You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Industrial Review ProjectDocument74 pagesIndustrial Review ProjectMeghna SardaNo ratings yet
- Unleash Your Inner Creativity - Embracing The Power of ImaginationDocument1 pageUnleash Your Inner Creativity - Embracing The Power of ImaginationJohnNo ratings yet
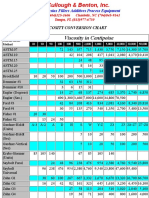
- Viscosity Conversion ChartDocument2 pagesViscosity Conversion ChartCorvetteNo ratings yet
- Grade 10 Mathematics - Review of The BasicsDocument42 pagesGrade 10 Mathematics - Review of The BasicsDouglas WeberNo ratings yet
- Strategic Significance of Arabian SeaDocument4 pagesStrategic Significance of Arabian SeaShamshad Ali RahoojoNo ratings yet
- Proposal For Piping Spool Prefab Line (Fixed Type)Document57 pagesProposal For Piping Spool Prefab Line (Fixed Type)Ranjith Kumar100% (1)
- Digital GCB Brochure FinalDocument12 pagesDigital GCB Brochure FinalantonioNo ratings yet
- Pipeline Stress Analysis With Caesar IIDocument16 pagesPipeline Stress Analysis With Caesar IIshane maxwellNo ratings yet
- New Applications December 2021Document135 pagesNew Applications December 2021sachinmaster434No ratings yet
- Non Euclidean GeometryDocument11 pagesNon Euclidean GeometryGeorge TsavdNo ratings yet
- Potato Peel As PackagingDocument6 pagesPotato Peel As PackagingMyra PacumioNo ratings yet
- NervousDocument19 pagesNervousEmmanuel A. GalvanNo ratings yet
- Painting An Icon Step by StepDocument35 pagesPainting An Icon Step by StepVictorIoncu100% (2)
- Specific Attenuation Model For Rain For Use in Prediction MethodsDocument5 pagesSpecific Attenuation Model For Rain For Use in Prediction MethodsНакит ДимитраNo ratings yet
- 2011 Retaining Wall Design Guide USFS Mohney 5 LVR Slope StabilityDocument559 pages2011 Retaining Wall Design Guide USFS Mohney 5 LVR Slope StabilitySima ViorelNo ratings yet
- 22a-RSJ Runway Beam Check-Simply Supported-Hand OperatedDocument2 pages22a-RSJ Runway Beam Check-Simply Supported-Hand OperatedParthiban Arivazhagan100% (1)
- Coal India Probation Closure Exam QuestionsDocument32 pagesCoal India Probation Closure Exam QuestionsAjeet Kumar100% (1)
- DPP 10 Jee Advanced Revision DPP BDocument33 pagesDPP 10 Jee Advanced Revision DPP BBhagwat Singh UdawatNo ratings yet
- Nctiabe'19 Paper-AparajitaDocument6 pagesNctiabe'19 Paper-AparajitaAparajita VibuNo ratings yet
- Content 22380 PDFDocument4 pagesContent 22380 PDFTriranga BikromNo ratings yet
- Lab 9 PDFDocument17 pagesLab 9 PDFAfie RosmanNo ratings yet
- AEC 4th UnitDocument28 pagesAEC 4th UnitShakthi PriyaNo ratings yet
- Practices of Commercial Construction - Cameron AndresDocument629 pagesPractices of Commercial Construction - Cameron AndresEnrique Rodriguez SanchezNo ratings yet
- D C G E: Epsom and ST Helier University HospitalsDocument1 pageD C G E: Epsom and ST Helier University HospitalscarlcthayerNo ratings yet
- Tooth Mobility PedoDocument47 pagesTooth Mobility PedoFourthMolar.comNo ratings yet
- IIB-7 G.R. No. L-17240 Villongco Vs Florencio MorenoDocument3 pagesIIB-7 G.R. No. L-17240 Villongco Vs Florencio MorenoJoovs JoovhoNo ratings yet
- Health 4 LAS Q4Document39 pagesHealth 4 LAS Q4Chariza TadeoNo ratings yet
- Pune Metagraph CoDocument49 pagesPune Metagraph CoAmol JadhavNo ratings yet
- Immo OffDocument32 pagesImmo Offsoptea60% (5)
- Sylvania Engineering Bulletin - Fluorescent Lamps 1985Document26 pagesSylvania Engineering Bulletin - Fluorescent Lamps 1985Alan Masters100% (1)