You might also like
- Cerebral Herniation Syndromes and Intracranial HypertensionFrom EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNo ratings yet
- Acute Stroke Management in the Era of ThrombectomyFrom EverandAcute Stroke Management in the Era of ThrombectomyEdgar A. SamaniegoNo ratings yet
- Biology Worksheet Sheep Heart DissectionDocument3 pagesBiology Worksheet Sheep Heart DissectionFluphie Bunny0% (1)
- HSA e Isquemia Tardia 2016Document12 pagesHSA e Isquemia Tardia 2016Ellys Macías PeraltaNo ratings yet
- Delayed Cerebral Ischaemia After SAHDocument3 pagesDelayed Cerebral Ischaemia After SAHFebrian Indra Jr.No ratings yet
- Stroke: BackgroundDocument10 pagesStroke: Backgroundjhay-r reyesNo ratings yet
- HSA Aneurism+â-Ítica ICM 2014Document4 pagesHSA Aneurism+â-Ítica ICM 2014Ellys Macías PeraltaNo ratings yet
- "Triple H" Therapy For Aneurysmal Subarachnoid Haemorrhage: Real Therapy or Chasing Numbers?Document0 pages"Triple H" Therapy For Aneurysmal Subarachnoid Haemorrhage: Real Therapy or Chasing Numbers?ganpur01No ratings yet
- Nature-Delayed Neurological Deterioration After Subarachnoid HaemorrhageDocument16 pagesNature-Delayed Neurological Deterioration After Subarachnoid HaemorrhageEyE UVNo ratings yet
- Treating Delayed Ischemic Neurological Deficit After Subarachnoid HemorrhageDocument11 pagesTreating Delayed Ischemic Neurological Deficit After Subarachnoid Hemorrhageanton MDNo ratings yet
- Role of CiticolineDocument20 pagesRole of CiticolinesylviaNo ratings yet
- E2f7 PDFDocument7 pagesE2f7 PDFSujith KumarNo ratings yet
- A Review On Cerebral Ischemic Stroke Mandeep Pundir, Manjinder Kour, Darshdeep SinghDocument11 pagesA Review On Cerebral Ischemic Stroke Mandeep Pundir, Manjinder Kour, Darshdeep SinghParamjeet Kaur Paramedical SciencesNo ratings yet
- DCI MX - NeuroCritCare2023Document15 pagesDCI MX - NeuroCritCare2023Ahida VelazquezNo ratings yet
- Crit Care Clin 2024 Jan 40 (1) 73-88Document16 pagesCrit Care Clin 2024 Jan 40 (1) 73-88aguileradavid.1311No ratings yet
- Thrombolytic Therapy For Ischemic StrokeDocument7 pagesThrombolytic Therapy For Ischemic StrokechandradwtrNo ratings yet
- Treating The Acute Stroke Patient As An EmergencyDocument9 pagesTreating The Acute Stroke Patient As An EmergencyAnonymous EAPbx6No ratings yet
- Stroke ThesisDocument7 pagesStroke Thesisnavysavchenkobellevue100% (1)
- Management of Vasoplegic ShockDocument16 pagesManagement of Vasoplegic ShockxmksmwyspyNo ratings yet
- Intracerebral Hemorrhage Medical TreatmentDocument3 pagesIntracerebral Hemorrhage Medical TreatmentDarrel Allan MandiasNo ratings yet
- Ijms 13 11753 PDFDocument20 pagesIjms 13 11753 PDFVandy IkraNo ratings yet
- Controversies in The Neurosurgical Management of Cerebellar Hemorrhage and InfarctionDocument10 pagesControversies in The Neurosurgical Management of Cerebellar Hemorrhage and InfarctionThiago SouzaNo ratings yet
- Fluid Resuscitation in Haemorrhagic ShockDocument9 pagesFluid Resuscitation in Haemorrhagic ShockbashiruaminuNo ratings yet
- Vasospasm Metaanalysis 2011Document9 pagesVasospasm Metaanalysis 2011mlannesNo ratings yet
- Complications and Management of Brain TumorsDocument18 pagesComplications and Management of Brain TumorsBenedictus Yudha BaskaraNo ratings yet
- Nervous SystemDocument62 pagesNervous Systemmyat252No ratings yet
- Treatment: Stroke UnitDocument6 pagesTreatment: Stroke Unitgraze_hinataNo ratings yet
- Essential Guide to Diagnosing and Treating Ischemic StrokeDocument21 pagesEssential Guide to Diagnosing and Treating Ischemic Strokekuchaibaru90No ratings yet
- Ich Magistris, 2013Document8 pagesIch Magistris, 2013ignasachyntiaNo ratings yet
