You might also like
- Maternal and Child Health Nursing Reviewer-CompleteDocument66 pagesMaternal and Child Health Nursing Reviewer-Completeposh003892% (39)
- The Science of LoveDocument13 pagesThe Science of LoveZin Ortiz Zitro100% (1)
- Britt Research ProposalDocument4 pagesBritt Research Proposalapi-258119727No ratings yet
- Science: Quarter 3 - Module 2: The Female Reproductive System and The Menstrual CycleDocument25 pagesScience: Quarter 3 - Module 2: The Female Reproductive System and The Menstrual Cyclejane mamon100% (1)
- Ovarian New Growth CASE REPORTDocument53 pagesOvarian New Growth CASE REPORTAbbey Jane Ayro69% (13)
- Ass Ectopic PregnancyDocument10 pagesAss Ectopic PregnancyPriyaNo ratings yet
- Feedback Mechanisms and Menstrual CycleDocument90 pagesFeedback Mechanisms and Menstrual CycleThird WillowNo ratings yet
- Summative-Test in Science 10Document8 pagesSummative-Test in Science 10trexia autida0% (1)
- UntitledDocument22 pagesUntitledAiza Ragsag CabiltesNo ratings yet
- Lesson 101 Reproductive SystemDocument52 pagesLesson 101 Reproductive SystemtheacielaNo ratings yet
- Menstrual CycleDocument19 pagesMenstrual CycleBasmat HassanNo ratings yet
- Ncma 217 MidtermsDocument15 pagesNcma 217 MidtermsCharmaine BautistaNo ratings yet
- Labor: Ismailaliff Amirul Syameer Luvin Raj Samuel Das Eizzat Fahmi Syafikah Shaamim Fadzilah AisyahDocument26 pagesLabor: Ismailaliff Amirul Syameer Luvin Raj Samuel Das Eizzat Fahmi Syafikah Shaamim Fadzilah AisyahSyameer Yusof100% (1)
- Sexual Response Fertiliztion ImplantationembryoDocument38 pagesSexual Response Fertiliztion ImplantationembryoHana-Lou TaquiquiNo ratings yet
- Ovarian Cysts: Presented by Neha Barari Assistant Professor SNSRDocument52 pagesOvarian Cysts: Presented by Neha Barari Assistant Professor SNSRBhawna JoshiNo ratings yet
- Ovarian and Menstrual CyclesDocument48 pagesOvarian and Menstrual CyclesNadir KhanNo ratings yet
- Menstruation and FertilizationDocument54 pagesMenstruation and FertilizationJanaica JuanNo ratings yet
- Menstrual CycleDocument33 pagesMenstrual CycleRyan Paul BilgeraNo ratings yet
- Feedback Mechanism in Female RSDocument21 pagesFeedback Mechanism in Female RSnathanielstanaj.mNo ratings yet
- Maternal and Child Health IDocument772 pagesMaternal and Child Health Ikarendelarosa06100% (6)
- Reproductive HealthDocument72 pagesReproductive HealthLance Andre V. RosalNo ratings yet
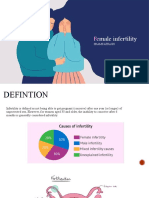
- Female InfertilityDocument32 pagesFemale InfertilityShams AtrashNo ratings yet
- Vaginal Bleeding During PregnancyDocument67 pagesVaginal Bleeding During PregnancyLunaLureNo ratings yet
- Everything To Know About Menstruation.Document3 pagesEverything To Know About Menstruation.KofiNo ratings yet
- OvulationDocument4 pagesOvulationAshleyn Mary SandersNo ratings yet
- Case StudyDocument23 pagesCase StudyLucero HyacinthNo ratings yet
- Menstrual CycleDocument9 pagesMenstrual Cyclevarshasharma05100% (2)
- Menstrual CycleDocument16 pagesMenstrual CycleMark MarigmenNo ratings yet
- Menstrual Cycle 1Document16 pagesMenstrual Cycle 1CoxnxkNo ratings yet
- Menstrual PeriodDocument2 pagesMenstrual Periodapi-206847705No ratings yet
- Gce Presentation Group 11Document11 pagesGce Presentation Group 11Covenant UbahNo ratings yet
- Obstetric Nursing RevisedDocument345 pagesObstetric Nursing Revisedkarendelarosa06100% (1)
- Maternity Nursing NotesDocument7 pagesMaternity Nursing NotesazitaaaaaNo ratings yet
