You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 327 1426 8 PBDocument11 pages327 1426 8 PBMaymay DamayNo ratings yet
- Pastel Portfolio - by SlidesgoDocument45 pagesPastel Portfolio - by SlidesgoKhansa MutiaraHasnaNo ratings yet
- First Report of COVID-19 Reinfection in A Patient With Beta Thalassemia MajorDocument5 pagesFirst Report of COVID-19 Reinfection in A Patient With Beta Thalassemia MajorwidyamsNo ratings yet
- Curriculum VitaeDocument1 pageCurriculum VitaewidyamsNo ratings yet
- 1 SM PDFDocument7 pages1 SM PDFNofri antsNo ratings yet
- Ruang/Waktu Hari/Tanggal Minggu Ruang Waktu Kamis I 1 PoliDocument4 pagesRuang/Waktu Hari/Tanggal Minggu Ruang Waktu Kamis I 1 PoliwidyamsNo ratings yet
- Management of Pregnancy With Eisenmenger Syndrome: AnesthesiaDocument12 pagesManagement of Pregnancy With Eisenmenger Syndrome: AnesthesiawidyamsNo ratings yet
- First Report of COVID-19 Reinfection in A Patient With Beta Thalassemia MajorDocument5 pagesFirst Report of COVID-19 Reinfection in A Patient With Beta Thalassemia MajorwidyamsNo ratings yet
- First Report of COVID-19 Reinfection in A Patient With Beta Thalassemia MajorDocument5 pagesFirst Report of COVID-19 Reinfection in A Patient With Beta Thalassemia MajorwidyamsNo ratings yet
- 3375 7036 1 SM PDFDocument7 pages3375 7036 1 SM PDFBruno MarsNo ratings yet
- IDR 71505 The Effect of A Unique Propolis Compund Propoelix TM On CL - 120914Document7 pagesIDR 71505 The Effect of A Unique Propolis Compund Propoelix TM On CL - 120914widyamsNo ratings yet
- Siva 2016Document5 pagesSiva 2016widyamsNo ratings yet
- Hipernatremia Dan Penatalaksanaanya: Yuswanto SetyawanDocument7 pagesHipernatremia Dan Penatalaksanaanya: Yuswanto SetyawanlalaNo ratings yet
- Peer Review Part23Document2 pagesPeer Review Part23widyamsNo ratings yet
- Ankle Brachial 1Document6 pagesAnkle Brachial 1titissetiarNo ratings yet
- Original Article Oral Health-Related Quality of Life in Children in Chile Treated For Cleft Lip and Palate: A Case-Control ApproachDocument7 pagesOriginal Article Oral Health-Related Quality of Life in Children in Chile Treated For Cleft Lip and Palate: A Case-Control ApproachwidyamsNo ratings yet
- Penatalaksanaan Ketoasidosis Diabetik (Kad)Document13 pagesPenatalaksanaan Ketoasidosis Diabetik (Kad)Emir AfifNo ratings yet
- k9 - Male Sexual DysfunctionDocument37 pagesk9 - Male Sexual DysfunctionwidyamsNo ratings yet
- (K8) Abnormality PDFDocument22 pages(K8) Abnormality PDFwidyamsNo ratings yet
- K6 RiskDocument26 pagesK6 RiskNilamAnggrianiTambunanNo ratings yet
- Prevalence of Anemia Among Adolescent Girls in A Rural Are ADocument12 pagesPrevalence of Anemia Among Adolescent Girls in A Rural Are AwidyamsNo ratings yet
- Pi Is 0901502717303168Document2 pagesPi Is 0901502717303168widyamsNo ratings yet
- 000000000000000000000000Document30 pages000000000000000000000000Isnaini ZNo ratings yet
- Gimul 17Document10 pagesGimul 17widyamsNo ratings yet
- CVC Removal Non Tunneled FINAL Jun 172012Document5 pagesCVC Removal Non Tunneled FINAL Jun 172012widyamsNo ratings yet
- 3852 e (C) F (T) PF (V) Pfa (A) PDocument6 pages3852 e (C) F (T) PF (V) Pfa (A) PwidyamsNo ratings yet
- Prevalence of Anemia Among Adolescent Girls in A Rural Are ADocument12 pagesPrevalence of Anemia Among Adolescent Girls in A Rural Are AwidyamsNo ratings yet
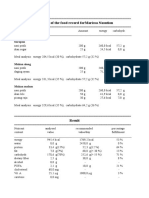
- Analysis of The Food Record Formargaret Simamora: SarapanDocument2 pagesAnalysis of The Food Record Formargaret Simamora: SarapanwidyamsNo ratings yet