- Intensive Care Management of Subarachnoid HaemorrhDocument9 pagesIntensive Care Management of Subarachnoid HaemorrhTariku GelesheNo ratings yet
- Bruce C V Campbell Ischaemic Stroke 2019Document22 pagesBruce C V Campbell Ischaemic Stroke 2019yiyecNo ratings yet
- Manejo PostparoDocument17 pagesManejo PostparoAngela Moreira ArteagaNo ratings yet
- Intracranialhemorrhage Andintracranial Hypertension: Evie Marcolini,, Christoph Stretz,, Kyle M. DewittDocument16 pagesIntracranialhemorrhage Andintracranial Hypertension: Evie Marcolini,, Christoph Stretz,, Kyle M. DewittAxel DuncanNo ratings yet
- Dent Clin N Am 50 (2006) 625-633Document9 pagesDent Clin N Am 50 (2006) 625-633lalajanNo ratings yet
- Anticoagulant Therapy For Ischemic StrokeDocument6 pagesAnticoagulant Therapy For Ischemic StrokeDewi LestariNo ratings yet
- Meningitis EskemikDocument17 pagesMeningitis Eskemikakbar011512No ratings yet
- Hsa Icm 2015Document4 pagesHsa Icm 2015Ellys Macías PeraltaNo ratings yet
- Cerebral Vasospasm - OpenAnesthesiaDocument7 pagesCerebral Vasospasm - OpenAnesthesiaAhmet PinarbasiNo ratings yet
- Aneurysmal SAHDocument19 pagesAneurysmal SAHlakshminivas PingaliNo ratings yet
- Original PapersDocument9 pagesOriginal PapersNanda Charitanadya AdhitamaNo ratings yet
- Anemia and Transfusion BJA 2018Document11 pagesAnemia and Transfusion BJA 2018JoelGámezNo ratings yet
- EMBO Mol Med - 2022 - Simats - Systemic Inflammation After Stroke Implications For Post Stroke ComorbiditiesDocument18 pagesEMBO Mol Med - 2022 - Simats - Systemic Inflammation After Stroke Implications For Post Stroke ComorbiditiesAna GabrielaNo ratings yet
- Hemorragia IntracerebralDocument9 pagesHemorragia IntracerebralEdwin Jofred Torres HuamaniNo ratings yet
- Lin 2014Document4 pagesLin 2014zixzaxoffNo ratings yet
- Cardiogenic ShockDocument6 pagesCardiogenic ShockhamadaelgenNo ratings yet
- Terapia SimpatomoduladoraDocument10 pagesTerapia SimpatomoduladorajijocasoNo ratings yet
- 2019 - Brain Functional Reserve in The Context of Neuroplasticity After StrokeDocument10 pages2019 - Brain Functional Reserve in The Context of Neuroplasticity After StrokeEl Tal RuleiroNo ratings yet
- 9 CNS Sequela of CHDDocument9 pages9 CNS Sequela of CHDVictor PazNo ratings yet
- D22e PDFDocument6 pagesD22e PDFLucky Ikram AlfathanyNo ratings yet
- Hypertension: SMF Saraf Rsud Bangli Fakultas Kedokteran Universitas Islam Al-Azhar 2018Document49 pagesHypertension: SMF Saraf Rsud Bangli Fakultas Kedokteran Universitas Islam Al-Azhar 2018Muhammad HidayatullahNo ratings yet
- Review ArticleDocument11 pagesReview ArticleZainuddin Surkan HNo ratings yet
- JRMS 17 396Document6 pagesJRMS 17 396fani rudiyantiNo ratings yet
- Vaso e SpasmoDocument16 pagesVaso e Spasmodrjavier.jorozcoNo ratings yet
- Journal NeuroDocument6 pagesJournal NeuroBetari DhiraNo ratings yet
- Management of Spontaneous Intracerebral Hemorrhage: Stroke (H Diener, Section Editor)Document11 pagesManagement of Spontaneous Intracerebral Hemorrhage: Stroke (H Diener, Section Editor)Deby AnditaNo ratings yet
- Critical Care of Patients With Acute Ischemic and Hemorrhagic StrokeDocument7 pagesCritical Care of Patients With Acute Ischemic and Hemorrhagic StrokeMary Jhane VillanuevaNo ratings yet
- Current Use and Advances in Vasopressors and Inotropes Support in ShockDocument13 pagesCurrent Use and Advances in Vasopressors and Inotropes Support in ShockJose Luis Espino MacielNo ratings yet
- Acute Stroke ArticleDocument10 pagesAcute Stroke ArticlenesredeNo ratings yet
- HIE and CVSDocument11 pagesHIE and CVSakshayajainaNo ratings yet
- Merk & Type Price (RP) Diff (RP)Document13 pagesMerk & Type Price (RP) Diff (RP)Rizka Leonita FahmyNo ratings yet
