Professional Documents
Culture Documents
Schizophrenia NCMH Case Study
Schizophrenia NCMH Case Study
Uploaded by
Dexter FloresOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Schizophrenia NCMH Case Study
Schizophrenia NCMH Case Study
Uploaded by
Dexter FloresCopyright:
Available Formats
Republic of the Philippines DIVINE WORD COLLEGE OF BANGUED Bangued, Abra
NURSING DEPARTMENT
A case study on
SCHIZOPHRENIA, UNDIFFERENTIATED TYPE
In Partial Fulfillment of the Requirements in NCM 204 (RLE) Leading to the Degree Bachelor of Science in Nursing
National Center for Mental Health Mandaluyong, City Pavilion 10
Submitted to:
Myra P. Locquiao, R.N., R.M., MAN. Clinical Instructor
Submitted by: Roderick C. Ancheta
July 26, 2009 SY 2009-2010 BATCH 2010
I.
BACKGROUND OF THE STUDY
A. INTRODUCTION Schizophrenia is a group of psychotic reactions that affect multiple areas of an individuals functioning including thinking and communication, perceiving and interpreting reality, feeling and demonstrating emotions and behaving in a socially accepted manner. This condition causes distortion and bizarre behavior, thoughts, movements, emotions and perceptions. This condition is usually diagnosed in late adolescence or early adulthood and rarely manifest in childhood. The symptoms of schizophrenia are divided into two major categories; the positive and negative symptoms. The positive symptoms include delusions and its types, hallucinations, loose associations and bizarre or disorganized behavior while the negative symptoms includes restricted emotions, anhedonia, avolition, alogia, catatonia and social withdrawal. Most clients with schizophrenia have a mixture of both types of symptoms. The diagnosis of this condition usually is made when the person begins to display more actively positive symptoms of delusions, hallucinations and disordered thinking. Onset may be abrupt but most clients slowly and gradually develop signs and symptoms such as social withdrawal, unusual behavior, loss of interest and neglected hygiene. Schizophrenia is also classified into five types and diagnosed according to the clients predominant symptoms. Paranoid type is characterized by persecutory or grandiose delusions, hallucinations and occasionally excessive religiosity hostility and aggressive behavior. Disorganized type is characterized by inappropriate or flat affect, disorganized speech and disorganized behavior. The catatonic is characterized by marked psychomotor disturbance, either motionless or excessive motor activity. Motor immobility may be manifested by waxy flexibility or stupor. Excessive motor activity is apparently purposeless and not influenced by external stimuli. Other features include extreme negativism, echolalia, echopraxia or even mutism. Undifferentiated type is characterized by mixed schizophrenic symptoms of other types along with disturbances of affect and behavior. The last type which is residual is characterized by the absence of prominent delusions, hallucinations, disorganized speech and grossly disorganized or catatonic behavior. Our client was classified and diagnosed as schizophrenia, undifferentiated type. Which means, that she demonstrated mixed schizophrenic symptoms of others but not enough of them to define its particular type.
B. THEORETICAL FRAMEWORK According to Learning Theory, the irrational ways of handling situations, the distorted thinking and the deficient communication patterns of person with schizophrenia are a result of poor parental models in early childhood. Children learn what they are exposed to on daily basis, from parents who have their own significant emotional problems. Thus, the child does not develop skill forming good interpersonal relationships which she possesses when she grows up. If this was not to be resolve, it will lead to some emotional distortions. Sullivan was the principal proponent of learning theory, believing that the developing individual was shaped by social interactions. Therefore, the complex feelings, thoughts and behavioral expressions grew out of the individuals experiences with those closest to her or him. For example, if the childs father was mean and dictatorial, the perception may have generalized to other men in positions with authority. Or if the childs mother coped problems by projecting blame onto others, the child learn this pattern of behavior and alienated others by putting it into practice. As what the child seen at early stage of life, that was the things she will be doing when she grow up to cope problems and save her or his ego identity. This theory I think was indicated to my client who have difficulty in coping when she was still at normal state of life. Later, she developed untoward behaviors when triggers the development of her condition and was diagnosed to have schizophrenia, undifferentiated type. This is in relationship with the relationship of the client with the other members of the family especially her parents who were to be the model of the young minds. She grew up with a mean father and mother which she never inculcated during the interactions. And from this case, the client tend to blame her mother for the development of the condition.
C. PERSONAL DATA Name: Age: Birth date: Birthplace: Address: Gender: Civil Status: Nationality: Religion: Educatonal Attaiment: Date of Admission: Time of Admission: Admitting Physician: Chief Complaints: According to the Father, the client was hostile and showing untoward behaviors. She was claiming that she was a prophet and speaks most often about satan. The informant also added that the client often says that she was not accepted by their church because of her mother who sold herself to satan when they went to a tour around the world. Admitting Diagnosis: Final Diagnosis: Agency: Undifferentiated Schizophrenia, Chronic and Unstable Undifferentiated Schizophrenia, Manageable National Center for Mental Health, Mandaluyong City 48 y/o February 17, 1961 Marikina City 98 Malaya Street, Malanday Marikina City Female Married Filipino Jehovas Witness College Graduate July 11, 2001 2:40 PM
D. CHIEF COMPLAINT According to the Father, the client was hostile and showing untoward behaviors. She was claiming that she was a prophet and speaks most often about satan. The informant also added that the client often says that she was not accepted by their church because of her mother who sold herself to satan when they went to a tour around the world.
E. HISTORY OF PRESENT ILLNESS The present condition of the client started when she was 34 years old. Due to some circumstances, the client become hostile and showed untoward behaviors and even hurting her own self. She was readmitted on July 11, 2001 with a diagnosis of Schizophrenia undifferentiated type, Chronic and unstable. She has a regular check up and taking the medications religiously but her condition worsened when she was not accepted to their church. The clients condition now was already stable and manageable, but sometimes she still manifests some symptoms like hallucinations and tends to mumble to herself. F. PAST MEDICAL HISTORY The client has a regular medical check up when she was still at normal state. Shes been taking antihypertensive drugs due to the rise and fall of her blood pressure. The client was first admitted at the National Center for Mental Health at the year 1995 because of hostility, untoward behaviors and social withdrawal. She was then diagnosed to have Schizophrenia, undifferentiated type. According to the client herself, she always heard voices and even saw things which were vague for her. Meaning, she was experiencing visual and auditory hallucinations. That was why her father brought her at the center. She was been manageable and was in and out at the center for 6 years. At the year 2001, at 2:40 in the afternoon of July 11, she was readmitted accompanied by her father for she experienced again symptoms like hallucinations and delusions. The client then denied the presence of auditory and visual hallucinations and claimed to have a good sleep. She also added that she was been admitted at the center before and taking up medications like Haloperidol. The client was been at the National Center for Mental Health for about 14 years but sometimes in and out due to the progressive state of her condition.
G. PAST PERSONAL HISTORY The client was a graduate of College Degree at the University of the East. She was married and has three children. Shes been affiliated religiously at their church as a member and she was been active to their church activities. She spends most of her time on her affiliation and has a normal state dealing with her colleagues. H. PAST FAMILIAL HISTORY The client belongs to a well to do family. They were five siblings in their family and have already their own families respectively and she was the only one who has the condition. Her father was businessman and so with her husband. The client has three children and they were studying at a prestigious school in Metro Manila. According to her, their family fond of going into different places in the country and also abroad. On both paternal and maternal side, they do not have a history of schizophrenia and she was the first to have the condition. The client has a mean father and she never speak to much about her mother. I. PAST SOCIAL HISTORY The client was an active member of her Religious affiliation. She was dedicated and goes along with her colleagues religiously and acts accordingly. Shes fond of dealing with her co-members. The client always remembers that she was singing at their church with other group members. The clients social atmosphere changed when one day she was not already a member of their church. She always claimed that she was rejected due to the wrong doing of her mother. She became socially withdrawn, suspicious and later became hostile and has disorganized behavior.
II.
PHYSICAL AND MENTAL ASSESSMENT
A. GENERAL APPEARANCE The client appears stated with her age of 48 years old, wearing a pink dress with a face towel at her back, well groomed and with good personal hygiene. Shes taking a bath everyday with a good daily routine. The client has a good posture, gait and coordination. During interaction, she has a good eye to eye contact and an appropriate affect or facial expression with regards to a certain situation. She was well nourished and has a fair skin as evidenced by her good body built and has no sleeping difficulties by the absence of dark circles under her eyes. She was well oriented with time, place, date and reality. The client considered the interview the interview as a normal thing and she was guided accordingly with no harsh or offending questions thrown to her during the interview. She was cooperative with consistency of speech and behavior. B. GENERAL BEHAVIOR AND ACTIVITY The client sometimes lethargic and catatonic stupor during interactions. There are also times that she was restless where she cant remain still. She has also hand tremors which were involuntary, purposeless rhythmic movements. C. ORIENTATION The client was well oriented on date, time, place and reality. She can relate to past experiences and able to organized ideas and thoughts related to her present condition. She know and aware that she was at the National Center for Mental Health.
