You might also like
- Perioperative Nursing ReportDocument19 pagesPerioperative Nursing ReportPortia Dulce Patatag Toquero100% (1)
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- Care of Patient With Respiratory DisordersDocument35 pagesCare of Patient With Respiratory Disorderskriiteeabns100% (1)
- Duties of scrub and circulating nurses (38Document12 pagesDuties of scrub and circulating nurses (38ckimkimkimNo ratings yet
- BSN3-1 Perioperative-Nursing 2021Document236 pagesBSN3-1 Perioperative-Nursing 2021Ms MedSurg Nursin100% (2)
- Intra Op CombinedDocument62 pagesIntra Op CombinedJan Federick Bantay100% (1)
- IELTS Essay SamplesDocument5 pagesIELTS Essay SamplesRebaz Jamal AhmedNo ratings yet
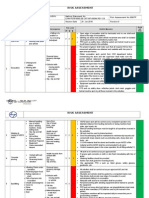
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- Asepsi S: SurgicalDocument47 pagesAsepsi S: Surgicalspongebob27No ratings yet
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Intraoperative 2Document104 pagesIntraoperative 2Mark Arryson CasisonNo ratings yet
- Care of Clients Requiring SurgeryDocument27 pagesCare of Clients Requiring SurgeryNokz M. Raki-inNo ratings yet
- Immediate DenturesDocument35 pagesImmediate DenturesSimran SahniNo ratings yet
- Operating NURSEDocument8 pagesOperating NURSEAlexis de los SantosNo ratings yet
- Aseptic TechniqueDocument15 pagesAseptic Techniquerhizalyn13No ratings yet
- Types of Surgeries Preoperative Nursing Care Preoperative Nursing CareDocument6 pagesTypes of Surgeries Preoperative Nursing Care Preoperative Nursing CareDarlyn AmplayoNo ratings yet
- Surgical Handwashing Resource Material 2023-2024Document9 pagesSurgical Handwashing Resource Material 2023-2024Cherry Louise O. SanvictoresNo ratings yet
- Asepsis and Aseptic Practices in The Operating RoomDocument5 pagesAsepsis and Aseptic Practices in The Operating RoomSalinder Kaur DhaliwalNo ratings yet
- Chapter IiDocument37 pagesChapter Iicoosa liquors100% (1)
- Scrub Nurse1Document50 pagesScrub Nurse1Amy Lalringhluani Chhakchhuak100% (1)
- Perioperative NursingDocument12 pagesPerioperative Nursingtheglobalnursing100% (12)
- Isolation Practices & Sterile Technique GuideDocument91 pagesIsolation Practices & Sterile Technique GuidenicNo ratings yet
- Perioperative Nursing LectureDocument125 pagesPerioperative Nursing LectureHazel Von S. Bravo88% (24)
- Duties of Scrub Nurse & Circulating NurseDocument2 pagesDuties of Scrub Nurse & Circulating Nurseimafashionista90% (21)
- Risk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeDocument3 pagesRisk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeSenyorita KHaye75% (12)
- Intraoperative Phase 2021Document62 pagesIntraoperative Phase 2021Jmarie Brillantes PopiocoNo ratings yet
- Scrub and Circulating Nurses DutiesDocument7 pagesScrub and Circulating Nurses DutiesJune Dumdumaya100% (1)
- Or Rle 1-1Document23 pagesOr Rle 1-1Jan Federick Bantay100% (1)
- Readiness For Enhanced Knowledge NCP FDARDocument4 pagesReadiness For Enhanced Knowledge NCP FDARRaidis Pangilinan100% (2)
- Water Treatment PDFDocument87 pagesWater Treatment PDFJubin KumarNo ratings yet
- Aseptic Technique ProcedureDocument10 pagesAseptic Technique ProcedureaksinuNo ratings yet
- Contrast and Special Radiographic Procedures: Topic - Aseptic TechniquesDocument15 pagesContrast and Special Radiographic Procedures: Topic - Aseptic TechniquesPOOJA MNo ratings yet
- Operating RoomDocument4 pagesOperating RoomKristine Anne Liquiran Avenado100% (1)
- Perioperative Nursing CareDocument124 pagesPerioperative Nursing CarePaul Anthony Lorica100% (1)
- What Is Aseptic TechniqueDocument11 pagesWhat Is Aseptic TechniqueMarlchiel Nathan ArregladoNo ratings yet
- Assisted Gowning & GlovingDocument12 pagesAssisted Gowning & GlovingCarmina GurreaNo ratings yet
- Operating Room Nursing GuideDocument20 pagesOperating Room Nursing GuideErika BacarroNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- MCA - LAB - Sterile Technique Procedures - NotesDocument7 pagesMCA - LAB - Sterile Technique Procedures - NotesRaynelah AnnNo ratings yet
- Or ResponsibilitiesDocument26 pagesOr ResponsibilitiesFrancine kimberlyNo ratings yet