- Female Reproductive SystemDocument42 pagesFemale Reproductive SystemAhmie MarcosNo ratings yet
- Menstrual CycleDocument2 pagesMenstrual CycleShekinah MaeNo ratings yet
- Female Reproductive System & Menstrual CycleDocument77 pagesFemale Reproductive System & Menstrual Cyclebrandonbrandino624No ratings yet
- PERIOD MEMES Only Girls Can UnderstandDocument27 pagesPERIOD MEMES Only Girls Can UnderstandChloeNo ratings yet
- Blocked Fallopian TubesDocument6 pagesBlocked Fallopian TubesJuliet AmondiNo ratings yet
- Menstrual CycleDocument19 pagesMenstrual CycleCarlos MasNo ratings yet
- 3 The Menstrual CycleDocument41 pages3 The Menstrual CycleBryan Lloyd Ballestar RayatNo ratings yet
- The Human Reproductive SystemDocument53 pagesThe Human Reproductive Systemapi-406307933No ratings yet
- Ovulation - ReproDocument14 pagesOvulation - ReproMuhammad Abbas WaliNo ratings yet
- LECTURE NO 4 - Mentrual CycleDocument3 pagesLECTURE NO 4 - Mentrual CycleRebell AeonNo ratings yet
- Stages of Menstrual Cycle - Menstruation, Ovulation, Hormones, MorDocument13 pagesStages of Menstrual Cycle - Menstruation, Ovulation, Hormones, MorMc Cobert AlipioNo ratings yet
- Menstrual Cycle: Anna Liza F. Rabo RN, ManDocument31 pagesMenstrual Cycle: Anna Liza F. Rabo RN, ManFhei Lya Dee TioNo ratings yet
- Menstrual CycleDocument19 pagesMenstrual Cycleraghuram reddyNo ratings yet
- Menstrual History and Determining Ovulation: Prepared By: Danmar C. Yepez, RM, BSM Cp101-InstructorDocument23 pagesMenstrual History and Determining Ovulation: Prepared By: Danmar C. Yepez, RM, BSM Cp101-InstructorlaarnieNo ratings yet
- UntitledDocument35 pagesUntitledPrincess Diane M. RagusNo ratings yet
- Maternal ReviewerDocument6 pagesMaternal ReviewerSherma Sheikh karimNo ratings yet
- 1 Normal Ob (Menstrual Cycle) : Glora P. de Leon, RN, RM, ManDocument75 pages1 Normal Ob (Menstrual Cycle) : Glora P. de Leon, RN, RM, ManJoan VillafrancaNo ratings yet
- Menstrual CycleDocument13 pagesMenstrual Cyclesilanpillay0No ratings yet
- Normal MenstruationDocument2 pagesNormal MenstruationNoella MenesesNo ratings yet
- Female Reproductive System: Sexual Health UnitDocument47 pagesFemale Reproductive System: Sexual Health UnitСухоставець Наталія ПетрівнаNo ratings yet
- Menstruatio N: Prepared By: Lirio, Riza D. BSN 2-1Document26 pagesMenstruatio N: Prepared By: Lirio, Riza D. BSN 2-1Eidyc_Etak_Sin_8542No ratings yet
- INFERTILITYDocument19 pagesINFERTILITYAnu LijuNo ratings yet
- AssignmentLab12 RodriguezDocument5 pagesAssignmentLab12 RodriguezRAZELLE JOY CATIAN RODRIGUEZNo ratings yet
- Menstrual CycleDocument26 pagesMenstrual CycleYeyeth Jabaybay TabolongNo ratings yet
- Adv - Adolescence and Reproduction - Lec Notes 7Document7 pagesAdv - Adolescence and Reproduction - Lec Notes 705 Nalin PrabhatNo ratings yet
- FEMALEDocument60 pagesFEMALETri JaraNo ratings yet
- MaternalDocument6 pagesMaternalBlessed Glaiza MarianoNo ratings yet
- 2 The Process of Reproduction - Alsree - MalunjaoDocument30 pages2 The Process of Reproduction - Alsree - Malunjaojose mari chanNo ratings yet
- Ovarian Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOvarian Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 3 out of 5 stars3/5 (2)
- EBM Case Write Up - To Rule Out MERS COVDocument5 pagesEBM Case Write Up - To Rule Out MERS COVFaiz TaqiuNo ratings yet
- EBM Surgery CWU - Testicular CancerDocument5 pagesEBM Surgery CWU - Testicular CancerFaiz TaqiuNo ratings yet
- The DoctoRDocument3 pagesThe DoctoRFaiz Taqiu0% (1)