- Dimenhydrinate in Children With Infectious Gastroenteritis A Prospective, RCT 2009Document13 pagesDimenhydrinate in Children With Infectious Gastroenteritis A Prospective, RCT 2009Rizka Leonita FahmyNo ratings yet
- Merk & Type Price (RP) Diff (RP)Document13 pagesMerk & Type Price (RP) Diff (RP)Rizka Leonita FahmyNo ratings yet
- Kunci Jawaban UKDI Clinic 1 Batch Feb 2016Document1 pageKunci Jawaban UKDI Clinic 1 Batch Feb 2016Christina AprilianaNo ratings yet
- BMD 2011Document5 pagesBMD 2011Rizka Leonita FahmyNo ratings yet
- Post Test Radiologi MEIDocument22 pagesPost Test Radiologi MEIRizka Leonita FahmyNo ratings yet
- 052 Westermeier Journal Neurology NeurophysiologyDocument8 pages052 Westermeier Journal Neurology NeurophysiologyRizka Leonita FahmyNo ratings yet
- Cover Profil SapcoDocument1 pageCover Profil SapcoRizka Leonita FahmyNo ratings yet
- Nebulized Budesonide Added To StandardDocument9 pagesNebulized Budesonide Added To StandardRizka Leonita FahmyNo ratings yet
- Peds 2012-2030Document7 pagesPeds 2012-2030Rizka Leonita FahmyNo ratings yet
- Jurnal Gastro PerforationDocument6 pagesJurnal Gastro PerforationYuke PutriNo ratings yet
- Merk & Type Price (RP) Diff (RP)Document13 pagesMerk & Type Price (RP) Diff (RP)Rizka Leonita FahmyNo ratings yet
- Ajr 07 2955Document7 pagesAjr 07 2955Yogi PrasetioNo ratings yet
- Peds 2012-2030Document7 pagesPeds 2012-2030Rizka Leonita FahmyNo ratings yet
- PDF DIR 5932Document5 pagesPDF DIR 5932Yogi PrasetioNo ratings yet
- Efficacy of Antidepressants in Treating The Negative Symptoms of Chronic Schizophrenia: Meta-AnalysisDocument9 pagesEfficacy of Antidepressants in Treating The Negative Symptoms of Chronic Schizophrenia: Meta-AnalysisRizka Leonita FahmyNo ratings yet
- Amoxicillin For Acute RhinosinusitisDocument8 pagesAmoxicillin For Acute RhinosinusitisTresno JoyoNo ratings yet
- Initial Assessment of Chest X-Ray in Thoracic Trauma Patients Awareness of Specific InjuriesDocument5 pagesInitial Assessment of Chest X-Ray in Thoracic Trauma Patients Awareness of Specific Injurieslorenz_gtlNo ratings yet
- Peds 2012-2030Document7 pagesPeds 2012-2030Rizka Leonita FahmyNo ratings yet
- Lajevardi Et Al-2015-International Journal of DermatologyDocument7 pagesLajevardi Et Al-2015-International Journal of DermatologyRizka Leonita FahmyNo ratings yet
- Procedural Complication of Epidural Anesthesia in Obese PatientDocument6 pagesProcedural Complication of Epidural Anesthesia in Obese PatientAlexNo ratings yet
- CPG KDDocument6 pagesCPG KDBernard LeonardoNo ratings yet
- AHP Excel Template Calculates Weights for Multiple CriteriaDocument6 pagesAHP Excel Template Calculates Weights for Multiple Criteria'Nez CastraNo ratings yet
- NIH Public AccessDocument17 pagesNIH Public AccessRizka Leonita FahmyNo ratings yet
- 86Document5 pages86Faris Aziz PridiantoNo ratings yet
- Jurnal Kulit PVDocument7 pagesJurnal Kulit PVarinsaharaNo ratings yet
- AHP MunawarDocument5 pagesAHP MunawarRizka Leonita FahmyNo ratings yet
- Peds 2012-2030Document7 pagesPeds 2012-2030Rizka Leonita FahmyNo ratings yet
- Tipo y Localizacion de Placenta PreviaDocument6 pagesTipo y Localizacion de Placenta PreviadorissjbNo ratings yet
- Original Article: ISSN: 0976 3325Document4 pagesOriginal Article: ISSN: 0976 3325Rizka Leonita FahmyNo ratings yet
- Hypertension: "The Silent Killer" Because It Generally Has No Symptoms Until Serious Complications DevelopDocument24 pagesHypertension: "The Silent Killer" Because It Generally Has No Symptoms Until Serious Complications Developmaryam ijazNo ratings yet
- IV TherapyDocument3 pagesIV TherapyYalc LapidNo ratings yet