D. AFFECT AND MOOD The client show appropriate affect with regards to a certain situation. But sometimes, she suddenly change in expression of mood and this makes hard to identify whether she was on stated condition and willing to cooperate and interested with the interaction. Sometimes, there was an alteration of the affective state of the client which was inappropriate and contrary to her feelings and emotions. E. THOUGHT PROCESS AND CONTENT Even the client was at the center, she has a normal and logical thought process. What she uttered was meaningful and with sense. She didnt use confabulation nor circumstantial. She can easily catch up what the interviewee mean and answer relevant to the questions. F. MEMORY, PRESENT AND REMOTE
The client good memory but sometimes she had lapses. She can recall and remember her past experiences and important events and people in her life. What were discussed in the previous days were recalled which were integrated on the present scenario on the interaction. G. JUDGMENT The condition of the client only started when she was on her early adulthood. Therefore, it doesnt mean that she can not make decisions on its own for she was at the center. She can formulate and think of other alternatives which later beneficial for solving her own problems. H. INSIGHT The client was knowledgeable and aware of her condition that she was at the national center for mental health. She knows the state of her illness being manageable and how was the progression with regards to her rehabilitation and in response to medication regimen and psychotherapies. She was able to respond of what was going on and can comprehend appropriately. I. INTELLECT She has a good sense of reasoning but it was limited. She was able to pinpoint and defend her answers but if asked for the main reason why she was at the center, she cant answer directly. J. COPING MECHANISMS The client has good pattern in handling stressors that arises in her life. Since she was able to formulate ideas and alternatives in order to divert her attention her problems, she just did her responsibilities at the center and just enjoyed the therapies especially during plays for her not to think or not be bothered by her problems even in a short period of time. K. DEFENSE MECHANISM In the case of my client, she used denial as a defense mechanism. In the reason why she was at the center, she elaborated that she only wanted to rest because she was already tired and exhausted, but in fact, shes been hostile and doing unacceptable manner. In some of the activities that were done, the client never excels in such, but became a winner in the play therapies; therefore she was compensating on her actions that was not succeeded on her part. And one thing also that I noticed was that, she tend and often said that her attitude of mumbling and rattling of speech was due to limited
visitation by her family. Shes blaming and concluding that her physical handicap was due to that event and it was a defense mechanism called conversion.
III.
PSYCHOPATHOPHYSIOLOGY
A. PSYCHODYNAMICS According to Freud, schizophrenia is a form of regression, back to the oral stage of development. The oral stage is the first stage of psychosexual development. A baby is born a bundle of id; ID is self-indulgent and concerned only with a satisfaction of his/her needs. There is a need to gratify these impulses but their experiences in the real world result in conflict. People with schizophrenia are overwhelmed by anxiety because their egos are not strong enough to cope with id impulses. In schizophrenia, this can lead to self-indulgent symptoms such as delusions of grandeur, Jesus Christ. As the patient is still living in the real world, this may result in further DELUSIONS such as hearing voices which may have an ultimate authority such as God. This explanation suggests that schizophrenia has a psychosomatic cause the origin is solely in the mind. At best it could only be a partial explanation of some symptoms, e.g. delusions. In reality, Freud is denying the very experience of patients with schizophrenia. It is unscientific and extremely difficult to test. Concepts such as repression are difficult to observe and measure, although this difficulty does not invalidate the theory. The theory is based on unrepresentative samples, case studies, from which it is difficult to generalize. And it involves poor methodology. The theory fails to account for gender differences - the onset for males is around 20 years, and for females 30 years. Nor does the theory explain why, prior to diagnosis, their behavior has appeared normal. Further more, it excludes a consideration of the environment. Dysfunctional Families This explanation suggests that schizophrenia is the result of dysfunctional families. In contrast to the biological or medical approach which may be regarded as more humane, attaching no blame to the individual, this model by implication is attaching blame to the family. BATESON (1956) claimed that parents predispose their children to schizophrenia by communicating in double binds. Double binds are a no-win situation for the child, e.g. a parent might complain about a child, lack of affection, but when the child does give affection, s/he is told that s/he is too old for that. BATESON used the term double bind to explain these ideas of contradictory messages. Emotions and Environments
Support for this view comes from the work of BROWN (1966) who examined the progress of patients with schizophrenia discharged from hospital. BROWN found that those patients who came from families characterized by high expressed emotion (high conflict, constant interference) were more likely to return to hospital in a shorter period of time. 58% of patients returned to high EE families experienced a relapse compared with 10% returning to low EE families. The implications of this research are that the environment has a significant role to play in the course of the development of schizophrenia. However, the direction of causation is unclear, it may be that living with a person with schizophrenia is causing hostility and high expressed emotion within the family. Alternatively, it may be the family that is causing the relapse. The effects of stress on the immune system and on the incidence of disease and illness are well-known. If stress has a role in physical illness, it may well have a role in mental illness. Cognitive Deficits Also, it may be noted that schizophrenia is characterized by cognitive deficits, disorganized speech, hallucinations, delusions, and a cognitive model focuses more tightly on these deficits. Deficits in information processing may leave people vulnerable to the behaviors typically seen as symptoms of schizophrenia. The cognitive approach tends to be descriptive rather than explanatory and tend to use the biological model to explain the origin of schizophrenia. Research does suggest that people with cognitive deficits are highly susceptible to stress. Diathesis-Stress Model The diathesis-stress model combines biological and genetic factors with levels of stress. Diathesis refers to a predisposition (innate) and the stress is environmental (nurture). This model suggests that mental disorders are the result of an interaction between nature and nurture. Finnish study revealed that none of the adopted children raised in healthy families developed schizophrenia, but 11% in severely disturbed families went on to do so. The biopsycho-social approach is a more eclectic approach to studying and understanding schizophrenia. The idea that schizophrenia is the result of schizophrenogenic families is based on retrospective studies and may be unhelpful and highly destructive. Today, high expressed emotion families which are hostile, critical, and over-involved, are seen as maintaining schizophrenia rather than causing it. However, it should be noted that many patients with schizophrenia are estranged from their families. It does seem as if there is a role for attributions of relatives. Weisman (1998) found that relatives who tend to attribute positive symptoms and delusions to a person mental illness do not hold them accountable. Relatives attributing negative symptoms tend to become angry and critical. There are higher relapse rates in families with highly critical attributions
Biological/Medical Model: Genetic Influences
This model suggests that schizophrenia is rooted in our physiology and is treated as a disease or illness. The model operates at the level of genes, brain structure, brain chemistry, hormones, and disease/illness. Schizophrenia has a tendency to run in families. First degree relatives are 18 times more at risk. However, family studies are conducted using interview techniques. Interviews are retrospective involve looking back at the past and our memories are often inaccurate. Interviews are also subjective based on opinions and interviewees do not have the benefit of diagnostic criteria. Furthermore, family history studies fail to separate genes and environment. This suggests that genes do play a significant role in schizophrenia. However, the concordance rate is not 100%. There remains the problem that Tienaris study is ongoing and the critical period for the onset for females has only just been reached. These figures are likely to be underestimates as the figures fail to include information about the biological father. Genes do not operate in isolation and are linked to brain chemistry Brain Chemistry This level of explanation would suggest an imbalance of neurotransmitters or chemical messengers in the brain. The dopamine hypothesis suggests that schizophrenia is a result of excess levels of dopamine in the brain. The evidence for this hypothesis lies in the fact that phenothiazines reduce symptoms of schizophrenia. They inhibit levels of dopamine activity. L-Dopa is a synthetic dopamine releasing drug which induces the symptoms of schizophrenia. Also, Parkinsons disease, shaking of limbs are common side effects associated with the effects of anti-psychotic medication. Parkinsons disease is associated with low levels of dopamine. Further support for the dopamine hypothesis comes from studies of amphetamines. These release dopamine at the central synapses. They worsen the symptoms of schizophrenia.
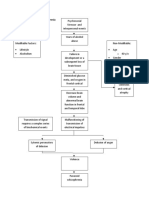
B. PREDISPOSING AND PRECIPITATING FACTORS The relationship between members of the family has a big relationship in the development of the condition. Parenting in the early stage of life which the child seen during those years, she may manifest and carried until shed grow up. As to the blaming of others for problems and maybe a problem with authority figures. In this case, the person may be able to be withdrawn and may not develop interpersonal or social relationships, she may also vulnerable to stress as she never know what were the alternatives for the coping of her problems. Nature of work also predispose the development of the condition, if the person is always ridiculed even she thinks that she did her best and her work is good but it has no effect on his boss, feeling of guilt a and inadequacy and inferiority begins. Thats why, the person maybe have fascinating effects that someday her boss would be please on what she had done or maybe think of hostility against her boss.