- Surgical AsepsisDocument4 pagesSurgical AsepsisChristian Pardilla BuenaNo ratings yet
- Asepsis and Aseptic Practices in The Operating RoomDocument6 pagesAsepsis and Aseptic Practices in The Operating RoomMichelle ViduyaNo ratings yet
- DARUNDAY Written Requirements of Assigned ReadingsDocument17 pagesDARUNDAY Written Requirements of Assigned ReadingsEzra Miguel DarundayNo ratings yet
- Post Test Name: Rosenie H. Tanag YR/SEC: BSN 3-1 Score: - Learning ActivityDocument3 pagesPost Test Name: Rosenie H. Tanag YR/SEC: BSN 3-1 Score: - Learning ActivityCorrine IvyNo ratings yet
- Perioperative: Operating Room AttireDocument95 pagesPerioperative: Operating Room AttireCristina Tagle GarciaNo ratings yet
- Or Notes UpdatedDocument11 pagesOr Notes UpdatedKc Cabanilla LizardoNo ratings yet
- Roles of Surgeon, Assistant, Anesthesiologist, Scrub & Circulating Nurses (38Document3 pagesRoles of Surgeon, Assistant, Anesthesiologist, Scrub & Circulating Nurses (38chacha javierNo ratings yet
- Goso: General ObjectiveDocument26 pagesGoso: General ObjectiveGIOVANNIE II JAPSONNo ratings yet
- OR Sitting and Sterile Technique GuideDocument50 pagesOR Sitting and Sterile Technique Guidetsega tilahunNo ratings yet
- Document 1Document20 pagesDocument 1Khryzzia Mae DiacomaNo ratings yet
- Operating Room Technique Write Up PAPA SLRCDocument43 pagesOperating Room Technique Write Up PAPA SLRCShane Vlademier ParadoNo ratings yet
- Aseptic TechniqueDocument10 pagesAseptic TechniqueDeborah Chimeremeze JosephNo ratings yet
- Etiquette and PrinciplesDocument3 pagesEtiquette and PrinciplesHoney Bee S. PlatolonNo ratings yet
- MedsurDocument116 pagesMedsurMacy MarquezNo ratings yet
- Perioperative Nursing Module 2Document147 pagesPerioperative Nursing Module 2fleur harrisonNo ratings yet
- Surgical Preparation & Procedures: Chapter 14 - Lesson 2Document2 pagesSurgical Preparation & Procedures: Chapter 14 - Lesson 2Nugroho WibisonoNo ratings yet
- Operating Room Personnel OrganizationDocument4 pagesOperating Room Personnel OrganizationantihistamiiineNo ratings yet
- Operation Theatre Technique Indepth StudyDocument42 pagesOperation Theatre Technique Indepth Studyjyoti singhNo ratings yet
- Perioperative Nursing Lecture 2Document54 pagesPerioperative Nursing Lecture 2Gabriel GagaNo ratings yet
- NCM 112 Perioperative NursingDocument5 pagesNCM 112 Perioperative Nursingsecondacvalo123No ratings yet
- Perioperative NursingDocument148 pagesPerioperative NursingBok's TriadNo ratings yet
- Perioperative SkillsDocument23 pagesPerioperative Skillsapi-3722454100% (1)
- or ConceptsDocument65 pagesor ConceptsAzehr CommzNo ratings yet
- Aseptic TechniqueDocument10 pagesAseptic TechniqueIan Carlo Padama MosesNo ratings yet
- Aseptic and Aseptic TechniqueDocument12 pagesAseptic and Aseptic Techniqueofficial1basherNo ratings yet
- Peri Operative LectureDocument17 pagesPeri Operative LectureErica Mei CapiliNo ratings yet
- Manual of Ambulatory General Surgery: A Step-by-Step Guide to Minor and Intermediate SurgeryFrom EverandManual of Ambulatory General Surgery: A Step-by-Step Guide to Minor and Intermediate SurgeryNo ratings yet
- Mitochondrion: Name: - Darlyn I. Amplayo - Section: - A2-PyponcoDocument2 pagesMitochondrion: Name: - Darlyn I. Amplayo - Section: - A2-PyponcoDarlyn AmplayoNo ratings yet
- Objectives in SurgeryDocument1 pageObjectives in SurgeryDarlyn AmplayoNo ratings yet
- Case Scenario Types of Surgery and Pre-Op Care PDFDocument1 pageCase Scenario Types of Surgery and Pre-Op Care PDFDarlyn AmplayoNo ratings yet
- What Is CancerDocument7 pagesWhat Is CancerDarlyn AmplayoNo ratings yet
- Objectives for Surgery RotationDocument1 pageObjectives for Surgery RotationDarlyn AmplayoNo ratings yet
- Guide Questions For Treatment of ModalitiesDocument1 pageGuide Questions For Treatment of ModalitiesDarlyn AmplayoNo ratings yet
- A. Badiou - Who Is NietzscheDocument6 pagesA. Badiou - Who Is Nietzscheforzamhj100% (1)
- FA-51 FinalDocument1 pageFA-51 FinalDarlyn AmplayoNo ratings yet
