You might also like
- Chapter 6 Strategy Analysis and Choice: Strategic Management: A Competitive Advantage Approach, 16e (David)Document27 pagesChapter 6 Strategy Analysis and Choice: Strategic Management: A Competitive Advantage Approach, 16e (David)Masum ZamanNo ratings yet
- Nicu Must KnowsDocument7 pagesNicu Must KnowsCyfern100% (2)
- VSIM Jackson Weber DocumentationDocument2 pagesVSIM Jackson Weber DocumentationJacqueline LamNo ratings yet
- Sample Strong Eras Lor 5-05Document1 pageSample Strong Eras Lor 5-05Raiyan KhanNo ratings yet
- Shelly Cashman Series Microsoft Office 365 Excel 2016 Comprehensive 1st Edition Freund Solutions ManualDocument5 pagesShelly Cashman Series Microsoft Office 365 Excel 2016 Comprehensive 1st Edition Freund Solutions Manualjuanlucerofdqegwntai100% (10)
- MCN Midterm Review QuestionsDocument6 pagesMCN Midterm Review QuestionsJenny VillanuevaNo ratings yet
- MCN II PostpartumDocument16 pagesMCN II PostpartumJharaNo ratings yet
- The Limits of The Sectarian Narrative in YemenDocument19 pagesThe Limits of The Sectarian Narrative in Yemenهادي قبيسيNo ratings yet
- Literature Review - Part Time Job Among StudentDocument3 pagesLiterature Review - Part Time Job Among StudentMarria65% (20)
- Management of Gastroschisis Using Standard Urobag As Silo: Case ReportDocument4 pagesManagement of Gastroschisis Using Standard Urobag As Silo: Case ReportdokterdonnyNo ratings yet
- Case Report: Intestinal Obstruction in A Child With Massive AscariasisDocument4 pagesCase Report: Intestinal Obstruction in A Child With Massive AscariasisWella Vista EdwardNo ratings yet
- Malnutrition and Hypernatraemia in Breastfed Babies: Annals of Tropical PaediatricsDocument6 pagesMalnutrition and Hypernatraemia in Breastfed Babies: Annals of Tropical PaediatricsUlliaNo ratings yet
- Makalahkoheri 10:7:19Document18 pagesMakalahkoheri 10:7:19PutuIantaParamaSiwiNo ratings yet
- Case Study: GeneralDocument39 pagesCase Study: GeneralrdNo ratings yet
- Mosby's Pedia Nclex@CnDocument63 pagesMosby's Pedia Nclex@Cnsushilpradeep500No ratings yet
- Metode Kangguru BBLRDocument5 pagesMetode Kangguru BBLRdiana seviaNo ratings yet
- MCHN Reviewer 80 ItemsDocument6 pagesMCHN Reviewer 80 ItemsChristine UdhayNo ratings yet
- Group 1b Case Presentation NRMFDocument57 pagesGroup 1b Case Presentation NRMFElesis samaNo ratings yet
- Nursing ProcessDocument3 pagesNursing ProcessKrishelle Kate PannigNo ratings yet
- G1 Script Flow For Duty CHN RLEDocument3 pagesG1 Script Flow For Duty CHN RLELouwella RamosNo ratings yet
- This Study Resource WasDocument1 pageThis Study Resource WasMelinda Cariño BallonNo ratings yet
- Mosbys Child Health Nursing 1Document62 pagesMosbys Child Health Nursing 1Darren VargasNo ratings yet
- RLE RequirementDocument5 pagesRLE RequirementSvetlana DiazNo ratings yet
- MCN II NewbornDocument14 pagesMCN II NewbornJharaNo ratings yet
- Review Questionnaire MTRNALDocument13 pagesReview Questionnaire MTRNALKevin Vincent AquinoNo ratings yet
- Iajt 05 I 4 P 155Document1 pageIajt 05 I 4 P 155api-3702148No ratings yet
- Pedia Old eDocument11 pagesPedia Old eDivynne MadeloNo ratings yet
- Association of Etonogestrel-Releasing Contraceptive Implant With Reduced Weight Gain in An Exclusively Breastfed Infant: Report and Literature ReviewDocument4 pagesAssociation of Etonogestrel-Releasing Contraceptive Implant With Reduced Weight Gain in An Exclusively Breastfed Infant: Report and Literature ReviewFian FebriantoNo ratings yet
- Cow's Milk Allergy ManagementDocument17 pagesCow's Milk Allergy ManagementHensen ChenNo ratings yet
- UntitledDocument9 pagesUntitledPurilarp Dao-aroonkietNo ratings yet
- PNC PresentationDocument42 pagesPNC PresentationRijoy ZuzadNo ratings yet
- 07 Nursing Role in The Health of Ill Children and Their FamiliesDocument20 pages07 Nursing Role in The Health of Ill Children and Their FamiliesJAN CAMILLE LENONNo ratings yet