Low Frustration Tolerance also a factor that triggers the development of the illness. Like on the nature of work, she may not be able to cope up with the problems she may encounter that makes her think of something that were not appropriate to reality and acts contrary. Severe Religiosity was also included as a part of the past social history of the client. She was very active to her religion and she did anything for that her faith in god and to their church may not be ruined. But one that predisposed was the wrong act of her mother that the latter cause her to be rejected to their church. In this case, the client become hostile and shows untoward behaviors towards other and towards self. Since the client has well to do family, socio economic status has a lesser effect on the development of her condition, but the main thing connected to it was the attitude of family members like her father which is very mean and strict to them. Other factors include the acquisition of influenza virus by the mother during the second trimester of pregnancy. The virus may create maternal antibodies. In the fetus, there become auto antibodies which an external source of developmental change. In this case, this is a great factor in the development of adult schizophrenia. Others include trauma like head injuries or diseases during childhood and substance abuse.
C. PSYCHOPATHOLOGY Schizophrenia is a group of psychotic reactions that affect multiple areas of an individuals functioning including thinking and communication, perceiving and interpreting reality, feeling and demonstrating emotions and behaving in a socially accepted manner. This condition causes distortion and bizarre behavior, thoughts, movements, emotions and perceptions. This condition is usually diagnosed in late adolescence or early adulthood and rarely manifest in childhood. In relation to the predisposing and precipitating factors, the clients cause of illness is severe religiosity, parenting (family relationships and attitudes towards other), low frustration tolerance and the nature of work. The onset of the symptoms usually occurs in the adolescence or early adulthood and the onset can be gradual or sudden. Course of schizophrenia is variable and remissions may occur. Some clients may recover completely. Some have chronic, unremitting disorder. Schizophrenic clients have difficulty in perceiving reality and disturbances on ego. These individuals have poor sense of identity as well as lowered self esteem. The signs and symptoms which manifested by the client when admitted were delusions (grandiose, jealous, persecution and reference), hallucinations (auditory and
visual), hostility, loose associations, disorganized behavior, social withdrawal and restricted emotions.
D. DRUG STUDY DIVINE WORD COLLEGE OF BANGUED BANGUED, ABRA DRUG STUDY NO.1 GENERIC/ BRAND NAME Haloperidol/ Haldol CLASSIFICATION MECHANISM OF ACTION A butyrophenone that probably exerts antipsychotic effects by blocking post synaptic dopamine receptors in the brain. CONTRAINDICATION Hypersensitivity to drug and those with Parkinsonism, coma or CNS depression SIDE & ADVERSE EFFECT CNS: severe extra pyramidal reactions, dyskinesia, seizures, lethargy CV: hypotension, tachycardia GI: anorexia, constipation, dry mouth NURSING IMPLICATION - Monitor patient for tardive dyskinesia which may occur after prolong use. - Watch for signs and symptoms of extra pyramidal effects - Tell client to relieve dry mouth with sugarless candy EVALUATION
Antipsychotic
DOSAGE 5 mg tablet once a day
INDICATION Psychotic Disorders
THERAPEUTIC PRECAUTION EFFECTS Exerts antipsychotic effects to the client Use cautiously in elderly clients, those with history of seizures, CV disorders and those using lithium.
DIVINE WORD COLLEGE OF BANGUED BANGUED, ABRA DRUG STUDY NO.2 GENERIC/ BRAND NAME Chlorpromazine CLASSIFICATION MECHANISM OF ACTION A piperidone phenothiazine that may block post synaptic dopamine receptors in the brain. CONTRAINDICATION Hypersensitivity to drug and those with Parkinsonism, coma or CNS depression SIDE & ADVERSE EFFECT CNS: severe extra pyramidal reactions, dyskinesia, dizziness, drowsiness CV: tachycardia GI: nausea constipation, dry mouth NURSING EVALUATION IMPLICATION -Monitor blood pressure regularly. - Watch for orthostatic hypotension -Monitor for tardice dyskinesia -Watch for signs and symptoms of neurolyptic malignant syndrome -Advise client not to chew extended release capsule before swallowing
Antipsychotic
DOSAGE 100 mg capsule once a day
INDICATION Psychotic Disorders
THERAPEUTIC PRECAUTION EFFECTS Exerts antipsychotic effects to the client Use cautiously in elderly clients, those with history of seizures, CV disorders and respiratory disorders
IV.
NURSE PATIENT INTERACTION A. PROCESS RECORDING
ORIENTATION PHASE (JULY 06, 2009)
OBJECTIVES: to establish rapport and trust and cooperation to establish roles and purposes of the meeting to identify clients problems and clarify expectations
ASSESSMENT: Wears pink dress with a face towel at her back Well groomed with good personal hygiene with good posture and gait Has good eye contact during interaction, good mood and appropriate affect Well oriented on time, place and identity Well nourished with fair skin Spontaneous speech and with relevant answers Able to recall past experiences and relate to the present situation and reality Alert and had good judgment and reality
ORIENTATION PHASE (July 7, 2009 1:00 Pm) NURSE Magandang Hapon po, kumusta po kayo? THERAPEUTIC RATIONALE COMMUNICATION Okay naman ako, Giving recognition Greeting the magandang hapon client indicates din. the she is acknowledge and recognize as a person. Ganun ba? Giving Information This gives the client an overview what were the reasons why you were there and make her aware what are the boundaries of the interaction, the purposes, the time and place and who were to be involved CLIENT
Ako po si Roderick Ancheta, and magiging student Nurse ninyo. Tawagin mo naang po akong Rhod. Galing po ako Sa Divine Word College of Bangued. Simula po sa araw na ito, July 7, 2009 makakasama niyo po ako at makakausap hanggang sa susunod na Linggo, July 16, 2009. Magsisimula po tayo ng alas otso ng umaga hanggang alas tres ng hapon. Pag-uusapan po natin ang inyong mga karanasan at mga dahilan kung paano po kayo napunta ditto. Lahat po ang pag-uusapan natin ay mananatiling sikreto at tayo lamang pong dalawa ang nakakaalam. Tapos na po akong magpakilala, pwede po bang kayo naman po ang magpakilala?
Ako si Charito Laureano, naktira sa Marikina City.
Providing General Leads
Ilang taon nap o ba kayo?
48 years old na ako.
Seeking information
It encourages the client to continue what she is saying and that the nurse is active in listening. Helps the client facilitate thoughts, feelings and ideas clearly.
Matagal na po ba kayo rito?
Maari po ba ninyong ilahad kung ano po ang dahilan kung pano po kayo napasok ditto?
Fourteen years na Seeking Information ako rito pero yung 6 years, pabalik-balik ako at yong walong taon diretso hanggang ngayon. Ipinasok ako ng Exploring tatay ko ditto tsaka gusto ko na ding magpahinga at magrelax. Seeking Information
Helps the client facilitate thoughts, feelings and ideas clearly.
Helps them both the client and the nurse to examine the issue more fully.
Ano po sa palagay ninyo ang dahilan kung bakit kayo ipinasok na tatay niyo rito? Ano po ba ang trabaho ninyo dati at nasabi po ninyong pagod na kayo?
Di ko na maalala. Basta ipinasaok nlang nila ako rito. Bale tinutulungan ko lang yong tatay ko sa pagtitinda? Ano po ung mga itinitinda Mga pare parts ng ninyo? mga sasakyan Ano pong kurso ang Business tinapos ninyo, maari kop o Management ako bang malaman? sa University of the East. May mga gusto pa po ba Wala na Rhod. kayong sabihin sakin?
Seeking Information
Seeking Information Seeking Information
Offering self
Cge po Nanay Charito, bukas po ulit ha. Magsisimula nap o tayo ng alsa otso ng umaga. Mag-isip po kayo ng mga ikukwento ninyo sa akin ha.
Sige, maraming salamat. Paalam
Giving Recognition
Making oneself available and showing interest and concern to the client let them feel more comfortable and will develop further trust. Greeting the client indicates the she is acknowledge and recognize as a person.
WORKING PHASE (July 08, 2009) OBJECTIVES: To identify issues and concerns causing problems To guide client to examine feelings and responses To develop coping skills and more positive self image To examine consistency of thoughts and ideas
ASSESSMENT: Well dressed with pink dress Well groomed with pink hair band With good eye contact during interaction and oriented on date, time, place and identity With euthymic mood and appropriate affect With hand tremors on both hands Spontaneous speech, consistent answers to questions asked Has good communication skills, insight and judgment Alert, able ti think abstractly and make generalizations
WORKING PHASE (DAY 1 July 8, 2009) NURSE Magandang Hapon po, Nanay Charito. THERAPEUTIC RATIONALE COMMUNICATION Magandang Giving recognition Greeting the umaga din Rhod. client indicates the she is acknowledge and recognize as a person. Maaga kasi akong Making observations To make them nagising kaya aware what are naligo na ako. their actions and Masaya ako dahil what the client andito ka na feels. naman. Nagpakilala tayo Summarizing This seeks to sa isat isa at bring out the pinag-usapan important points natin kung bakit of the ako andito? discussion and increase awareness to the client Gusto ko lang Seeking information magrelax at magpahinga Kumakanta Seeking information lamang ako. CLIENT
Napansin ko po, bagong ligo na kayo, kumusta po ang araw ninyo.
