You might also like
- Understanding-Ocd 2016 v2Document27 pagesUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- Celiac DiseaseDocument36 pagesCeliac Diseaseapi-281575628100% (2)
- Pocket Reference For ECGs Made Easy 5th EditionDocument133 pagesPocket Reference For ECGs Made Easy 5th EditionSylvia Loong100% (2)
- Pfizer Inc.: United States Securities and Exchange CommissionDocument246 pagesPfizer Inc.: United States Securities and Exchange CommissionDipanshu NagarNo ratings yet
- Exercise 8 Pig Embryo (Posterior Sections)Document16 pagesExercise 8 Pig Embryo (Posterior Sections)Gail AmuraoNo ratings yet
- Anatomy 2021 FinalDocument2,156 pagesAnatomy 2021 Finalansh tyagiNo ratings yet
- Trauma Informed CareDocument8 pagesTrauma Informed CareJohn BitsasNo ratings yet
- Chest X - Ray InterpretationDocument147 pagesChest X - Ray InterpretationFcsieka FcseikaNo ratings yet
- Applied AnatomyDocument76 pagesApplied Anatomysantosh bhandariNo ratings yet
- IV Infusion: Purpose of Starting IV'sDocument6 pagesIV Infusion: Purpose of Starting IV'sKiara Denise TamayoNo ratings yet
- A Disease Study of Cushing's DiseaseDocument13 pagesA Disease Study of Cushing's DiseaseKristine AlejandroNo ratings yet
- Non Carious LesionsDocument18 pagesNon Carious LesionsAjmal NajeebNo ratings yet
- Chest X-Ray InterpretationDocument104 pagesChest X-Ray InterpretationIbra Geeky100% (1)
- Mung BeanDocument24 pagesMung BeanCaleb VoosNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayRizka RamadaniNo ratings yet
- Refresher Course: Preboard Examination Nursing Practice III: Care of Clients With Physiologic and Psychosocial Alterations (Part A)Document9 pagesRefresher Course: Preboard Examination Nursing Practice III: Care of Clients With Physiologic and Psychosocial Alterations (Part A)Jastine Sabornido0% (1)
- Varicose VeinsDocument37 pagesVaricose VeinsJavier SaadNo ratings yet
- OB - TransesDocument112 pagesOB - TransesAldwin BagtasNo ratings yet
- Guidelines For Laparoscopic (TAPP) and Endoscopic (TEP) Treatment of Inguinal Hernia Surg Endosc 2011Document71 pagesGuidelines For Laparoscopic (TAPP) and Endoscopic (TEP) Treatment of Inguinal Hernia Surg Endosc 2011John Kalaitzis100% (1)
- Medsurg 3 Exam 1Document55 pagesMedsurg 3 Exam 1Melissa Blanco100% (1)
- Atlas of Dialysis Vascular Access: Tushar J. Vachharajani, MD, FASN, FACPDocument75 pagesAtlas of Dialysis Vascular Access: Tushar J. Vachharajani, MD, FASN, FACPEileen del RosarioNo ratings yet
- AbdomenDocument83 pagesAbdomenprima suci angrainiNo ratings yet
- Veins: Anatomy Department, School of Medicine, Wuhan UniversityDocument18 pagesVeins: Anatomy Department, School of Medicine, Wuhan Universityapi-19641337No ratings yet
- Cephalic VeinDocument1 pageCephalic VeinTogaju KuboyeNo ratings yet
- K5 DAN K6 - Anatomi Throax, Abdomen, Dan PelvisDocument43 pagesK5 DAN K6 - Anatomi Throax, Abdomen, Dan PelvisyuyunNo ratings yet
- Digesti 2: Dr. Agus Budi UtomoDocument90 pagesDigesti 2: Dr. Agus Budi UtomoMuhammad Nur SidiqNo ratings yet
- 549-2. Article Text - Manuscript-2768-1-10-20151106Document5 pages549-2. Article Text - Manuscript-2768-1-10-20151106Estanislao MartinNo ratings yet
- Cardiac ImagingDocument118 pagesCardiac ImagingSay DieukayNo ratings yet
- Clinical Examination of Respiratory System.......Document45 pagesClinical Examination of Respiratory System.......Sreedeep TejaNo ratings yet
- Thoracic 428 Edited2Document87 pagesThoracic 428 Edited2Mihary RamanandraitsioryNo ratings yet
- Anatomy Board Review 11-12Document80 pagesAnatomy Board Review 11-12Mark MaNo ratings yet
- Physiology - Cardiovascular Sys.Document8 pagesPhysiology - Cardiovascular Sys.Nur Liyana MohamadNo ratings yet
- Bimbingan Toraks NormalDocument40 pagesBimbingan Toraks NormalTheArieyadhiNo ratings yet
- Falciform Ligament: Jump To Navigation Jump To SearchDocument6 pagesFalciform Ligament: Jump To Navigation Jump To SearchsakuraleeshaoranNo ratings yet
