You might also like
- Proforma For Calculation of Income Tax For Tax DeductionDocument1 pageProforma For Calculation of Income Tax For Tax DeductionManchala Devika100% (1)
- PPCSGO-HRD-006 (Revised QAME Analysis Form 1)Document4 pagesPPCSGO-HRD-006 (Revised QAME Analysis Form 1)PERCIVAL DE GUZMAN100% (1)
- Weekly Home Learning PlanDocument12 pagesWeekly Home Learning Planjonalyn100% (2)
- David Vs ArroyoDocument2 pagesDavid Vs ArroyoAjpadateNo ratings yet
- Empowerment 2Document39 pagesEmpowerment 2Lee Oh100% (2)
- IELTS Academic Writing: How To Write 8+ Answers For The IELTS Exam!From EverandIELTS Academic Writing: How To Write 8+ Answers For The IELTS Exam!Rating: 4.5 out of 5 stars4.5/5 (6)
- Northlink: Activity Approval Form For Clubs ActivityDocument2 pagesNorthlink: Activity Approval Form For Clubs ActivityRaf Belz100% (1)
- Proposal TemplateDocument6 pagesProposal TemplateArt Veloso Mangubat100% (1)
- Activity Completion Report Template For TRAINING PROPONENTSDocument6 pagesActivity Completion Report Template For TRAINING PROPONENTSSLNHSNo ratings yet
- Weekly Home Learning Plan For Grade 7 Week 3Document3 pagesWeekly Home Learning Plan For Grade 7 Week 3reiya100% (4)
- ALS RPL Form 2 Training RecordDocument2 pagesALS RPL Form 2 Training RecordHoney Grace Buyan100% (1)
- Monitoring, Evaluating, and Improving: An Evidence-Based Approach to Achieving Development Results that Matter!From EverandMonitoring, Evaluating, and Improving: An Evidence-Based Approach to Achieving Development Results that Matter!No ratings yet
- Ok Sa Deped Accomplishment ReportDocument15 pagesOk Sa Deped Accomplishment ReportAnonymous YhZlC5AmNo ratings yet
- Check Condition of Tools and EquipmentDocument18 pagesCheck Condition of Tools and EquipmentApril AbengozaNo ratings yet
- Constitutional Law II Digest on Poe vs. Comelec and TatadDocument49 pagesConstitutional Law II Digest on Poe vs. Comelec and TatadMica Joy FajardoNo ratings yet
- Re-Entry Action Plan (Reap) and Implemetation Report: Dep Artment of EducationDocument3 pagesRe-Entry Action Plan (Reap) and Implemetation Report: Dep Artment of EducationAbegail H. Laquiao100% (3)
- Computer Lab ProposalDocument1 pageComputer Lab ProposalApril Abengoza100% (1)
- Chapter 02 - CONCEPTUAL FRAMEWORK: Objective of Financial ReportingDocument6 pagesChapter 02 - CONCEPTUAL FRAMEWORK: Objective of Financial ReportingKimberly Claire AtienzaNo ratings yet
- ALS Cluster 4 Monthly CalendarDocument7 pagesALS Cluster 4 Monthly CalendarKristine Banda-Rosas CanalesNo ratings yet
- Form A Health ReportDocument2 pagesForm A Health ReportSer IC93% (30)
- Letter of Motivation (Financial Services Management)Document1 pageLetter of Motivation (Financial Services Management)Tanzeel Ur Rahman100% (5)
- NEAP QAME Analysis Forms 1 2 3Document15 pagesNEAP QAME Analysis Forms 1 2 3Clarissa Soliven0% (1)
- Ok Sa Deped Form CDocument4 pagesOk Sa Deped Form CMeera Joy Deboma BlancoNo ratings yet
- Subject Improvement Plan For 2022.Document2 pagesSubject Improvement Plan For 2022.Zinhle83% (6)
- FM-SGO-HRD-006 (Revised QAME Analysis Form 1)Document4 pagesFM-SGO-HRD-006 (Revised QAME Analysis Form 1)Ronel M. BuidNo ratings yet
- Oplan Kalusugan Sa Deped Form ADocument2 pagesOplan Kalusugan Sa Deped Form AGlory Jane Pequiño CodillaNo ratings yet