Maaari niyo po bang ilahad kung ano yung ginawa natin kahapon?
Ano po uli yung dahilan kung bakit po kayo andito? Ganun po ba. Kapag wala po tayong activity ano po ung kadalasan ninyong gingawa? Ano po ung paborito ninyong kanta? Ano naman po ung mga nasa isip at nararamdaman ninyo kapag kayo ay kumakanta ng religious song?
Kahit anong religious song Gumagaan pakiramdam ko dahil di ako pinababayaan ng Diyos.
Seeking Information Encouraging expression Encouraging the client to make her own appraisal rather than to accept opinions from others.
Sa activity po natin kanina Masaya at medyo na Music and arts therapy, malungkot? ano po ang nararamdaman ninyo habang ginagawa ang activity? Ano pong dahilan at Naalala ko kasi
Encouraging expression
Seeking information
nasabi po ninyong malungkot? Ang ibig niyo po bang sabihin ay gusto nap o ninyong umuwi at maksama ang pamilya ninyo? Ano naman po yung mga naiisip ninyong paraan o solusyon para makauwi na kayo?
yong mga anak ko at pamilya ko. Oo, gusto ko nang Translating into umuwi. feelings
Magpapakabuti ako ditto at sinusunod ko yunmg mga sinasabi ng mga nurses at doctor. Ano naman po ang una Magsisimba ako niyong gagawin kapag para nakalabas na kayo ditto? magpasalamat sa Diyos at mamamasyal kaming buong pamilya Maari niyo po bang May tatlo akong ibahagi sa akin tungkol sa anak, dalawang inyong pamilya? lalaki at isang babae. Nasaan po sila ngayon? Nag-aaral sila Sino po ang nag-aalaga sa Yung tatay at kanila? asawa ko. Ano po ba ang pangalan Fernando yung ng asawa at Tatay Ninyo? asawa ko at yung tatay ko eh clarito. Ano po yung trabaho nila? Wla nasa bahay lang yung asawa ko, ung tatay ko naman ay nasa shop. Sinabi po ninyo kahapon Pagod na kasi ako na gusto niyo ppong eh, kaya gusto ko magpahinga at magrelax. nang magpahinga. Iyon lang po ba ang dahilan? Sa palagay niyo po ba Oo, kasi konti makakapgpahinga po kayo lang yung mga rito kung andito po kayo? ginagawa. May gusto pa po ba Wala na Rho. kayong ibahagi sa akin?
Exploring
This technique is to verbalize clients feeling of what she said indirectly Helps them both the client and the nurse to examine the issue more fully.
Seeking information
Seeking information
Seeking information Seeking information Seeking information
Seeking information
Seeking information
Seeking information
Offering Self
Sige bukas ulitCharito.
Salamat, Paalam
Giving Recognition
DAY 2 (July 9, 2009) NURSE Magandang umaga po Nanay Charito, andito na naman ako para kausapin kayo. Kumusta po ang tulog niyo? Kumain nap o ba kayo? CLIENT (Client smiled) Magandang Umaga din Mabuti naman Katatapos lang at uminom nari ako ng gamut. (Client smiled) THERAPEUTIC COMMUNICATION Giving recognition Offering self RATIONALE
Seeking information Seeking information
Mabuti po kung ganun. Sige po magsimula na tayo Tungkol pos a napagusapan natin na paborito niyo pong kanta, ano ulit ang mga yun? Wow, ang galling pop ala ninyong kumanta.
General leads
Mga religious songs. Gusdto mo kumanta ako. (Client sung) Salamat
Clarifying
Giving recognition
Clarifies further knowledge and understanding on what is verbalized Greeting the client indicates the she is acknowledge and recognize as a person.
Saan po ninyo natutunan yun? Ano naman po ang pangalan ng simbahan ninyo? Ano naman po ung mga naaalala ninyo sa simbahan ninyo? Maari po ba ninyong sabihin sa akin?
Sa simbahan naming, active kasi ako doon. Jehovas Witness
Seeking information
Seeking information
Masaya (Client become silent) (Client become silent)
Seeking information
Silence
Making silence let the client formulate and organize ideas and makes feel the client that she is
understood and with companion. May sasabihin pa po ba kayo sa akin? Sige po Nanay Charito, bukas po ulit. Punta na po tayo dun sa mga kasamahan natin at may gagawin po tayong activity. Wala na. Seeking Information Greeting the client indicates the she is acknowledge and recognize as a person.
(Client smiled Giving Recognition and just followed)
DAY 3 (July 10, 2009) NURSE Magandang umaga po. CLIENT Magandang umaga din THERAPEUTIC RATIONALE COMMUNICATION Giving recognition Greeting the client indicates the she is acknowledge and recognize as a person. Seeking information Making Observations To make them aware and to know what really the client feels
Kumusta naman kayo ditto? Napansin kop o kanina nung nag-eexercise po tayom parang matamlay po kayo, maaari niyo po bang sabihin sa akin ang dahilan? Ano po bang pangalan ng mga anak ninyo?
Mabuti naman at nakakatulog din Naiisip ko lang yung mga anak ko. Parang nakikita ko sila kapag andito ka. Yung panganay, si Clarence, 19 taon na siya, tapos si Frederick, 18 naman at tsaka si Ruth, magteten years old na siya. Si Clarence, sa UST. Nursing din siya kagaya mo. Si Frederick ay sa UE, civil engineering at si Ruth sa POLA.
Seeking information
Saan po nag-aaral yung mga anak ninyo?
Seeking information
Ang gagaling pala ng mga anak ninyo Nanay Charito.
Salamat
Giving Recognition
Habang pinag-uusapan po natin sila, parang naluluha po kayo, ano po ang dahilan?
Sige po, ipagpatuloy niyo lang.
Kahapon sa activity natin, ang saya-saya po ninyo.
Namimiss ko na kasi sila at naaawa ako sa kanila kasi di ko sila maalagaan dahil andito ako sa Mental Lalo na ksi yung bunso, di ko siya naalagaan at nagyon malaki na siya at pasalamat ako di siya pinabayaan ng Diyos. Opo
Making Observations
Greeting the client indicates the she is acknowledge and recognize as a person. To make them aware what are their actions and what the client feels.
Giving general leads
Giving recognition
Nanalo nga rin po kayo sa mga games, ano po ang nararamdaman ninyo?
Ano pa po?
Sige po Nanay Charito, hanggang sa susunod ulit. May gagawin po tayo nagyon, puntahan nap o natin yung mga kasama natin.
Masay, kahit papano nakakalimutan ko yung mga problema ko at para rin sa mga anak ko yun, inspirasyon ko kasi sila. Miss ko na sila, gusto ko nang umuwi. Sige (client smiled)
Encouraging expression
Greeting the client indicates the she is acknowledge and recognize as a person. Encouraging the client to make her own appraisal rather than to accept opinions from others.
Giving general leads
Giving recognition
Greeting the client indicates the she is acknowledge and recognize as a person.
DAY 4 (July 13, 2009) NURSE Hello po Nanay Charito, magandang umaga. Andito na naman po ako. CLIENT Magandang umaga din THERAPEUTIC RATIONALE COMMUNICATION Giving recognition Greeting the client indicates the she is acknowledge and recognize as a person. Seeking information Giving recognition Summarizing. This seeks to bring out the important points of the discussion and increase awareness to the client Clarifies further knowledge and understanding on what is verbalized To make them aware what are their actions and what the client feels.
Ano po ang nararamdaman ninyo? Pwede niyo po bang sabihin sa akin yung mga napag-usapan natin noong nakaraang lingo?
Ano po ang naaalala ninyong bugtong?
Napansin ko po nung Makita ninyo yung larawan, napahawak po kayo sa inyong dibdib, ano po yung naalala ninyo? Ano po yung mga naalala ninyo tungkol sa inyong mga anak?
Iyon lang po ba ang dahilan? May mga gusto pa po ba kayong sabihin? Sige nanay Charito, pumunta nap o tayo sa mga kasamahan natin.