- CH3 Patho D&R AgamDocument30 pagesCH3 Patho D&R AgamS Balagopal SivaprakasamNo ratings yet
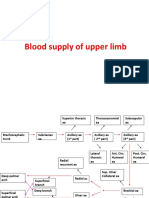
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- Principles and Pitfalls in Coronary Vasomotor Function TestingDocument26 pagesPrinciples and Pitfalls in Coronary Vasomotor Function TestingRamón López PalopNo ratings yet
- Anatomy of The KidneyDocument5 pagesAnatomy of The Kidneycatherine kate gulengNo ratings yet
- Physical Assessment ChecklistDocument4 pagesPhysical Assessment ChecklistShades ofyellowNo ratings yet
- Heart Block Vein Opening Natural RemedyDocument20 pagesHeart Block Vein Opening Natural Remedysheku_1990No ratings yet
- Wilcox's Surgical Anatomy of The Heart 4th Ed (PDF) (Tahir99) VRG PDFDocument391 pagesWilcox's Surgical Anatomy of The Heart 4th Ed (PDF) (Tahir99) VRG PDFTatiana Decuseară100% (10)
- Cardiac Troponin I Leve in STEMI and Clinical Correlation With LeftVentricular Dysfunction in Indian Population 2329 9517.1000116Document6 pagesCardiac Troponin I Leve in STEMI and Clinical Correlation With LeftVentricular Dysfunction in Indian Population 2329 9517.1000116panjiNo ratings yet
- Case Reports AbstractsDocument7 pagesCase Reports AbstractsNovie AstiniNo ratings yet
- Science: Quarter 1 - Module 1: Respiratory and Circulatory Systems, Working With Other Organ SystemsDocument27 pagesScience: Quarter 1 - Module 1: Respiratory and Circulatory Systems, Working With Other Organ SystemsSofia Rose Saniel Gonzales100% (1)
- The Circulatory System PDFDocument4 pagesThe Circulatory System PDFPerry SinNo ratings yet
- Edema and FarctionDocument45 pagesEdema and FarctionGokulapriya.KNo ratings yet
- 4th Universal Definition of Myocardial Infarction 2018Document34 pages4th Universal Definition of Myocardial Infarction 2018Luis Carlos OstolazaNo ratings yet
- Anesthesia Consideration For Cranipharyngioma Resection in Pediatric PatientDocument5 pagesAnesthesia Consideration For Cranipharyngioma Resection in Pediatric PatientpitriaNo ratings yet
- AtherosclerosisDocument9 pagesAtherosclerosisBixuan ChiaNo ratings yet
- Transportation in Animals and Plants Worksheet 10 PDFDocument2 pagesTransportation in Animals and Plants Worksheet 10 PDFParul ShahNo ratings yet
- HypertensionDocument26 pagesHypertensionAbdalrhman Zaqqa100% (1)
- Case Study of 53-Year-Old Male with Hypertension and Coronary Artery DiseaseDocument6 pagesCase Study of 53-Year-Old Male with Hypertension and Coronary Artery DiseaseApoorv Jain100% (1)
- Chapter 4 - Mixed Venous Oxygen SaturationDocument3 pagesChapter 4 - Mixed Venous Oxygen SaturationJamesNo ratings yet
- Blood Vessels, AnatomyDocument20 pagesBlood Vessels, AnatomyAbu BakarNo ratings yet
- Pelvic Lymphadenectomy Step-By-Step Surgical EducaDocument5 pagesPelvic Lymphadenectomy Step-By-Step Surgical EducaVlad GrigoreNo ratings yet
- Angina Types and TreatmentDocument44 pagesAngina Types and TreatmentsimonjosanNo ratings yet
- 6 The Jejunum and The Ileum DiyaDocument24 pages6 The Jejunum and The Ileum DiyaEsosa OdighizuwaNo ratings yet
- Edema: Dr. Bernardo Dámaso MataDocument55 pagesEdema: Dr. Bernardo Dámaso MataDeivis Dan ErickNo ratings yet
- Terapi Oksigen Terhadap Perubahan Saturasi Oksigen Melalui Pemeriksaan Oksimetri Pada Pasien Infark Miokard Akut (Ima)Document6 pagesTerapi Oksigen Terhadap Perubahan Saturasi Oksigen Melalui Pemeriksaan Oksimetri Pada Pasien Infark Miokard Akut (Ima)edi sambasNo ratings yet
- Circulatory Systemand Respiratory SystemDocument39 pagesCirculatory Systemand Respiratory SystemEbb Edel QuibodNo ratings yet
- Rigel Vital Signs Booklet UK PDFDocument44 pagesRigel Vital Signs Booklet UK PDFJJ MMNo ratings yet