- Cilios Com Ptirus PubisDocument4 pagesCilios Com Ptirus PubisRafael CedroNo ratings yet
- MRCPCH Part Ii: Safdar Iqbal'sDocument5 pagesMRCPCH Part Ii: Safdar Iqbal'sGalaleldin AliNo ratings yet
- Weekly Plan of Care 2019Document3 pagesWeekly Plan of Care 2019LoraNo ratings yet
- UntitledDocument1 pageUntitledIvan VillapandoNo ratings yet
- Article ContentDocument11 pagesArticle ContentAli FalihNo ratings yet
- Sample Case StudyDocument38 pagesSample Case Studyanon-387573100% (3)
- Critical Apraisal Metode KanguruDocument5 pagesCritical Apraisal Metode KanguruMeilani ManuNo ratings yet
- Take One Mockbaords NP 1 5Document48 pagesTake One Mockbaords NP 1 5marlon armamento100% (1)
- After 2 Hours of Nursing Intervention, The Mother Will Verbalized The Understanding of The Condition, Process, and TreatmentDocument3 pagesAfter 2 Hours of Nursing Intervention, The Mother Will Verbalized The Understanding of The Condition, Process, and TreatmentJelly Yanquiling DumlaoNo ratings yet
- Emotional Support in The Immediate Post Partum 1. Taking PhaseDocument3 pagesEmotional Support in The Immediate Post Partum 1. Taking PhaseApRil Anne BalanonNo ratings yet
- Gordon'S 11 Functional Health Patterns Functional Health Pattern Before Hospitalization During Hospitalization Health Perception-Health ManagementDocument6 pagesGordon'S 11 Functional Health Patterns Functional Health Pattern Before Hospitalization During Hospitalization Health Perception-Health ManagementLadybelle GototosNo ratings yet
- Nursing KardexDocument1 pageNursing KardexLouie Siazon VasquezNo ratings yet
- Ob Journal 2Document3 pagesOb Journal 2api-662323379No ratings yet
- Comparison of Radiant Warmer Care and Kangaroo MotDocument3 pagesComparison of Radiant Warmer Care and Kangaroo Motkurniawati0% (1)
- Intestinal Malrotation in Neonates With Nonbilious Emesis: Perinatal/Neonatal Case PresentationDocument3 pagesIntestinal Malrotation in Neonates With Nonbilious Emesis: Perinatal/Neonatal Case PresentationSaurav SultaniaNo ratings yet
- L-Reuteri in Infantile ColicDocument9 pagesL-Reuteri in Infantile ColicFrancesco SassiNo ratings yet
- Zinc Supplementation in Preterm Neonates and Neurological Development: A Randomized Controlled TrialDocument5 pagesZinc Supplementation in Preterm Neonates and Neurological Development: A Randomized Controlled TrialjanakaNo ratings yet
- OseiDocument74 pagesOseiPrilla AgyenNo ratings yet
- Which of The fo-WPS OfficeDocument3 pagesWhich of The fo-WPS OfficeLala MumuNo ratings yet
- Case Scenerio MENINGITISDocument10 pagesCase Scenerio MENINGITISEllen AngelNo ratings yet
- Fistula in Ano Final For PresentationDocument41 pagesFistula in Ano Final For PresentationRhajeeb Aennas SugalaNo ratings yet
- En MB Sukma 11 Dec 18 13.10Document35 pagesEn MB Sukma 11 Dec 18 13.10Handoyo KooNo ratings yet
- Makalah Ce Carissa - 18.08.2020 PK 18.26Document75 pagesMakalah Ce Carissa - 18.08.2020 PK 18.26sumbiaindrianiNo ratings yet
- Price Douglas2007Document6 pagesPrice Douglas2007azhar naufaldiNo ratings yet
- School of Health and Natural Sciences Nursing DepartmentDocument52 pagesSchool of Health and Natural Sciences Nursing DepartmentJosephine Mae TumanutNo ratings yet
- Intended Learning OutcomeDocument1 pageIntended Learning OutcomeJade CentinoNo ratings yet
- Journal of Human Lactation: Fentanyl Transdermal Analgesia During Pregnancy and LactationDocument4 pagesJournal of Human Lactation: Fentanyl Transdermal Analgesia During Pregnancy and Lactationcaturpw7No ratings yet
- Cogasa Gordon'sDocument3 pagesCogasa Gordon'sJasmine BesaNo ratings yet
- Extremely Low Birth Weight Babies: Report of Two Cases)Document3 pagesExtremely Low Birth Weight Babies: Report of Two Cases)yasintameganabilaNo ratings yet
- Ca Skin To SkinDocument9 pagesCa Skin To SkinSusi HersaptitiNo ratings yet
- Steps To Successfully Breastfeed The Premature InfantDocument10 pagesSteps To Successfully Breastfeed The Premature InfantKholis FaisolNo ratings yet
