The Sunne RisingDocument2 pagesAmeama Zubair 70080433 Poem: Goe, and Catche A Falling Star: Poem: The Sunne RisingAsma KhanNo ratings yet
- C01 Globalisation: The Global Village?Document21 pagesC01 Globalisation: The Global Village?Mat RoyNo ratings yet
- Hindalco Industries Ltd000Document19 pagesHindalco Industries Ltd000Parshant Chohan100% (1)
- Unit 2.ieltsDocument11 pagesUnit 2.ieltsKarina HrishkovskaNo ratings yet
- The Art of Dying by Neville GoddardDocument4 pagesThe Art of Dying by Neville GoddardhabiotoNo ratings yet
- I) Complete With The Correct Form of The Given Verb: - /5Document3 pagesI) Complete With The Correct Form of The Given Verb: - /5Jasmina PedišićNo ratings yet
- Telecom Business Information System AbstractDocument5 pagesTelecom Business Information System AbstractTelika RamuNo ratings yet
- MSC Logic Self Study 2019 CompleteDocument88 pagesMSC Logic Self Study 2019 CompleteAlyssa RenataNo ratings yet
- The Etherington BrothersDocument30 pagesThe Etherington Brotherstoninho_6660% (1)
- Dokumen - Tips - Chapter 17 Job Order Costing Costing Chapter 17 Learning Objectives 1 DistinguishDocument25 pagesDokumen - Tips - Chapter 17 Job Order Costing Costing Chapter 17 Learning Objectives 1 DistinguishNouman SheikhNo ratings yet








































![1.Antifungal Drug Derma Presentation .Done[1]](https://imgv2-2-f.scribdassets.com/img/document/726540793/149x198/253071d297/1714042600?v=1)