- Systemic Venous Anomalies - DR RanjithDocument96 pagesSystemic Venous Anomalies - DR RanjithKhaled S. HarbNo ratings yet
- Thoracic Imaging Radiographic BasicsDocument130 pagesThoracic Imaging Radiographic BasicsIsak ShatikaNo ratings yet
- The Anatomy of The Pelvis: Structures Important To The Pelvic Surgeon Workshop 45 Tuesday 24 August 2010, 14:00 - 18:00Document29 pagesThe Anatomy of The Pelvis: Structures Important To The Pelvic Surgeon Workshop 45 Tuesday 24 August 2010, 14:00 - 18:00Kumah WisdomNo ratings yet
- Vascular AnomaliesDocument77 pagesVascular AnomaliesRazan AlayedNo ratings yet
- Anatomy of Circulatory SystDocument6 pagesAnatomy of Circulatory SystKyle PoticarNo ratings yet
- Chest Radiology 1Document120 pagesChest Radiology 1heba1997bshNo ratings yet
- Cardiac Imaging Sept 2016tDocument254 pagesCardiac Imaging Sept 2016tColeen Joyce NeyraNo ratings yet
- KUMC 18 Vascular Supply To UE StudentDocument36 pagesKUMC 18 Vascular Supply To UE StudentAzwarmuslimHasballahAminNo ratings yet
- Relisys Medical Peripheral Tranning 1Document20 pagesRelisys Medical Peripheral Tranning 1Harendra NavinNo ratings yet
- Laboratory 11Document8 pagesLaboratory 11Jc JardinicoNo ratings yet
- Abdomen and Pelvis Vessels & NervesDocument48 pagesAbdomen and Pelvis Vessels & NervesMajd HusseinNo ratings yet
- 3.1 Anterior Abdominal Wall (Bea)Document5 pages3.1 Anterior Abdominal Wall (Bea)Norjetalexis CabreraNo ratings yet
- Medtronic HBP Basics ELearnDocument77 pagesMedtronic HBP Basics ELearnRichiNo ratings yet
- Ar Te Ri Es: Abdominal RegionDocument36 pagesAr Te Ri Es: Abdominal RegionLeony CrisostomoNo ratings yet
- CT Abdomen/Pelvis Anatomy Usc/Som Department of Radiology Kirk Peterson, MDDocument53 pagesCT Abdomen/Pelvis Anatomy Usc/Som Department of Radiology Kirk Peterson, MDArip NurpriadiNo ratings yet
- Vascular Supply To Upper ExtremityDocument36 pagesVascular Supply To Upper ExtremityFrancis ChegeNo ratings yet
- 1166 Stomach Dr.-RaviDocument38 pages1166 Stomach Dr.-RaviKubra ĖdrisNo ratings yet
- Chest X-Ray InterpretationDocument55 pagesChest X-Ray InterpretationMaryam OmarNo ratings yet
- Aorta AnatomyDocument41 pagesAorta AnatomySingey LhendupNo ratings yet
- 2008 Venous and Lymphatic SystemsDocument63 pages2008 Venous and Lymphatic Systemsprasun_vNo ratings yet
- EsophagusDocument25 pagesEsophagusAhmad NizamNo ratings yet
- Practical Checklist PD CVS OnlyDocument6 pagesPractical Checklist PD CVS OnlyardiandawoodNo ratings yet
- Chest X-Ray InterpretationDocument116 pagesChest X-Ray Interpretation6130016019 AISYAH WANDA PUSPANINGTYASNo ratings yet
- l21. Surgical Conditions of ThyroidDocument107 pagesl21. Surgical Conditions of Thyroidmohd bakarNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument28 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Last Moment Revision in Anatomy To Practice of MedicineDocument30 pagesLast Moment Revision in Anatomy To Practice of Medicinevavij71588No ratings yet
- 2 1-S2.0-S1930043317305782-MainDocument5 pages2 1-S2.0-S1930043317305782-MainmihaelamocanNo ratings yet
- Lorma Colleges College of Physical and Respiratory TherapyDocument33 pagesLorma Colleges College of Physical and Respiratory TherapyAnab Mohamed Elhassan Abbas AlnowNo ratings yet
- Circulatory Sytem of The CatDocument3 pagesCirculatory Sytem of The CatIvy CruzNo ratings yet
- Pelvimetría Clínica PDFDocument7 pagesPelvimetría Clínica PDFCamargo Pinto LeonardoNo ratings yet
- Overview of Principal Blood Vessels (Arteries) : Learning ObjectivesDocument8 pagesOverview of Principal Blood Vessels (Arteries) : Learning ObjectivesUloko ChristopherNo ratings yet
- Guidelines For Laboratory Demonstrations. Lab 1 - Superficial Back. Structures To Show Important ConceptsDocument7 pagesGuidelines For Laboratory Demonstrations. Lab 1 - Superficial Back. Structures To Show Important Conceptsjtarta19659No ratings yet