- Physician's Life As A PatientDocument4 pagesPhysician's Life As A PatientFaiz TaqiuNo ratings yet
- Essay Untuk Pinjaman MARA 2012Document2 pagesEssay Untuk Pinjaman MARA 2012Faiz Taqiu100% (4)
- Career Essay (For MARA Interview)Document4 pagesCareer Essay (For MARA Interview)Faiz Taqiu100% (4)
- Practical Gynecology 221002 234708Document44 pagesPractical Gynecology 221002 234708Muhammad RizgarNo ratings yet
- Pre-Board Exam For November 2009 NLEDocument28 pagesPre-Board Exam For November 2009 NLEFranz.thenurse6888100% (1)
- 0009KK003556F2Document3 pages0009KK003556F2Sunny SharmaNo ratings yet
- OBGYN NotesDocument29 pagesOBGYN NotesavavNo ratings yet
- AZOL 100 & AZOL 200: Azolnew Zealand Data SheetDocument11 pagesAZOL 100 & AZOL 200: Azolnew Zealand Data SheetSwempi Melchiadi AbollaNo ratings yet
- ASYNCHRONOUS-ACTIVITY-Module 1Document7 pagesASYNCHRONOUS-ACTIVITY-Module 1Grant Wynn ArnucoNo ratings yet
- Course Outline Human ReproductionDocument3 pagesCourse Outline Human ReproductionButter VittoriNo ratings yet
- Progestin Only ContraceptionDocument4 pagesProgestin Only ContraceptionTareq SawanNo ratings yet
- DR Khaled A-Malek MCDocument63 pagesDR Khaled A-Malek MCﻣﻠﻚ عيسىNo ratings yet
- Early Pregnancy SymptomDocument77 pagesEarly Pregnancy Symptomzulaikhaabdrahman100% (1)
- DLP VALDERAMA Carla Ann - BSE SCIENCE IV DEMODocument19 pagesDLP VALDERAMA Carla Ann - BSE SCIENCE IV DEMOMarvi ValdezNo ratings yet
- Effects of Food Habits On Menstrual Cycle Among Adolescent GirlsDocument10 pagesEffects of Food Habits On Menstrual Cycle Among Adolescent GirlsDon Baraka DanielNo ratings yet
- Case Study On EmotionsDocument5 pagesCase Study On EmotionsAnonymous q93WlgNo ratings yet
- Hubungan Peran Ibu Sebagai Pendidik Remaja Dengan Kesiapan Menghadapi Menarche Pada Siswi Usia 10 - 12 Tahun Di SD Negeri 3 Sedayu Bantul YogyakartaDocument20 pagesHubungan Peran Ibu Sebagai Pendidik Remaja Dengan Kesiapan Menghadapi Menarche Pada Siswi Usia 10 - 12 Tahun Di SD Negeri 3 Sedayu Bantul YogyakartaWaddah MukarromahNo ratings yet
- Brightstone Transitions Medical HistoryDocument5 pagesBrightstone Transitions Medical HistoryRidhwan Hakim ZainurinNo ratings yet
- IB and Bi 12 Menstrual-Cycle Worksheet W KeyDocument4 pagesIB and Bi 12 Menstrual-Cycle Worksheet W KeyRhynnieNo ratings yet
- 1.04 Gyne Amenorrhea Dr. DeLeon 2021Document50 pages1.04 Gyne Amenorrhea Dr. DeLeon 2021Allysa Marie CotandaNo ratings yet
- Distribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemDocument3 pagesDistribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemirmaarmiyahNo ratings yet
- Abnormal Uterine BleedingDocument13 pagesAbnormal Uterine BleedingratnacantikNo ratings yet
- Management of Reproductive Health and DysmenorrheaDocument33 pagesManagement of Reproductive Health and DysmenorrheaIntan Permatasari Putri SNo ratings yet
- Lesson Plan BIO565 March - July 2017Document3 pagesLesson Plan BIO565 March - July 2017habibahNo ratings yet
- Topic-Menstural Cycle: Name-Divya Sharma Roll No-8 & Bharti Kotwal Roll No-7Document15 pagesTopic-Menstural Cycle: Name-Divya Sharma Roll No-8 & Bharti Kotwal Roll No-7chanderNo ratings yet
- NCM107 Maternal & Child Nursing - Module 2Document10 pagesNCM107 Maternal & Child Nursing - Module 2Marco VillanuevaNo ratings yet
- 12bio Assignment ch123Document14 pages12bio Assignment ch123Krishna GovilNo ratings yet
- Final Thesis Document MenorrhagiaDocument64 pagesFinal Thesis Document MenorrhagiaSuman Samal MagarNo ratings yet