Masay kasi may makakausap na naman ako. Marami. Nagmusic and arts tayo, tapos may palaro at tsaka yung bugtungan na bingyan natin ng mga importansiya yung mga sagot. Di ko sigurado yung tanong, pero yung sagot ay yung gatas ng ina? Unaware naman ako dun sa nagawa ko. Naalala ko lang yung mga anaqk ko lalo na yung bunso. Lahat kasi sila nagbote lang, di ko sila napasuso. Maganda pala ang gatas ng ina. Oo Wala na. Sige
Clarifying
Making observations
Seeking informations
Seeking information Seeking information Giving recognition.
DAY 5 (July 15, 2009) NURSE Magandang umaga nanay Charito. CLIENT Magandang umaga din Rhod. THERAPEUTIC RATIONALE COMMUNICATION Giving recognition Greeting the client indicates the she is acknowledge and recognize as a person. Seeking information Seeking information Seeking information Giving recognition Seeking information
Kumusta po ang tulog ninyo? Kumain nap o ba kayo?
Mabuti naman.
Oo, inom na rin ng gamut. Ano pong petsa ngaun ang July 14 ay nagyon anong araw? ay Miyeskules. Magaling. Tama po. (client Smiled) Sa tuwing nag-uusap po Mga anak ko, tayo, ano po yung mga miss na miss ko naaalala ninyo? na kasi sila at yung mga lugar na parati naming pinupuntahan. Saan po yung mga lugar Sa Batangas, na parati ninyong Palawan, tapos sa pinupuntahan? Thailang nung nagtour kami. Ano po yung ginagawa Nagsuswimming niyo dun kapag kami, pumupunta po kayo? namamasyal at kumakain. Kung sakali po, Sa Batangas, makakalabas kayo ditto, magsuswimming saan po yung lugar na kami. Tapos pupuntahan ninyo at ano punta kami sa yung mga gagawin ninyo? Mall. Bibili kami ng maraming pagkain, mamamasyal kahit saan kasama ang mga anak ko. May gusto pa po ba Wala na. kayong sabihin sa akin? Sige po, puntahan na natin Sige. Salamat yung mga kasama natin, (Client smiled may activity po tayo ulit. and followed)
Seeking information
Seeking information.
Exploring
Helps them both the client and the nurse to examine the issue more fully.
Offering self Giving recognition.
TERMINATION PHASE (July 15, 2009) NURSE Magandang umaga po Nanay Charito. CLIENT Ganu din sayo (Client smiled) THERAPEUTIC RATIONALE COMMUNICATION Giving recognition Greeting the client indicates the she is acknowledge and recognize as a person. Seeking information Giving Information
Kumusta po kayo? Ngayon pong araw na ito, bale ito nap o yung huli nating pagsasamat paguusap. May kunti po tayong programa at maaasahan kop o ba ang kooperasyon ninyo? Nag-enjoy po ba kayo? Sige po, hanggang ditto nalang po an gating paguusap Nanay Charito. Maraming salamat pos a inyong kooperasyon at tiyaga sa pakikinig sa amin.
Mabuti naman Ganun ba, sige.
AFTER THE PROGRAM Nag-enjoy naman Seeking information Maraming salamat Giving recognition din. Paalam (client shoke hands with me)
B. LIST OF NURSING DIAGNOSIS (NANDA)
CUES SUBJECTIVE:
OBJECTIVE: >talks to self frequently > leaves area suddenly without explanation >poor concentrations >Has difficulty maintaining conversations
NURSING DIAGNOSIS Disturbed sensory perception related to loneliness and isolation as evidenced by talking to self frequently, leaves suddenly without explanations, poor concentration and has difficulty in maintaining conversations.
JUSTIFICATION Disturbed sensory perception should be given first priority for the client may manifest untoward behavior towards self and other clients due to misinterpretation of stimuli
SUBJECTIVE: >Gusto ko nang umuwi, miss ko na mga anak ko.
Anxiety related to prolong rehabilitation as evidenced by grimacing, poor eye contact at times, hand tremors and restlessness.
OBJECTIVE: >poor eye contact at times > grimacing > hand tremors > restless SUBJECTIVE: >Malungkot ditto kapag walang student nurse. OBJECTIVE: >sadness > poor eye contact at times >absent of significant others >isolates self in room most of the time
Anxiety level of the client should be given importance for it will also lead the client to danger if uncontrolled. Therefore, it should monitored and managed for the clients safety
Social Isolation related to sadness, poor eye contact at times, absent of significant others and isolation of self in room most of the time.
Social isolation would be the last for it requires least nursing interventions but it should also be given importance for the benefit and success of the clients rehabilitation. The client will be able to develop social skills and social acceptance if it is properly given appropriate nursing interventions.
DIVINE WORD COLLEGE OF BANGUED BANGUED, ABRA Nursing Care Plan 1 CUES SUBJECTIVE: BACKGROUND KNOWLEDGE The client experience disturbed sensory perception which is incongruent with actual stimuli. In this case, the client misinterpreted and acts contrary to what is real. PATIENTS PROBLEM Disturbed sensory perception related to loneliness and isolation as evidenced by talking to self frequently, leaves suddenly without explanations, poor concentration and has difficulty in maintaining conversations. OBJECTIVE OF INTERVENTIONS After Nursing interventions, the client will demonstrate ability to hold conversation without hallucinating and ceases to talk to self. NURSING ACTIONS AND RATIONALE >Establish a therapeutic relationship. _To gain clients trust >Orient the client continuously to actual environment, events and activities. _Frequent orientation helps to present reality to the client >Call the client by name. _Using correct names reinforce reality are reducing hallucinations. >State your reality about the clients hallucinating experience. _The client is helped to distinguish the actual voices which promote reality. >Use clear and distinctive voice _To avoid misinterpretations >Encouraged the client to engaged in activities _Activities are alternatives and distractions to hallucinations >Accept and support feelings of the client _This convey empathy and understanding which reduces fear or anxiety.
OBJECTIVE: >talks to self frequently > leaves area suddenly without explanation >poor concentrations >Has difficulty maintaining conversations
DIVINE WORD COLLEGE OF BANGUED BANGUED, ABRA Nursing Care Plan 2 CUES SUBJECTIVE: >Gusto ko nang umuwi, miss ko na mga anak ko. BACKGROUND KNOWLEDGE Uneasy feeling of discomfort accompanied by autonomic response. The client experiences anxiety for she thought that shell be discharged and be accompanied by her family. PATIENTS PROBLEM Anxiety related to prolong rehabilitation as evidenced by grimacing, poor eye contact at times, hand tremors and restlessness. OBJECTIVE OF INTERVENTIONS After Nursing interventions, the clients leve; of anxiety will be lessened. NURSING ACTIONS AND RATIONALE >Provide therapeutic Environment _To gain clients trust >Be available to client at all times _to make the clients feel valued and has importance. >Stay at the clients and provide a comfortable environment. _To make clients feel valued and relieves the level of anxiety and releases tension >Encourage client to engage self in activities _Activities helps the client divert attention from anxiety and from undesirable behaviors. >Encourage client to acknowledge and express feelings _To explore the cause of feeling of apprehension.
OBJECTIVE: >poor eye contact at times > grimacing > hand tremors > restless
DIVINE WORD COLLEGE OF BANGUED BANGUED, ABRA Nursing Care Plan 3 CUES SUBJECTIVE: >Malungkot ditto kapag walang student nurse. BACKGROUND KNOWLEDGE Aloneness experienced by the individual are perceived as imposed by others and as a negative or threatening state. PATIENTS PROBLEM Social Isolation related to sadness, poor eye contact at times, absent of significant others and isolation of self in room most of the time. OBJECTIVE OF INTERVENTIONS After nursing interventions, the client will be able to engage self in all social activities actively and verbalize willingness to social interactions. NURSING ACTIONS AND RATIONALE >Provide therapeutic Environment _To gain clients trust > Provide a positive reinforcement when client makes moves towards others. _It encourages continuation of efforts. >Promote participation in activities. _This facilitates socialization >Engage other client to interact with the client _this promotes social skills in a safe setting. >Help the client seek out clients to socialize with who have similar interest. _Shared common interest promote more enjoyable socialization which may be repeated. >Praise the client for attempts to seek out others for activities and interactions _Praises promotes repeated positive social behavior.
OBJECTIVE: >sadness > poor eye contact at times >absent of significant others >isolates self in room most of the time
V.