- Ok Sa Deped Form ADocument3 pagesOk Sa Deped Form APhoebe Sudweste Quitaneg100% (1)
- Ok Sa Deped Form ADocument3 pagesOk Sa Deped Form AJewela AlbaoNo ratings yet
- DepEd Health Form Progress ReportDocument4 pagesDepEd Health Form Progress ReportAirene Mariel MagbanuaNo ratings yet
- Okd Form ADocument15 pagesOkd Form ARollyNo ratings yet
- Revised OK Sa DepEd Forms 2019 1Document16 pagesRevised OK Sa DepEd Forms 2019 1Marison GerantaNo ratings yet
- Okd Form ADocument22 pagesOkd Form AJoan DalilisNo ratings yet
- DO s2018 028-Converted-1Document29 pagesDO s2018 028-Converted-1Jenie Viva AndradeNo ratings yet
- Progress Report FormDocument2 pagesProgress Report FormJonathan CostiboloNo ratings yet
- Revised OK Sa DepEd Forms 2019Document16 pagesRevised OK Sa DepEd Forms 2019Annielou OliveraNo ratings yet
- OPLAN KALUSUGAN SA DEPED FORM A EdtedDocument2 pagesOPLAN KALUSUGAN SA DEPED FORM A EdtedTine Cristine100% (1)
- Ok Sa Deped Form ADocument3 pagesOk Sa Deped Form AMay John Delos SantosNo ratings yet
- DO s2018 028Document29 pagesDO s2018 028erikabeltran100% (1)
- Progress Report: Plan Alusugan Sa DepedDocument3 pagesProgress Report: Plan Alusugan Sa DepedRosalie Dela CruzNo ratings yet
- Daily Training Evaluation SummaryDocument4 pagesDaily Training Evaluation Summarycristina maquintoNo ratings yet
- BSBSUS401 - Student Assessment v2.2Document10 pagesBSBSUS401 - Student Assessment v2.2yukio misimaNo ratings yet
- 16 LD Acomplishment ReportDocument2 pages16 LD Acomplishment ReportAlma ZaraNo ratings yet
- Ok Sa Deped Form CDocument4 pagesOk Sa Deped Form CJanus SalinasNo ratings yet
- Division Memo. No. 098, S. 2021Document19 pagesDivision Memo. No. 098, S. 2021Gregson GucelaNo ratings yet
- Brigada EskwelaDocument11 pagesBrigada EskwelaErich David GarciaNo ratings yet
- Subject_Improvement_Plan_for_2022 (Blank)Document2 pagesSubject_Improvement_Plan_for_2022 (Blank)nhloeh.sotobeNo ratings yet
- RC-HRD-FR-016-QAME-Form-2-Summary-of-Daily-MEDocument4 pagesRC-HRD-FR-016-QAME-Form-2-Summary-of-Daily-METiffanyKateJuanLintaoNo ratings yet
- TCCES LAC Tools and TemplatesDocument19 pagesTCCES LAC Tools and TemplatesEdgar Amisola FernandezNo ratings yet
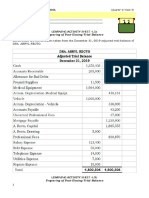
- LEARNING ACTIVITY SHEET 4.5aDocument2 pagesLEARNING ACTIVITY SHEET 4.5aMelu Jean MayoresNo ratings yet
- FORM 3C Research and Extension FunctionsDocument2 pagesFORM 3C Research and Extension Functionscil dacaymatNo ratings yet
- FM-SGO-HRD-008 (L - D Completion Report) INSETDocument4 pagesFM-SGO-HRD-008 (L - D Completion Report) INSETRenge TañaNo ratings yet
- SHS TVL MEMO Enclosures-2Document10 pagesSHS TVL MEMO Enclosures-2LYDIANo ratings yet
- PARTS of OJT Narrative ReportDocument6 pagesPARTS of OJT Narrative ReportPatricia Anne CorpuzNo ratings yet
- Strengthening Tuberculosis and HIV&AIDS Responses in East Central Uganda (STAR-EC)Document5 pagesStrengthening Tuberculosis and HIV&AIDS Responses in East Central Uganda (STAR-EC)Francis BukenyaNo ratings yet
- Attachment 1Document3 pagesAttachment 1John NjihiaNo ratings yet
- Qad Form 006 Government Renewal Permit GRP Processing Checklist New TemplateDocument3 pagesQad Form 006 Government Renewal Permit GRP Processing Checklist New TemplateJenevic LatorsaNo ratings yet