- Cardiovascular Anatomy Physiology: NAMA: Andy Setiawan NIM: 2111102411150Document42 pagesCardiovascular Anatomy Physiology: NAMA: Andy Setiawan NIM: 2111102411150andy stwnNo ratings yet
- Anatomy VeinDocument12 pagesAnatomy VeinReinaldo AbenteNo ratings yet
- Gross Anatomy-Review NotesDocument56 pagesGross Anatomy-Review NotesJohnNo ratings yet
- Phlebotomy Puncture Juncture: Preventing Phlebotomy Errors-Potential For Harming Your PatientsDocument4 pagesPhlebotomy Puncture Juncture: Preventing Phlebotomy Errors-Potential For Harming Your PatientsBelleNo ratings yet
- Final Exam PointersDocument53 pagesFinal Exam PointersBelleNo ratings yet
- CNS Drugs ExaminationDocument2 pagesCNS Drugs ExaminationBelleNo ratings yet
- Pathogenesis and Morphorlogy of Tuberculosis M. O. UdohDocument6 pagesPathogenesis and Morphorlogy of Tuberculosis M. O. UdohBelleNo ratings yet
- Chronic Hyperuricemia, Uric Acid Deposit and Cardiovascular RiskDocument7 pagesChronic Hyperuricemia, Uric Acid Deposit and Cardiovascular RiskBelleNo ratings yet
- Review of The Autonomic Nervous SystemDocument31 pagesReview of The Autonomic Nervous SystemBelleNo ratings yet
- Review of The Autonomic Nervous SystemDocument31 pagesReview of The Autonomic Nervous SystemBelleNo ratings yet
- 100 Words To Describe Facial ExpressionsDocument5 pages100 Words To Describe Facial ExpressionsDanaNo ratings yet
- Depression Essay TopicsDocument7 pagesDepression Essay Topicsrlxaqgnbf100% (2)
- Palliative SurgeryDocument2 pagesPalliative SurgeryCrisel EvangelistaNo ratings yet
- Swine Management Manual: Agricultural InstructionalDocument129 pagesSwine Management Manual: Agricultural InstructionaljaiNo ratings yet
- Health Salt 2Document7 pagesHealth Salt 2Nithyalawrence LawrenceNo ratings yet
- Clinical Veterinary Advisor Dogs and Cats by Etienne Cote DVMDACVIMCardiology and Small Animal Internal Medicine - 5 Star ReviewDocument2 pagesClinical Veterinary Advisor Dogs and Cats by Etienne Cote DVMDACVIMCardiology and Small Animal Internal Medicine - 5 Star ReviewMirsad Gilic0% (1)
- Genetics Practice Problems: Purple Flowers Are Dominant To White Brown Eyes Are Dominant To BlueDocument5 pagesGenetics Practice Problems: Purple Flowers Are Dominant To White Brown Eyes Are Dominant To BlueTheodore Brian KartawinataNo ratings yet
- Anisa Rahma Dewi - Artikel MetpenDocument9 pagesAnisa Rahma Dewi - Artikel MetpenAnisa Rahma DewiNo ratings yet
- Text 1: Source: Danti://uilibraryDocument4 pagesText 1: Source: Danti://uilibrarylissa rositaNo ratings yet
- Who Di 31-4 Atc-DddDocument6 pagesWho Di 31-4 Atc-DddHenderika Lado MauNo ratings yet
- "So You Want To Be A Medical Microbiologist": Key PointsDocument2 pages"So You Want To Be A Medical Microbiologist": Key PointsJoan BandaNo ratings yet
- ONMEDDocument3 pagesONMEDTyas DesmaniasNo ratings yet
- Endocrinology: Nplex Review Kimberly Sanders, NDDocument37 pagesEndocrinology: Nplex Review Kimberly Sanders, NDValeria AcevedoNo ratings yet
- The Role of Imaging in Acute Ischemic Stroke: E T, M.D., Q H, M.D., P .D., J B. F, M.D., M W, M.D., M.a.SDocument17 pagesThe Role of Imaging in Acute Ischemic Stroke: E T, M.D., Q H, M.D., P .D., J B. F, M.D., M W, M.D., M.a.Schrist_cruzerNo ratings yet
- Agenda Packet For Caddo Commission Meeting June 8, 2023Document88 pagesAgenda Packet For Caddo Commission Meeting June 8, 2023CurtisNo ratings yet
- Chemtrails and Covid-19: Two Faces of EvilDocument17 pagesChemtrails and Covid-19: Two Faces of EvilFer TenerifeNo ratings yet
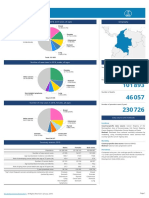
- 170 Colombia Fact SheetsDocument2 pages170 Colombia Fact SheetsLesly RodriguezNo ratings yet
- SITAGLIPTINDocument15 pagesSITAGLIPTINOnon EssayedNo ratings yet
- Penyakit Sendi Degeneratif & Patologi TulangDocument38 pagesPenyakit Sendi Degeneratif & Patologi Tulangnaufal ihsanNo ratings yet