- Analysis of The Food Record Fornina Amelia: SarapanDocument2 pagesAnalysis of The Food Record Fornina Amelia: SarapanwidyamsNo ratings yet
- Analysis of The Food Record Formarissa Nasution: SarapanDocument2 pagesAnalysis of The Food Record Formarissa Nasution: SarapanwidyamsNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Paper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockDocument11 pagesPaper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockTheresia AvilaNo ratings yet
- 10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)Document45 pages10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)MUHAMMAD BAGIR ALJUFRINo ratings yet
- Fluoroquinolones Full ListDocument2 pagesFluoroquinolones Full ListAvelox FloxNo ratings yet
- Fluids and Electrlytes 1Document14 pagesFluids and Electrlytes 1Pau-pau BasiNo ratings yet
- Jurnal Gastritis PDFDocument6 pagesJurnal Gastritis PDFSholeh Hasan87No ratings yet
- Naval Special Warfare Physical Training GuideDocument17 pagesNaval Special Warfare Physical Training GuideAnonymous k6Qd0sNo ratings yet
- s13014 015 0495 4Document6 pagess13014 015 0495 4produxing 101No ratings yet
- A-PULMO - (LEE-TAN-CONSTANTINO) - Prelims (TD) B - Pulmo - (Lee-Tan-Constantino) - PrelimsDocument17 pagesA-PULMO - (LEE-TAN-CONSTANTINO) - Prelims (TD) B - Pulmo - (Lee-Tan-Constantino) - PrelimsJohn Paulo CatacutanNo ratings yet
- ACTCDocument2 pagesACTCVenkat RavichandranNo ratings yet
- Bunion Symptom DisorderDocument5 pagesBunion Symptom DisorderNina KotNo ratings yet
- Macromolecule LabDocument7 pagesMacromolecule Labapi-318665838No ratings yet
- Trauma BuliDocument32 pagesTrauma BulimoonlightsoantaNo ratings yet
- The Manchurian ApproachDocument2 pagesThe Manchurian ApproachArtist Metu20% (5)
- What Is A PET Scan?: Purpose PET Scan vs. Other Tests Risks Preparation Procedure Follow-Up and ResultsDocument13 pagesWhat Is A PET Scan?: Purpose PET Scan vs. Other Tests Risks Preparation Procedure Follow-Up and Resultsmehtab sanaNo ratings yet
- 331-Book Chapter-3614-2-10-20210406Document20 pages331-Book Chapter-3614-2-10-20210406Yolla GitamayaNo ratings yet
- Pink Puffer Blue BloaterDocument10 pagesPink Puffer Blue BloaterMelinda MarianniNo ratings yet
- Jadwal PIT 2018Document11 pagesJadwal PIT 2018Noven Afiyata NugrahaNo ratings yet
- Beetroot 2 PDFDocument4 pagesBeetroot 2 PDFNatasya PermataNo ratings yet
- Bloodborne Pathogens TrainingDocument102 pagesBloodborne Pathogens Trainingapi-311432115No ratings yet
- Scabies Jurnal PDFDocument6 pagesScabies Jurnal PDFImam Hakim SuryonoNo ratings yet
- Family CounsellingDocument10 pagesFamily Counsellingindians risingNo ratings yet
- Aplastic Anemia Pa Tho PhysiologyDocument3 pagesAplastic Anemia Pa Tho Physiologyneil052275% (4)
- Tooth-Supported Overdentures 2 PDFDocument7 pagesTooth-Supported Overdentures 2 PDFKrupali JainNo ratings yet
- Project CharterDocument2 pagesProject CharterMatt MelvinNo ratings yet
- NCP Acute AppendicitisDocument2 pagesNCP Acute AppendicitisJane Arian Berzabal100% (1)
- Welfare AID BrochureDocument2 pagesWelfare AID BrochureWasfa Farooq BadshahNo ratings yet
- Freud and FreudianDocument20 pagesFreud and FreudianSherwan R ShalNo ratings yet
- LESSON PLAN Shwe Final PmsDocument14 pagesLESSON PLAN Shwe Final PmsSanthu Su100% (1)
- Down SyndromeDocument18 pagesDown Syndromepreciouslacdan86% (7)
- Graves DiseaseDocument2 pagesGraves Diseaseجـــروح الهــوىNo ratings yet