- Monitoring and Evaluation Tools To Sci Activity With FamilyDocument5 pagesMonitoring and Evaluation Tools To Sci Activity With FamilySuzette VillonNo ratings yet
- Private School Monitoring ReportDocument4 pagesPrivate School Monitoring ReportNer MangaronNo ratings yet
- School LRCPDocument14 pagesSchool LRCPSheina AnocNo ratings yet
- Hospital Staff Accomplishment ReportsDocument19 pagesHospital Staff Accomplishment ReportsMild BallezaNo ratings yet
- 24 Jan Inset Ipcr Monitoring Tool On SchoolsDocument2 pages24 Jan Inset Ipcr Monitoring Tool On SchoolsShajara Del Rosario-TablasonNo ratings yet
- Project Proposal: Schools Division of Sorsogon Cocok-Cabitan Elementary SchoolDocument4 pagesProject Proposal: Schools Division of Sorsogon Cocok-Cabitan Elementary SchoolJessa BurgosNo ratings yet
- EFLFDocument1 pageEFLFFryzchie May Alesna BatoonNo ratings yet
- Ptep Goals-AlgDocument4 pagesPtep Goals-Algapi-316781445No ratings yet
- SDO CamSur INSET - Activity Completion ReportDocument4 pagesSDO CamSur INSET - Activity Completion ReportKielah RequeNo ratings yet
- IEP Template for Transition PlanningDocument11 pagesIEP Template for Transition PlanningIshaMahajanNo ratings yet
- CAMANGAAN EAST ES OK-sa-DepEd-Form-ADocument3 pagesCAMANGAAN EAST ES OK-sa-DepEd-Form-AKristine Lacbayan CastroNo ratings yet
- Progress Utilization NEW FinalDocument3 pagesProgress Utilization NEW FinalMaheen IqbalNo ratings yet
- MEPA mONITORING TEMPLATEDocument9 pagesMEPA mONITORING TEMPLATENASSER ABDULNo ratings yet
- Introduction to Statistics Through Resampling Methods and RFrom EverandIntroduction to Statistics Through Resampling Methods and RNo ratings yet
- Drafting Elevations and SectionsDocument11 pagesDrafting Elevations and SectionsApril AbengozaNo ratings yet
- Findings and DiscussionDocument5 pagesFindings and DiscussionApril AbengozaNo ratings yet
- Mr. and Mrs. Kalix Martinez Mr. and Mrs. Akihiro Juarez Airasia Corp. Mr. and Mrs. Sebastian Camero Camero Mr. and Mrs. Clyden Ramirez St. Peter HDocument1 pageMr. and Mrs. Kalix Martinez Mr. and Mrs. Akihiro Juarez Airasia Corp. Mr. and Mrs. Sebastian Camero Camero Mr. and Mrs. Clyden Ramirez St. Peter HApril AbengozaNo ratings yet
- Industrial TechDocument1 pageIndustrial TechApril AbengozaNo ratings yet
- Summary of LessonDocument4 pagesSummary of LessonApril AbengozaNo ratings yet
- Kurtzman, 1984 Swanson, 1981Document1 pageKurtzman, 1984 Swanson, 1981April AbengozaNo ratings yet
- 1Document3 pages1April AbengozaNo ratings yet
- Methodology: RAND Corporation's (1973)Document1 pageMethodology: RAND Corporation's (1973)April AbengozaNo ratings yet
- MasterDocument1 pageMasterApril AbengozaNo ratings yet
- Empowerment Pre Final 2018-2019Document4 pagesEmpowerment Pre Final 2018-2019April AbengozaNo ratings yet
- Empowerment 4thDocument4 pagesEmpowerment 4thApril AbengozaNo ratings yet
- Left PDFDocument1 pageLeft PDFApril AbengozaNo ratings yet
- Computer Hardware Servicing CGDocument20 pagesComputer Hardware Servicing CGNobhe MeowNo ratings yet
- Example Case Study Activity #1Document1 pageExample Case Study Activity #1Kate MercadoNo ratings yet
- August 15, 2019: Vilma D. Eda, Ceso VDocument2 pagesAugust 15, 2019: Vilma D. Eda, Ceso VApril AbengozaNo ratings yet
- Book 1Document5 pagesBook 1April AbengozaNo ratings yet
- DO s2018 028Document29 pagesDO s2018 028erikabeltran100% (1)
