You might also like
- Basal Cell Carcinoma: Advances in Treatment and ResearchFrom EverandBasal Cell Carcinoma: Advances in Treatment and ResearchMichael R. MigdenNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Senchenkov 2013Document8 pagesSenchenkov 2013cocooakNo ratings yet
- 1 Ijdrdjun20191Document4 pages1 Ijdrdjun20191TJPRC PublicationsNo ratings yet
- 56 Sonawane EtalDocument3 pages56 Sonawane EtaleditorijmrhsNo ratings yet
- ECP 2017 Asbtracts Supplement (12 Lucrari)Document14 pagesECP 2017 Asbtracts Supplement (12 Lucrari)Cristiana PoppNo ratings yet
- Myeloma MultipleDocument7 pagesMyeloma MultipleCriissthiiann HernnandezNo ratings yet
- Pediatric Surgery Update Volume 33, 2009Document12 pagesPediatric Surgery Update Volume 33, 2009rajarshikNo ratings yet
- Concurrent Basal Cell and Squamous Cell Carcinomas Associated With Hydroxyurea TherapyDocument4 pagesConcurrent Basal Cell and Squamous Cell Carcinomas Associated With Hydroxyurea Therapyanisse89No ratings yet
- Primary Ameloblastic Carcinoma of The Maxilla A CaDocument9 pagesPrimary Ameloblastic Carcinoma of The Maxilla A CaMuhammad Avicenna AdjiNo ratings yet
- Basal Cell Carcinoma in ChildhoodDocument2 pagesBasal Cell Carcinoma in ChildhoodAgustina D'AlessandroNo ratings yet
- Unusual Skin TumorsDocument12 pagesUnusual Skin TumorsGleny SumNo ratings yet
- Recurrence of Mycosis Fungoides On Multiple Melanocytic Nevi: A Case Report and Review of The LiteratureDocument6 pagesRecurrence of Mycosis Fungoides On Multiple Melanocytic Nevi: A Case Report and Review of The LiteraturenanonanditoNo ratings yet
- 2018 Article 1941Document6 pages2018 Article 1941Chairul LatiefNo ratings yet
- MTT LabialDocument3 pagesMTT LabialRobertoNo ratings yet
- Squamous Cell Carcinoma of The Skin EpidemiologyDocument11 pagesSquamous Cell Carcinoma of The Skin EpidemiologyNeni NengsiNo ratings yet
- Issn 2 Issn 2 Issn 2 ISSN 2073 073 073 073 - 9990 East Cent. Afr. J. S 9990 East Cent. Afr. J. S 9990 East Cent. Afr. J. S 9990 East Cent. Afr. J. SDocument7 pagesIssn 2 Issn 2 Issn 2 ISSN 2073 073 073 073 - 9990 East Cent. Afr. J. S 9990 East Cent. Afr. J. S 9990 East Cent. Afr. J. S 9990 East Cent. Afr. J. SAngga Witra NandaNo ratings yet
- Mandibular Ameloblastic Carcinoma in A Young Patient: A S E E P O R TDocument5 pagesMandibular Ameloblastic Carcinoma in A Young Patient: A S E E P O R TYasmin Salwa LestariNo ratings yet
- Ca EndometriumDocument10 pagesCa Endometriumoktaviany810No ratings yet
- Rare Tumour - Sebaceous Carcinoma of The ScalpDocument2 pagesRare Tumour - Sebaceous Carcinoma of The ScalpInternational Organization of Scientific Research (IOSR)No ratings yet
- Int J Dermatology - 2022 - Iwasawa - Diagnostic Difficulties in Secondary Syphilis A Case ReportDocument3 pagesInt J Dermatology - 2022 - Iwasawa - Diagnostic Difficulties in Secondary Syphilis A Case ReportArmando NogueraNo ratings yet
- Melanoma With Striking Adenocarcinomatous DifferentiationHUMANSDocument11 pagesMelanoma With Striking Adenocarcinomatous DifferentiationHUMANSgranulomatous pneumoniaNo ratings yet
- UC Davis: Dermatology Online JournalDocument4 pagesUC Davis: Dermatology Online Journalma hNo ratings yet
- Diagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasDocument8 pagesDiagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasAffan AdibNo ratings yet
- Melanoma Treatment (PDQ®) - National Cancer InstituteDocument33 pagesMelanoma Treatment (PDQ®) - National Cancer InstituteAnil RajaniNo ratings yet
- Small Cell Neuroendocrine Carcinoma of Bartholin's Gland: A Case ReportDocument4 pagesSmall Cell Neuroendocrine Carcinoma of Bartholin's Gland: A Case ReportAfrican Journal of Medicine and Pharma ResearchNo ratings yet
- Cancer-3 (HSS 2305) - F2022 (PowerPoint PDFDocument65 pagesCancer-3 (HSS 2305) - F2022 (PowerPoint PDFzahra.lalani14No ratings yet