- MATERNAL and CHILD SUMMARY Chapters 26 - 29 (Adelle Pillitteri)Document87 pagesMATERNAL and CHILD SUMMARY Chapters 26 - 29 (Adelle Pillitteri)CHRISTIE MONTANO100% (8)
- Newborn Antibiotic Guide or Early and Late Onset Sepsis During Birth Episode of Care Revised June 2018Document14 pagesNewborn Antibiotic Guide or Early and Late Onset Sepsis During Birth Episode of Care Revised June 2018Raiyan KhanNo ratings yet
- Denosumab in MyelomaDocument5 pagesDenosumab in MyelomaRaiyan KhanNo ratings yet
- Prepare For Blood Donation Flyer A4Document1 pagePrepare For Blood Donation Flyer A4Raiyan KhanNo ratings yet
- Health Pra CRN at LawDocument313 pagesHealth Pra CRN at LawRaiyan KhanNo ratings yet
- Notification Form NOTF 00Document10 pagesNotification Form NOTF 00Raiyan KhanNo ratings yet
- Clin Infect Dis. 2002 Thomas 46 52Document7 pagesClin Infect Dis. 2002 Thomas 46 52Raiyan KhanNo ratings yet
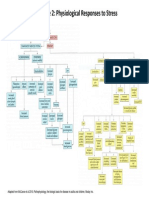
- Figure 2: Physiological Responses To StressDocument1 pageFigure 2: Physiological Responses To StressRaiyan KhanNo ratings yet
- LicenseDocument3 pagesLicenseSourav SharmaNo ratings yet
- Code of Practice For Design Loads (Other Than Earthquake) For Buildings and StructuresDocument39 pagesCode of Practice For Design Loads (Other Than Earthquake) For Buildings and StructuresIshor ThapaNo ratings yet
- ANTINEOPLASTICSDocument21 pagesANTINEOPLASTICSGunjan KalyaniNo ratings yet
- Reinforced Concrete Design PDFDocument1 pageReinforced Concrete Design PDFhallelNo ratings yet
- Chudamani Women Expecting ChangeDocument55 pagesChudamani Women Expecting ChangeMr AnantNo ratings yet
- AVEVA LFM - Data Summary v2Document6 pagesAVEVA LFM - Data Summary v2Joshua HobsonNo ratings yet
- Chapter 9Document28 pagesChapter 9Aniket BatraNo ratings yet
- AIP 2020 FINAL JuneDocument5 pagesAIP 2020 FINAL JuneVINA ARIETANo ratings yet
- QF Jacket (Drafting & Cutting) - GAR620Document15 pagesQF Jacket (Drafting & Cutting) - GAR620abdulraheem18822No ratings yet
- Furniture AnnexDocument6 pagesFurniture AnnexAlaa HusseinNo ratings yet
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentAditya ShanbhagNo ratings yet
- Volcanoes Sub-topic:Volcanic EruptionDocument16 pagesVolcanoes Sub-topic:Volcanic EruptionVhenz MapiliNo ratings yet
- GR 9 Eng CodebDocument6 pagesGR 9 Eng CodebSharmista WalterNo ratings yet
- MCFKTP G3 S2 SC Number Pattern PuzzlesDocument5 pagesMCFKTP G3 S2 SC Number Pattern PuzzlesEric GoNo ratings yet
- Week 1 Familiarize The VmgoDocument10 pagesWeek 1 Familiarize The VmgoHizzel De CastroNo ratings yet
- Final Lesson PlanDocument3 pagesFinal Lesson Planapi-510713019No ratings yet
- 3E Hand Over NotesDocument3 pages3E Hand Over NotesAshutosh MaiidNo ratings yet
- Zillah P. Curato: ObjectiveDocument1 pageZillah P. Curato: ObjectiveZillah CuratoNo ratings yet
- Oracle SOA Suite Oracle Containers For J2EE Feature Overview OC4JDocument10 pagesOracle SOA Suite Oracle Containers For J2EE Feature Overview OC4JLuis YañezNo ratings yet
- Antenatal Care (ANC)Document77 pagesAntenatal Care (ANC)tareNo ratings yet
- When SIBO & IBS-Constipation Are Just Unrecognized Thiamine DeficiencyDocument3 pagesWhen SIBO & IBS-Constipation Are Just Unrecognized Thiamine Deficiencyps piasNo ratings yet
- S3 U4 MiniTestDocument3 pagesS3 U4 MiniTestĐinh Thị Thu HàNo ratings yet
- General Return Service Agreement (RSA) GuidelinesDocument2 pagesGeneral Return Service Agreement (RSA) GuidelinesJune Francis AngNo ratings yet
- ASTR 323 Homework 4Document2 pagesASTR 323 Homework 4Andrew IvanovNo ratings yet
- Derivation Bragg's Snell Law PDFDocument4 pagesDerivation Bragg's Snell Law PDFVaswati BiswasNo ratings yet
- World BankDocument28 pagesWorld BankFiora FarnazNo ratings yet
- Embedded Software Development ProcessDocument34 pagesEmbedded Software Development ProcessAmmar YounasNo ratings yet