- Teenproblems 131118101824 Phpapp01Document10 pagesTeenproblems 131118101824 Phpapp01April AbengozaNo ratings yet
- 24 Nov 1997 Male GEN: Communication Address GATE Exam DetailsDocument1 page24 Nov 1997 Male GEN: Communication Address GATE Exam DetailsAr Tanmaye MahajanNo ratings yet
- Nobody Does It Better and Indian Hospitality Will Leave You Feeling Better Too.Document2 pagesNobody Does It Better and Indian Hospitality Will Leave You Feeling Better Too.Abhijeet UmatheNo ratings yet
- Ethical Considerations: Why Is Ethics The Focus of A Lead Chapter in This Book?Document17 pagesEthical Considerations: Why Is Ethics The Focus of A Lead Chapter in This Book?ibrahim haniNo ratings yet
- Philippine History: Pre-Colonial PeriodDocument87 pagesPhilippine History: Pre-Colonial PeriodJames Brian Garcia GarayNo ratings yet
- Water Resources in TamilnaduDocument4 pagesWater Resources in TamilnaduVignesh AngelNo ratings yet
- HR GDDocument8 pagesHR GDNisheeth BeheraNo ratings yet
- Module 6 - Ministries of JesusDocument5 pagesModule 6 - Ministries of JesusIce James PachanoNo ratings yet
- 2022 Buncombe County Domestic Violence Fatality ReviewDocument10 pages2022 Buncombe County Domestic Violence Fatality ReviewChristian SmithNo ratings yet
- Essay 3Document2 pagesEssay 3Rinna Trisha V. QuilinoNo ratings yet
- Department of Education: Answer Sheet ProvidedDocument3 pagesDepartment of Education: Answer Sheet ProvidedFlomarie AlferezNo ratings yet
- Bernard Stiegler The Writing Screen 2015Document12 pagesBernard Stiegler The Writing Screen 2015madequal2658100% (1)
- CXYS Liability FormDocument1 pageCXYS Liability FormRandy NissenNo ratings yet
- United States v. Arthur Young & Co., 465 U.S. 805 (1984)Document15 pagesUnited States v. Arthur Young & Co., 465 U.S. 805 (1984)Scribd Government DocsNo ratings yet
- Ingeus Restart Scheme Participant Handbook Cwl-19july2021Document15 pagesIngeus Restart Scheme Participant Handbook Cwl-19july2021pp019136No ratings yet
- Irb Ar 2012-13Document148 pagesIrb Ar 2012-13Shikhin GargNo ratings yet
- Procedures For Connection of PV Plants To MEPSO Grid in North MacedoniaDocument17 pagesProcedures For Connection of PV Plants To MEPSO Grid in North MacedoniaAleksandar JordanovNo ratings yet
- Wedding ScriptDocument9 pagesWedding ScriptMyn Mirafuentes Sta AnaNo ratings yet
- So Ping Bun's Warehouse Occupancy DisputeDocument4 pagesSo Ping Bun's Warehouse Occupancy DisputeVincent BernardoNo ratings yet
- Unjust identification of Pushyamitra as a BrahminDocument6 pagesUnjust identification of Pushyamitra as a BrahminSHIVAM SINGHNo ratings yet
- 20th Batch F 101Document22 pages20th Batch F 101Mohammad helal uddin ChowdhuryNo ratings yet
- INDIAN WAR OF INDEPENDENCE 1857 - ORIGINAL PUBLISHERs NoteDocument19 pagesINDIAN WAR OF INDEPENDENCE 1857 - ORIGINAL PUBLISHERs NoteBISWAJIT MOHANTYNo ratings yet
- All 18 QSS in One-1 PDFDocument314 pagesAll 18 QSS in One-1 PDFkishan23100% (1)
- Example Infrastructure Outage Incident ReportDocument3 pagesExample Infrastructure Outage Incident ReportLunarNo ratings yet
- ICAR IARI 2021 Technician T1 Recruitment NotificationDocument38 pagesICAR IARI 2021 Technician T1 Recruitment NotificationJonee SainiNo ratings yet
- Undertaking Form For Shifters and TransfereesDocument1 pageUndertaking Form For Shifters and TransfereesAngela JingcoNo ratings yet