- Jcad 2 8 30Document3 pagesJcad 2 8 30Mariana ValerianoNo ratings yet
- Piis1319453413000660 PDFDocument10 pagesPiis1319453413000660 PDFZhakiAlAsrorNo ratings yet
- Publications 011Document4 pagesPublications 011utamiNo ratings yet
- Ijohns 2015083115062935 PDFDocument6 pagesIjohns 2015083115062935 PDFradifNo ratings yet
- Biomarkers in MelanomaDocument6 pagesBiomarkers in MelanomaMatthew NgNo ratings yet
- Subcutaneous MetsDocument27 pagesSubcutaneous MetsDavidJohnsonNo ratings yet
- Langerhans Cell Histiocytosis Followed by Folliculotropic Mycosis FungoidesDocument4 pagesLangerhans Cell Histiocytosis Followed by Folliculotropic Mycosis FungoidesYuniita VerayantiiNo ratings yet
- Merkel Cell Carcinoma - Final Term PaperDocument10 pagesMerkel Cell Carcinoma - Final Term Paperdelisha dNo ratings yet
- Metastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyDocument7 pagesMetastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyJafet Gonzalez EstradaNo ratings yet
- Clinical and Genetic Characterization of Basal Cell Carcinoma and Breast Cancer in A Single PatientDocument7 pagesClinical and Genetic Characterization of Basal Cell Carcinoma and Breast Cancer in A Single PatientMahmoud AlshahatNo ratings yet
- Journal of Dermatology ResearchDocument17 pagesJournal of Dermatology ResearchAthenaeum Scientific PublishersNo ratings yet
- Cutaneous Collision Cancers Review HUMANSDocument5 pagesCutaneous Collision Cancers Review HUMANSgranulomatous pneumoniaNo ratings yet
- Melanocytic Lesions: A Case Based ApproachFrom EverandMelanocytic Lesions: A Case Based ApproachMai P. HoangNo ratings yet
- Ovarian Myeloid Sarcoma, Gynecol Oncol Rep 2023Document7 pagesOvarian Myeloid Sarcoma, Gynecol Oncol Rep 2023Semir VranicNo ratings yet
- Metastastic Vulvar Squamous Cell Carcinoma Mimicking Genital HerpesDocument3 pagesMetastastic Vulvar Squamous Cell Carcinoma Mimicking Genital HerpesSteve EdwardNo ratings yet
- Stem Cell Cancer: By: Monali.R.Bhakta Sem: 8 Roll No: 86Document13 pagesStem Cell Cancer: By: Monali.R.Bhakta Sem: 8 Roll No: 86coolharsh111No ratings yet
- Mixed Müllerian Tumor of UterusDocument3 pagesMixed Müllerian Tumor of UterusInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Tumores Mucinosos Del Ovario Con Nodulo Mural Case Report 2020Document10 pagesTumores Mucinosos Del Ovario Con Nodulo Mural Case Report 2020Jairo Lino BNo ratings yet
- Updateonmerkelcell Carcinoma: Paul W. HarmsDocument17 pagesUpdateonmerkelcell Carcinoma: Paul W. Harmssanti lestariNo ratings yet
- Recent Advancements in Skin Cancer Treatment: A Critical ReviewDocument31 pagesRecent Advancements in Skin Cancer Treatment: A Critical ReviewRajat GoyalNo ratings yet
- Metastatic Squamous Cell Carcinoma of The ButtockDocument3 pagesMetastatic Squamous Cell Carcinoma of The ButtockApple StarNo ratings yet
- Biomedicines 09 00171 v2Document33 pagesBiomedicines 09 00171 v2farihNo ratings yet
- 6703 23736 1 PBDocument3 pages6703 23736 1 PBReski Harlianty HarliNo ratings yet
- 1 s2.0 S1110036217300481 MainDocument3 pages1 s2.0 S1110036217300481 MainPutri YingNo ratings yet
- Eplasty 19 Ic 18Document8 pagesEplasty 19 Ic 18gausahajasikepoNo ratings yet
- Neuro Oncol 2014Document9 pagesNeuro Oncol 2014quirinalNo ratings yet
- Tumor OrbitaDocument4 pagesTumor OrbitaIda Bagus Deny PrayudiNo ratings yet
- Molecular Biomarkers in Sinonasal Cancers: New Frontiers in Diagnosis and TreatmentDocument13 pagesMolecular Biomarkers in Sinonasal Cancers: New Frontiers in Diagnosis and TreatmentventyperdanasariNo ratings yet
- Marj OlinDocument4 pagesMarj OlinAnonymous gpbQrsNo ratings yet
- Immunotherapy of SarcomaDocument150 pagesImmunotherapy of SarcomaAr-pardo RogerNo ratings yet
- 18 Extra-GuptaNDocument3 pages18 Extra-GuptaNGalih rarang gatiNo ratings yet