THERAPIES
1. ACTIVITIES OF DAILY LIVING - An activity done by an individual which is necessary for the promotion of good personal hygiene which can be done with or without assistance/ supervision to an individual Objectives: 1. 2. 3. 4. 5. To promote and improve personal hygiene and grooming To promote self-independence To encourage participation Evaluation through return demonstration To develop awareness on home management and community development 6. To develop interpersonal relationship 2. PLAY/RECREATIONAL THERAPY - A technique that makes it possible for the patient to express himself. Free play enables the individual a unique opportunity to discharge strong motion n a secure atmosphere. It is also a form of Psychotherapy for regressed psychotics to an extent of making its impossible to communicate with them through verbal channels Objectives: 1. To help patient interact with other patients in a slightly competitive but thoroughly enjoyable level, manner. 2. The client will be able to express themselves through acceptance and enjoyable mans. 3. To promote diversion from usual routinely experienced by the client in favor of a more dynamic activities. 4. To promote cooperation and sportsmanship 5. Allow free expression of feelings and thoughts. The first activity was not actually a game but we made it as a part of getting to know each other, it was an action song Kumusta Ka. First, the facilitator explains the mechanics of the game. That first, we will sing the song and then turn to the other client until the student nurse will be able to reach her/his partner. Then, the student nurses will kept their name tags and each client will name five of them, the client who will be able to name five will be given a price. The second game was Hep Hep Hurray, as a general rule, the client who will not be able to follow the direction will be out, and only one client will be the winner and have a grand prize while each client was given a consolation prize.
The third game was also an exercise which we made it as a game, the lean forward, and lean backward. The song was sung the student nurses together with the client. Each client will be sitting and follow the action. A client who will not be able to follow will be out of the game. The song was sung faster and faster until only one will be left and never committed a mistake, she will be declared as the winner.
INTERPRETATION AND ANALYSIS: With this therapy, the client showed interest and became a winner at one game, the Hep Hep, Hurray. She showed competitiveness and very active. This time, she said that this activity weve done was a good diversional activity for her to forget her problems.
3. MUSIC AND ART THERAPY - Is the opportunity for socialization and self expression and sometimes realization affected by certain musical activities. Art therapy is the process by letting the patient expresses his feelings and thoughts through various artistic means particularly sketching and drawing. One type of therapy with purposeful use of music and arts as a participative or listening experienced in the treatment of the patient to improve and motivate their mental and emotional state Objectives: 1. To know as a diagnostic tool, collecting signs and symptoms to supply psychiatric and to give correct diagnosis. 2. To release past trauma in life unconsciously. 3. To interpret psychological drawing 4. To discuss emotional problem and to give reasons and ideas regarding such problems 5. To develop interpersonal relationship During this activity, we gave each client one bond paper and a set of crayons. Then, we played a happy and fast music. We let them draw what they feel and later they interpreted it. Secondly, with the set of crayons and another bond paper, we played a sad and slow music and we let them also draw what they really feel. Since my client has hand tremors, she was not able to finish her activity until the song had finished, so we played again the song until all of them were finish doing the activity.
INTERPRETATION AND ANALYSIS: My client had drawn a grain which she said symbolizes as the main source of food. And she also added that she misses her grandfather who was a farmer before. During the sad music, she had drawn a mango and papaya fruit which she explained that she miss to eat those fruits, because of long rehabilitation she was not able to have and eat those favorite fruits of her.
4. BIBLIO-THERAPY - Use of literature, film or feature on creative writing with group discussion to promote self-acknowledgement and inter action of thoughts and feelings. Enhances patients awareness regarding an article of material s well as it increase with the information and content of such reading materials. It stimulates the inner self by expressing their feelings regarding with given story Objectives: 1. To stimulate the psychological, sociological and aesthetic values from books into human character, personality and behavior 2. To provide stimulus for the memory to compare events with their own interpersonal and intra psychic experience. 3. To increase level of understanding with information from the reading materials. In this therapy, we used Bugtungan. We made ten riddles written in a cartolina and each answer corresponding to each riddle was drawn in a bond paper. One by one, each client read the riddle and picked the picture of the answer. After they all answered, we gave importance each answer and we ask also what they know about the picture. Each client was very willing to answer and the activity was done smoothly.
5. OCCUPATIONAL THERAPY - Any activity mental and physical guided to an individual to recover from a handicap.There is an increasing awareness that process and not the product of the process is the greatest importance. Manual recreational and creative technique to facilitate personal experiences and increase social responses and self esteem
Objectives: 1. 2. 3. 4. To improve general performance To obtain essential skills of living To assist in symptom reduction To increase the sense of accomplishment, satisfaction and control over ones own life 5. To increase social responses 6. To increase self-esteem 6. REMOTIVATION TECHNIIQUE - Is a technique of every simple group therapy of an objective nature used in an effort to reach the wounded areas of the patients personality and get them moving in the direction of reality Objectives: 1. To stimulate client to think about something and talk about himself 2. To develop ability to communicate and share idea and experience with others 3. To develop feeling of acceptance and recognition.
VI.
CONCLUSION AND RECOMMENDATIONS As a result of the study and interaction of the client, the following conclusion are being gathered and seen: There is a great influence of the family and significant others in the development and progression of the illness. Severe religiosity can cause a disorder when really obsessed to the religious affiliation itself. Schizophrenia can be manageable with the aid of the family as the main source of strength and hope of the client. Clients who develop this kind of disorder have a connection to their development task which were unmet that makes them vulnerable to stress. In relation to their treatment, psychotherapies were used for the rehabilitation and will prepare the clients for their recovery and readiness to face challenges when they go outside the center. In relation to the management and interventions, close monitoring and guidance were important for the safety of the client especially for the recurrence of the signs and symptoms of the illness.
The following are the recommendations: Constant visitation should be done to the client in order for them to feel valued and cared by the family. Close monitoring should be done to client in order not to develop the recurrence of symptoms which are harmful to them and to other clients. Therapeutic communication should always be used and observed for clients not to be offended for they were already at the rehabilitation area, they have absolutely feelings to be hurt and may feel rejection.
VII.
NARRATIVE REPORT
July 06, 2009 It was the first day of our duty at the National Center for Mental Health. To be honest, I was so nervous. The time when our service van entered the gate of NCMH, my heart beated so fast and I begun trembling because it was the very first times I entered in a mental hospital and soon dealing with clients with different type of disorders. We waited in front of PAGASA Hall when we arrived. We waited for the orientation program to start as a part of the routine before starting our exposure at the institution. We saw lots of students from different schools that will also have their affiliation in the said institution. As we finally entered the hall, the anxiety I felt lessened because of the accommodating speakers like Mrs. Lucila o. Espinoza, the chief nurse. She was so good in speaking. She did talk about therapeutic techniques and therapeutic communications. The second speaker talked about the history of NCMH and the orientation was done smoothly. After the orientation, we went to our designated Pavilion together with our clinical instructor, Mrs. Myra P. Locquiao. She was good and very vocal. We were assigned to Pavilion 10 at the Rehabilitation area and I think we were so lucky because we had already a good teacher, and at the same time we had a good ambiance. We didnt yet get inside the ward but wed already seen the place were we are assigned. The day and the time had gone fast and we went home after a very exciting day. And from the endeavor we had that day I can say that I learned a lot! July 07, 2009 It was the second day of our duty at the National Center for Mental Health. This day, we had our Self-Awareness. One by one, we shared our experiences in life, our weaknesses and strengths, our limitations and our goals in life. Most of us cried because we were able to recall some of our painfull experiences in the past. We finished the selfawareness with a half day session, just in time for us to have our break for lunch. In the afternoon, our Clinical Instructor gave us some briefing before we entered our assigned pavilion. At first, I was not at ease during our first time to enter, but as time passed by, my anxiety was relieved. Finally I met my client. Her name was Charito. Shes nice and friendly. We had our orientation for a short period of time because our stay inside was limited during that time. Since we were assigned at a rehabilitation area, it was easy with us to mingle with our clients because they are already manageable. The notion I had that the clients are harmful was changed because of the way the clients accepted us. We ended our interaction and we went home with smiles on our faces.
July 08, 2009 It was a pleasant Wednesday morning. The day came to spend our whole day stay at the Pavilion 10 where we were assigned. It was a busy day for us and to our clients. As I observed during the activities inside the area, all clients were so active and participative with the activities. Later on, we watched and observed for remotivation therapy, what to be done and what to be discussed. It was demonstrated by a staff and it went so good because of the willingness and active participation of the group. The discussion was all about vegetables, what they get from them and how to make different things out from vegetables to make them beneficial to our healthy living. It was exciting and remembering because of the very bright ideas the clients have. After the activity, we had a follow up sharing about the activity and went out from the area. At exactly 1:00 PM, we entered the area together with our instructor and interacted with our clients. After a while, we gathered and went as a group at the pantry for our next activity. We started with an exercise in order to boast up their energy and motivate them. Our activity was music and arts. I, together with Delmar facilitated the activity and as a warm up, we asked them what they know about music and arts therapy and I couldnt believed that everybody wanted to answer. First, we played a fast music and we let them draw what they felt while listening to the fast music and afterwards, one by one explained their works. Secondly, we also played a soft and sad music and we let them also draw what they feel and think when they heard a sad music and later on, we let them also explained individually. We ended up the activity with their snacks and the activity gone smoothly and also we enjoyed it and I learned a lot including the mechanics and what to do consider in order for the activity to be interesting and memorable to our clients.