- Client With StrokeDocument11 pagesClient With StrokeDarlyn AmplayoNo ratings yet
- Macmorris SlidesCarnivalDocument16 pagesMacmorris SlidesCarnivalDarlyn AmplayoNo ratings yet
- CA 1 ReactionDocument1 pageCA 1 ReactionDarlyn AmplayoNo ratings yet
- Leaflet For ORDocument2 pagesLeaflet For ORDarlyn AmplayoNo ratings yet
- MedicalDocument2 pagesMedicalDarlyn AmplayoNo ratings yet
- Lecture NotesDocument13 pagesLecture NotesDarlyn AmplayoNo ratings yet
- Copy Me Game MechanicsDocument1 pageCopy Me Game MechanicsDarlyn AmplayoNo ratings yet
- Postoperative Nursing ResponsibilitiesDocument1 pagePostoperative Nursing ResponsibilitiesDarlyn AmplayoNo ratings yet
- Midterm ExamDocument18 pagesMidterm ExamDarlyn AmplayoNo ratings yet
- Article 1 - HemorrhoidectomyDocument2 pagesArticle 1 - HemorrhoidectomyDarlyn AmplayoNo ratings yet
- SHT Post-Op ExercisesDocument6 pagesSHT Post-Op ExercisesDarlyn AmplayoNo ratings yet
- Article 1 - HemorrhoidectomyDocument2 pagesArticle 1 - HemorrhoidectomyDarlyn AmplayoNo ratings yet
- Leaflet For ORDocument2 pagesLeaflet For ORDarlyn AmplayoNo ratings yet
- SakuraDocument1 pageSakuraDarlyn AmplayoNo ratings yet
- Leaflet For ORDocument2 pagesLeaflet For ORDarlyn AmplayoNo ratings yet
- Tales From MindanaoDocument2 pagesTales From MindanaoDauntless Karen0% (1)
- Amputations SyllabusDocument7 pagesAmputations SyllabusDarlyn AmplayoNo ratings yet
- CoverpageDocument3 pagesCoverpageDarlyn AmplayoNo ratings yet
- Worksheet On Preganancy Fetal Development Labor and DeliveryDocument4 pagesWorksheet On Preganancy Fetal Development Labor and DeliveryDarlyn AmplayoNo ratings yet
- Fa 2Document3 pagesFa 2Darlyn AmplayoNo ratings yet
- Managing Painful Diabetic NeuropathyDocument26 pagesManaging Painful Diabetic NeuropathyAthalia TalawayNo ratings yet
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- List of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atDocument2 pagesList of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atAdegokeNo ratings yet
- Multi-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseDocument28 pagesMulti-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseSobek1789No ratings yet
- Anna Fagin Resume Aug 2014Document1 pageAnna Fagin Resume Aug 2014api-261821160No ratings yet
- Lymphoedema Volume Measurement Form: Sánchez Disano Jeremias R R 24Document1 pageLymphoedema Volume Measurement Form: Sánchez Disano Jeremias R R 24Manuel OvelarNo ratings yet
- Avulsi Dan Degloving Injury Dr. LuthfiDocument26 pagesAvulsi Dan Degloving Injury Dr. Luthfimutiara firdausyNo ratings yet
- Plant Tissue Culture Media PDFDocument3 pagesPlant Tissue Culture Media PDFTitan Biotech100% (1)
- PIL For Sudafed DecongestantDocument2 pagesPIL For Sudafed DecongestantOdunlamiNo ratings yet
- City of Peterborough 2023 Draft Capital BudgetDocument535 pagesCity of Peterborough 2023 Draft Capital BudgetPeterborough ExaminerNo ratings yet
- Introduction To The Alpaca andDocument9 pagesIntroduction To The Alpaca andMai Chi PhạmNo ratings yet
- Theory Critique of Boundaries in MarriageDocument8 pagesTheory Critique of Boundaries in MarriagepatrickakingNo ratings yet
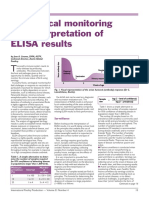
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- CV 2020Document3 pagesCV 2020api-519861494No ratings yet
- Ultrasound-Guided Lumbar Central Neuraxial Block 2016Document8 pagesUltrasound-Guided Lumbar Central Neuraxial Block 2016drkis20100% (1)
- KPJ Pasir Gudang Covid Test ReportDocument1 pageKPJ Pasir Gudang Covid Test ReportNooh DinNo ratings yet
- Empowering Women Key to Ending PovertyDocument25 pagesEmpowering Women Key to Ending PovertydassmbaNo ratings yet
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- Chapt01 The Sudy of ChangeDocument34 pagesChapt01 The Sudy of ChangeIkhsan Abdul HanifNo ratings yet
- The Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LDocument8 pagesThe Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LSyifa UlNo ratings yet
- A Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreDocument11 pagesA Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreRamasamyNagarajan100% (1)