- Immunobiology of Merkel Cell Carcinoma: Implications For Immunotherapy of A Polyomavirus-Associated CancerDocument10 pagesImmunobiology of Merkel Cell Carcinoma: Implications For Immunotherapy of A Polyomavirus-Associated CancerzahidNo ratings yet
- Second Primary TumorDocument7 pagesSecond Primary TumorJames BondNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
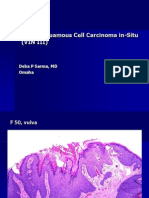
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
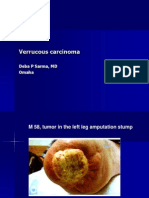
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationAbdallah AlasalNo ratings yet
- Pall CareDocument81 pagesPall Careडा. सत्यदेव त्यागी आर्यNo ratings yet
- Medical Laboratory Tests: Tang PingDocument42 pagesMedical Laboratory Tests: Tang Pingapi-19916399No ratings yet
- Gastroenterology EsophagusDocument2 pagesGastroenterology EsophagusJayanthNo ratings yet
- CONFIDENTIAL MEDICAL REPORT Viginie Alicia Massie - FEVERDocument2 pagesCONFIDENTIAL MEDICAL REPORT Viginie Alicia Massie - FEVERtahuchubby sesetanNo ratings yet
- Nurse Aide Practice TestDocument10 pagesNurse Aide Practice TestHerman Matias75% (4)
- Bidding Document For: Tender Bid Should Contains The Following Information / DocumentsDocument12 pagesBidding Document For: Tender Bid Should Contains The Following Information / Documentskhurram AbbasiNo ratings yet
- Hypothyroidism in Context: Where We've Been and Where We're GoingDocument12 pagesHypothyroidism in Context: Where We've Been and Where We're Going1130017003 AIMMATUL CHANIFAHNo ratings yet
- Clinical Nursing Care ScenarioDocument1 pageClinical Nursing Care ScenarioLeary John Herza TambagahanNo ratings yet
- AortographyDocument31 pagesAortographyWendy Escalante100% (1)
- Burkitt LymphomaDocument51 pagesBurkitt LymphomaDee100% (2)
- Exercise Is Essential For Osteoarthritis: The Many Benefits of Physical ActivityDocument1 pageExercise Is Essential For Osteoarthritis: The Many Benefits of Physical ActivityFrancisco Javier Luza RamosNo ratings yet
- Purpose of Urine TestDocument5 pagesPurpose of Urine TestDinar Surya UtamiNo ratings yet
- Medical AbbreviationDocument37 pagesMedical AbbreviationJessica QueNo ratings yet
- Patient Health Questionnaire-15: Physical SymptomsDocument1 pagePatient Health Questionnaire-15: Physical SymptomssorcNo ratings yet
- Pharmacotherapy of PneumoniaDocument56 pagesPharmacotherapy of Pneumoniahoneylemon.co100% (1)
- First Aid KitDocument15 pagesFirst Aid Kitdex adecNo ratings yet
- NCP For Preterm LaborDocument2 pagesNCP For Preterm LaborP Sta Maria75% (4)
- Clinical Virology, 3rd EditionDocument1,416 pagesClinical Virology, 3rd EditionRichard Balili100% (1)
- Presented By: Ayu Aqilah Binti Khazani Nurul Dhiya Binti Hassannuddin Narisa Samaradhantia Supervisor: DR .Dr. Khalid Saleh SPPD-KKV, FinasimDocument34 pagesPresented By: Ayu Aqilah Binti Khazani Nurul Dhiya Binti Hassannuddin Narisa Samaradhantia Supervisor: DR .Dr. Khalid Saleh SPPD-KKV, Finasimekhysyifka0% (1)
- Polio VirusDocument7 pagesPolio Virusapi-387894697No ratings yet
- VP Shunt Pada NPHDocument1 pageVP Shunt Pada NPHmiranti fauziNo ratings yet
- AReviewon Nutritional AnemiaDocument9 pagesAReviewon Nutritional AnemiaZainab Abubakar GwanduNo ratings yet
- Heat Stroke and Heat Exhaustion: An Update: Invited ReviewDocument5 pagesHeat Stroke and Heat Exhaustion: An Update: Invited ReviewMohd TaufiqNo ratings yet
- Health 7 Quarter 3 SummaryDocument8 pagesHealth 7 Quarter 3 Summarymr3632682No ratings yet
- Chest TraumaDocument47 pagesChest Traumafrenee aradanasNo ratings yet
- Plete Angelinesimulation Assignment ActivityDocument2 pagesPlete Angelinesimulation Assignment ActivityRoel John Atamosa CasilacNo ratings yet
- Medicine MCQS JULY 2023 SOLVEDDocument15 pagesMedicine MCQS JULY 2023 SOLVEDLijo JoNo ratings yet
- Psychological Disorders: Quick ReviewDocument5 pagesPsychological Disorders: Quick Reviewshah FahadNo ratings yet
- PsychiartryDocument7 pagesPsychiartryNeeraj SahuNo ratings yet