July 09, 2009 It was already our fourth day of duty at the Pavilion 10. We joined their flag ceremony and exercises and had a short interaction with our clients. I was so happy because my client had a good mood for the day, she evenly sung a song for me and in return, I did it too. I observed to my client that she always singing a religious song whenever I talked to her about singing and music. In the afternoon, I was shocked how my client turned to have an untoward action for she said that she will be discharged. She dressed up and ready to go home. After a few minutes, and maybe realizing that she will not be discharged, we changed her dress with their usual dress at the Pavilion joined our activity, and this time, the activity we had was play therapy. We played the Hep Hep Hurray, Kamusta Ka, and Lean Forward. It was so funny because I didnt expect that all of them were competitive even the other clients who were very silent and rare to talk.
They were willing to get the prize and declared to be winners. And one more thing was, when we played the lean forward, we even tend to give up because as we sung the song and became faster and faster, our three competitors were very good and no one ever to be a loser, so thats why we declared the three of them to be winners after a v ery long rally. It was an overwhelming experience and I was happy again because of what had happened even were a little bit tired, at least, we had given them happiness and we gave our best for them feel that they were also people who were longing for happiness.
July 10, 2009 It was our last day or the first week of our duty at National Center for Mental Health. And it was an interesting day for me for I will be given a chance again to discover more about the reason why my client was brought to the center. In the early morning, we joined them on their flag ceremony and their exercises. I was little bit embarrassed because sometimes I was not able to follow their steps for I admit that I was not a good dancer, but even just like that, I enjoyed and I hope that it would be beneficial for me to enhanced my dancing skills. After our clients had finished the necessary things they were doing everyday, I had my interaction again with my client and a little while, wed went to the pantry for our next activity. This day, the activity weve done was one of the forms of bibliotherapy, it was Bugtung-bugtungan. We prepared ten questions and all the answers were drawn and they only picked the answers. Each answer of the corresponding riddles were given importance by asking the clients what they think about and from this activity, I learned that this form of therapy will give the clients to explore more and express their own feelings as we dig more about their lives. We ended up with snacks and gave them rewards for their active participation. In the afternoon, we did not enter at the area for we had our discussions and evaluated the activity we had in the morning. As we all know that evaluation was very important in order for us to know our weaknesses and what to be improved for the betterment of the succeeding activities to be done. Wed go home with good smiles on our faces as we remember our clients.
July 13, 2009 It was not a good Monday morning for it was raining very early. The journey to Pavilion 10 continued as we go to our duty. As we waited for the flag ceremony, we cutted out the necessary materials needed for our first activity this morning, art therapy.
For this activity, we prepared cut outs for them to form and this would enhance their hand coordination for their roper manipulation and placement of every cutted parts for the activity. Since the rain stopped pouring for a while, we entered our designated area and interacted with our clients and joined them on their routine activities like the flag ceremony and their daily exercise and after, we proceeded to the pantry for their activity. Since it was an art therapy, it was simple and meaningful even we have our companion school at the pantry, we ended our activity successfully and the output od each client was a butterfly and a flower. As a summary and generalization of what they have done, we asked them their interpretation of the activity and what they felt while doing the activity. They shared their ideas and expressed their feelings. I had the chance also to interact with my client and followed up our activity and she told me that it was her first time to do that activity and cited that she was happy because she had her name and the corresponding student nurse in the activity and she misses to see butterflies especially during her childhood years. I learned that doing this kind of activity, we were given the chance to explore more about our clients and give them the chance to recall their happy moments in life.
July 14, 2009 A good and pleasant Tuesday morning. It was the time we observed socialization activity from other schools but before that, I had an interaction with my client. This gave me the chance to know more about my client and had a follow up on the things she had done and I had noticed especially her attitude upon seeing the breastfeeding mother during our activity with riddles. And out from this, she stated that she was unconscious on what she had done and remembering her children because she didnt have the chance to breastfed her children during their childhood years. In the afternoon, we had our chart reading. Here, I had seen the true condition of my client. On the things she had stated during our interaction, almost all of them were correct but she didnt elaborate much of the true reasons why she had been on the center for several years. I also discovered that she was religiously disturbed because of the cues she uttered during her stay at the center and during the onset of her condition and this was maybe the reason why she was at the center right now. She was been to the center for fourteen years but not consecutively. She was able to go out and be together with her family but later on go back to the center again. I ended the day with having so many questions on my mind why there are people having those kinds of problems and how their own family surpass and cope up with the situation.
July 15, 2009 Its Wednesday again, and only two days left for our stay at the National Center for mental Health. This day, we had our music therapy. We sung the song together and one by one, we asked them what the meaning of the song they had sung was. As a part of it, we gave the time for our clients to show their talents, they sung after the other and so with the student nurses. After all, we gave them their prizes as we promise for their active participation during the art and bibliotherapy. In the afternoon, we had our reporting by twos. We presented our reports and our clinical instructor had her questions and the necessary supplementations. We ended the day with bright ideas as she explained more and shared what she had.
July 16, 2009 The grand socialization day came. The day to say goodbye to our clients. The time to share our remaining times we were together with different schools here in Metro Manila. Since, it was already our last day at the institution, I learned a lot from here and we hope that we had done our parts. Even though we had only short period staying and dealing with our clients we had already developed trust between us student nurses ad so with our clients. From this socialization, we hope still gave them happiness by means of the presentations and games we prepared for them. And this day I thought would be the most remarkable and embarrassing moment during my stay at the national Center for Mental Health because of unfortunate things that was happened before and during the socialization and not to elaborate further. This time, we saw also our clinical instructors from different schools showing their singing talents, and of course our clinical instructor also did her part. During my stay at the National Center for Mental Health, I learned a lot, even though its hard to say goodbye, but its a must. Before we went out form the area where we had our two weeks duty, we gave out token for our patients as a sign of thanksgiving for their active participation and cooperation and also to the warm welcome they had given to us.
You might also like
- Bipolar Case StudyDocument46 pagesBipolar Case StudyNissie Degulacion100% (1)
- Case Study SchizopreniaDocument21 pagesCase Study SchizopreniaRay-ann Sorilla100% (2)
- Undifferentiated Schizophrenia Case Study SampleDocument202 pagesUndifferentiated Schizophrenia Case Study SampleSaro Balberan88% (8)
- Undifferentiated SchizophreniaDocument190 pagesUndifferentiated Schizophreniaallexiscampaner100% (17)
- A Case Study On SchizophreniaDocument11 pagesA Case Study On SchizophreniaRosa Isabel57% (7)
- F20 Schizophrenia Case StudyDocument45 pagesF20 Schizophrenia Case StudyRichard Joseph DomingoNo ratings yet
- Case Study of Paranoid SchizophreniaDocument22 pagesCase Study of Paranoid SchizophreniaFloidas Fernando100% (8)
- Case Study NCMHDocument41 pagesCase Study NCMHDiana Ortiz100% (1)
- Paranoid Schizophrenia - Case StudyDocument181 pagesParanoid Schizophrenia - Case StudyLouie Anne Cardines Angulo77% (26)
- Schizophrenia UndifferentiatedDocument88 pagesSchizophrenia UndifferentiatedHanya Bint Potawan75% (4)
- Bipolar CaseDocument41 pagesBipolar CaseEmariel Dulana25% (4)
- Schizophrenia Case StudyDocument8 pagesSchizophrenia Case Studyaira2350% (2)
- Schizophrenia CaseDocument14 pagesSchizophrenia CaseFrancez Anne Guanzon100% (1)
- Psychiatric Case StudyDocument32 pagesPsychiatric Case Studyrachael86% (35)
- Case Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderDocument37 pagesCase Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderEarl John Natividad89% (9)
- Case Study BipolarDocument22 pagesCase Study BipolarRobert de Guzman Jr.93% (29)
- Paranoid Schizophrenia Case StudyDocument38 pagesParanoid Schizophrenia Case StudyJayson Valeros75% (4)
- Schizophrenia Case StudyDocument75 pagesSchizophrenia Case StudyDatujen Sanayatin100% (1)
- Bipolar 1 Case PresentationDocument111 pagesBipolar 1 Case PresentationJhensczy Hazel Maye AlbaNo ratings yet
- Case Study On SchizophreniaDocument21 pagesCase Study On SchizophreniaAdrian Mallar100% (1)
- Undifferentiated SchizophreniaDocument26 pagesUndifferentiated SchizophreniaVictor Shon100% (2)
- Schizophrenia Case StudyDocument72 pagesSchizophrenia Case StudyNissie Degulacion100% (5)
- Case Study of Undifferentiated SchizophreniaDocument20 pagesCase Study of Undifferentiated SchizophreniaAbegail P Flores100% (2)
- Schizophrenia Case StudyDocument24 pagesSchizophrenia Case StudyRichard Sy100% (3)
- Case Study - Bipolar DisorderDocument24 pagesCase Study - Bipolar Disordermattheus101100% (11)
- Paranoid Schizophrenia Case StudyDocument33 pagesParanoid Schizophrenia Case StudyCherubim Lei DC Flores50% (4)
- Undifferentiated SchizophreniaDocument47 pagesUndifferentiated SchizophreniaChezka Palola100% (1)
- Schizophrenia Case StudyDocument8 pagesSchizophrenia Case StudyJohn Carlo Toledo0% (1)
- Process Recording On Mentally Ill PatientDocument6 pagesProcess Recording On Mentally Ill Patientkyeria40% (5)
- Psychopathology of SchizophreniaDocument2 pagesPsychopathology of SchizophreniaJhe MallariNo ratings yet
- Pathophysiology of SchizophreniaDocument1 pagePathophysiology of Schizophreniasarzlasco090% (1)
- Pathophysiology of Bipolar 1 DisorderDocument1 pagePathophysiology of Bipolar 1 DisorderMark Cau Meran100% (3)
- SchizophreniaDocument30 pagesSchizophreniaThe Legend2011100% (2)
- Pathophysiology of Bipolar DisorderDocument1 pagePathophysiology of Bipolar DisorderGab Abalos100% (2)
- Cases Study On BipolarDocument37 pagesCases Study On BipolarjaoNo ratings yet
- Bipolar Mood Disorder Case RevisionDocument11 pagesBipolar Mood Disorder Case RevisionEden Marie Francisco100% (1)
- Case Study (Undifferentiated Schizophrenia)Document12 pagesCase Study (Undifferentiated Schizophrenia)allenmariec88% (8)
- Schizophrenia Case StudyDocument13 pagesSchizophrenia Case StudyAnonymous Hfrl594No ratings yet
- Psychopathology of Undifferentiated SchizophreniaDocument4 pagesPsychopathology of Undifferentiated SchizophreniaMarlonReyes2011100% (2)
- Psychopathology of Schizophrenia (Client)Document1 pagePsychopathology of Schizophrenia (Client)Robert Joseph Sison67% (3)
- Case Study Paranoid SchizoDocument46 pagesCase Study Paranoid SchizoDiksha Sharma100% (1)
- Mental Case StudyDocument38 pagesMental Case StudyNishaThakuri80% (5)
- Case Study Psychia Bipolar 2Document57 pagesCase Study Psychia Bipolar 2Joule PeirreNo ratings yet
- Pa Tho Physiology of Bipolar Affective DisorderDocument2 pagesPa Tho Physiology of Bipolar Affective DisorderJerome Asuncion67% (3)
- Bipolar NCPDocument2 pagesBipolar NCPJermaine Anne MadayagNo ratings yet
- Schizophrenia NCMH Case StudyDocument45 pagesSchizophrenia NCMH Case StudyHomework PingNo ratings yet
- Schizophrenia NCMH Case StudyDocument45 pagesSchizophrenia NCMH Case StudyNickale Peralta100% (1)
- Abnormal Psychology Vignettes DSM IV-TRDocument4 pagesAbnormal Psychology Vignettes DSM IV-TRpeppermintkittyNo ratings yet
- Recognize and Ward off Dark Psychology: How to Recognize Emotional Manipulation, Expose a Personality Disorder and Lies and Skillfully Fend Off Manipulation TechniquesFrom EverandRecognize and Ward off Dark Psychology: How to Recognize Emotional Manipulation, Expose a Personality Disorder and Lies and Skillfully Fend Off Manipulation TechniquesNo ratings yet
- Eccentric Behavior in Among TeenagerDocument8 pagesEccentric Behavior in Among TeenagerNyimas Irina SilvaniNo ratings yet
- Anti-Social Personality Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAnti-Social Personality Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 3 out of 5 stars3/5 (1)
- Understanding Schizophrenia: Causes, cures, and how to live with schizophreniaFrom EverandUnderstanding Schizophrenia: Causes, cures, and how to live with schizophreniaNo ratings yet
- Personality Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPersonality Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- FiNAL CASE.Document50 pagesFiNAL CASE.John CrisostomoNo ratings yet
- Borderline Personality Disorder: A Complete Guide to the Signs, Symptoms, and Treatment Methods of Borderline Personality DisorderFrom EverandBorderline Personality Disorder: A Complete Guide to the Signs, Symptoms, and Treatment Methods of Borderline Personality DisorderRating: 3 out of 5 stars3/5 (1)
- Kristen Cookie Analysis SolutionsDocument3 pagesKristen Cookie Analysis SolutionsVikram SanthanamNo ratings yet
- Yojana May PDFDocument66 pagesYojana May PDFAyushi KumgupNo ratings yet
- Romania Off Plan Property Investment and OpportunitiesDocument12 pagesRomania Off Plan Property Investment and Opportunitiespropertyinvestment100% (2)
- Agrifoods Strategy WebDocument36 pagesAgrifoods Strategy WebThe Vancouver SunNo ratings yet
- Polygenic Traits and PenniesDocument4 pagesPolygenic Traits and PenniesSekai KamikiNo ratings yet
- MOTION FOR EXECUTION-PesimoDocument4 pagesMOTION FOR EXECUTION-PesimoLeo Archival ImperialNo ratings yet
- Ernst Mach's World Elements - Erik BanksDocument300 pagesErnst Mach's World Elements - Erik Banksphilosoraptor92No ratings yet
- WCFDocument167 pagesWCFsarascrNo ratings yet
- Civil Society Perspectives On Biodiversity and Waste Management in Uganda's Oil and Gas SectorDocument62 pagesCivil Society Perspectives On Biodiversity and Waste Management in Uganda's Oil and Gas SectorAfrican Centre for Media ExcellenceNo ratings yet
- Pistachio & Grapefruit CakeDocument2 pagesPistachio & Grapefruit Cake侯士大100% (1)
- Modules, Hierarchy Charts, and Documentation: After Studying Chapter 3, You Should Be Able ToDocument36 pagesModules, Hierarchy Charts, and Documentation: After Studying Chapter 3, You Should Be Able ToKobinaNo ratings yet
- Accomplishment BRIGADA NarrativeDocument5 pagesAccomplishment BRIGADA NarrativeEditha BallesterosNo ratings yet
- Two-Story Model Home in Belgium Was Produced in One Piece With Europe's Biggest 3D PrinterDocument4 pagesTwo-Story Model Home in Belgium Was Produced in One Piece With Europe's Biggest 3D PrinterKoriNo ratings yet
- Books ListDocument262 pagesBooks Listjamal85% (13)
- Alfredo M. YaoDocument7 pagesAlfredo M. Yaozhaks //100% (3)
- Lec 6 FX ArbitrageDocument31 pagesLec 6 FX ArbitrageAprilNo ratings yet
- Lesson 5 - A Taximan's Story - A Singaporean StoryDocument3 pagesLesson 5 - A Taximan's Story - A Singaporean StoryAngel Grace Opeliña100% (1)
- Golden FleeceDocument88 pagesGolden Fleeceganyesod67% (3)
- Dragonball ZDocument34 pagesDragonball ZVincenzoNo ratings yet
- JETIR1810813Document6 pagesJETIR1810813Chaithra.yNo ratings yet
- Bachrach vs. SeifertDocument3 pagesBachrach vs. SeifertJeryl Grace FortunaNo ratings yet
- Obj. 11 Reflection With Proof of Attendance 1Document2 pagesObj. 11 Reflection With Proof of Attendance 1Roy Bautista ManguyotNo ratings yet
- Fischer, J M - Gustav Mahler (Yale, 2011)Document775 pagesFischer, J M - Gustav Mahler (Yale, 2011)Gabrielamante del Barranco100% (13)
- 3 Asian Values Universality of HRDocument6 pages3 Asian Values Universality of HRElixirLanganlanganNo ratings yet
- Metro Concast v. Allied Banking - Case DigestDocument2 pagesMetro Concast v. Allied Banking - Case DigestLulu RodriguezNo ratings yet
- 15 Lozon V NLRCDocument5 pages15 Lozon V NLRCGie CortesNo ratings yet
- Service Entrance Masts and AccessoriesDocument11 pagesService Entrance Masts and AccessoriesPRABHU SHANKAR MNo ratings yet
- The New Testament in ByzantiumDocument26 pagesThe New Testament in ByzantiumRobert-Andrei BălanNo ratings yet
- Skirt & Anchor Bolt BROWNELL & YOUNG Process Equip. DesignDocument15 pagesSkirt & Anchor Bolt BROWNELL & YOUNG Process Equip. DesignImthiyaz HNo ratings yet
- Art College EssayDocument8 pagesArt College Essayejqdkoaeg100% (2)