You might also like
- AntibioticsDocument53 pagesAntibioticsMaheen IdreesNo ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- Integrated Care Applying Theory To PracticeDocument429 pagesIntegrated Care Applying Theory To PracticeMyriam Hernández Núñez100% (1)
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- Antimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Document58 pagesAntimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Fred OseiNo ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- AMINOGLYCOSIDES AND MACROLIDES: MECHANISMS AND CLINICAL USESDocument45 pagesAMINOGLYCOSIDES AND MACROLIDES: MECHANISMS AND CLINICAL USESAbdullah EmadNo ratings yet
- Provisional RestorationsDocument4 pagesProvisional RestorationsMyri Gebert SchererNo ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- AntibioticsDocument84 pagesAntibioticsNandini GulurNo ratings yet
- 5 6287273689696174255Document318 pages5 6287273689696174255rani silahudinNo ratings yet
- Diagnostic Aids in ProsthodonticsDocument60 pagesDiagnostic Aids in ProsthodonticsAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Antibacterials and AntibioticsDocument44 pagesAntibacterials and AntibioticsVallejo Taberna HannalieNo ratings yet
- Comprehensive Hospital Strategic Plan ExampleDocument28 pagesComprehensive Hospital Strategic Plan ExampleEsteban R. Langlois100% (1)
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- Antibiotic Resistance: Dr. Sharifah Shakinah Supervisor: Dr. Eppy SPPD KptiDocument25 pagesAntibiotic Resistance: Dr. Sharifah Shakinah Supervisor: Dr. Eppy SPPD KptiShasha Shakinah100% (1)
- Multiple SclerosisDocument6 pagesMultiple SclerosisRonnel Alvin Antonio AdrianoNo ratings yet
- OgminDocument7 pagesOgminSharar KalayliehNo ratings yet
- Augmentin in JDocument15 pagesAugmentin in JChutharat SucharitNo ratings yet
- AugmentinDocument7 pagesAugmentinImran KhanNo ratings yet
- Nurse Round - AugmentinDocument15 pagesNurse Round - AugmentinkyokeungkennethNo ratings yet
- Antimicrobial Pharmacologyforthe Neonatalfoal: K. Gary MagdesianDocument19 pagesAntimicrobial Pharmacologyforthe Neonatalfoal: K. Gary MagdesianCristhian Jover CastroNo ratings yet
- Ampicillin SulbactamDocument5 pagesAmpicillin SulbactamtitiNo ratings yet
- Hikma Pharmaceuticals: AmoclanDocument5 pagesHikma Pharmaceuticals: AmoclanBest ManNo ratings yet
- AmoxitidDocument5 pagesAmoxitidelcapitano vegetaNo ratings yet
- AmoxicillinDocument3 pagesAmoxicillinElena DenisaNo ratings yet
- AmoxicillinDocument8 pagesAmoxicillinMariusNeicuNo ratings yet
- 20120613Document16 pages20120613ALi Rḿ ḾöhẳḿḿẳdNo ratings yet
- Biology Lab Report AntibioticsDocument8 pagesBiology Lab Report AntibioticsLoore Liflander100% (1)
- Clamo Powder For Oral Suspension 312.5mg/5ml Drug InteractionDocument2 pagesClamo Powder For Oral Suspension 312.5mg/5ml Drug InteractionRania T. SabriNo ratings yet
- Calamox Tablets SuspensionsDocument4 pagesCalamox Tablets SuspensionsAbdurrahman DarmanNo ratings yet
- Augmentin ES 600 MDS006Document18 pagesAugmentin ES 600 MDS006JeneshNo ratings yet
- AntibioticsDocument24 pagesAntibioticsAlba GonzálezNo ratings yet
- AntibacterialsDocument8 pagesAntibacterialslisalynnleeNo ratings yet
- Amoxicillin PDFDocument6 pagesAmoxicillin PDFNaveen KumarNo ratings yet
- AugmentinDocument24 pagesAugmentinKaren Ann M. EstradaNo ratings yet
- CARBAPENEMS for treating serious infectionsDocument5 pagesCARBAPENEMS for treating serious infectionsabam_abamNo ratings yet
- Composition: Amoxicillin and Clavulanate Potassium Tablets USPDocument5 pagesComposition: Amoxicillin and Clavulanate Potassium Tablets USPManjeet SinghNo ratings yet
- Lac 10&11 PPTDocument16 pagesLac 10&11 PPTRaghdaNo ratings yet
- Reviewer - Pharmacology FinalsDocument17 pagesReviewer - Pharmacology Finalsarmanuel1390antNo ratings yet
- TerrexineDocument5 pagesTerrexineWakhidatus InryaNo ratings yet
- Antibacterial Agents Antimicrobial Antibiotic: Leilani O. Estacio, Man RNDocument44 pagesAntibacterial Agents Antimicrobial Antibiotic: Leilani O. Estacio, Man RNHERLIN HOBAYANNo ratings yet
- Treatment of Bacterial Infections 343Document48 pagesTreatment of Bacterial Infections 343ALNAKINo ratings yet
- MoxaclavDocument3 pagesMoxaclavAshish SharmaNo ratings yet
- AmpicillinsulbactamupdateDocument14 pagesAmpicillinsulbactamupdateOrlando EscalonaNo ratings yet
- Aminoglycoside AntibioticsDocument36 pagesAminoglycoside AntibioticsGeneral InquiriesNo ratings yet
- Pharmacology: Classification and Mode of Action of AntibioticsDocument44 pagesPharmacology: Classification and Mode of Action of AntibioticsAamir AzizNo ratings yet
- Effect of Antibiotic On BacteriaDocument19 pagesEffect of Antibiotic On BacteriaTootsie100% (2)
- Amoxicillin (: INN BAN β-lactam antibiotic bacterial infections microorganismsDocument17 pagesAmoxicillin (: INN BAN β-lactam antibiotic bacterial infections microorganismsNiks KanungoNo ratings yet
- Pharmacology Guide to Antimicrobials & ResistanceDocument86 pagesPharmacology Guide to Antimicrobials & ResistanceRuthvi Jain100% (1)
- Unit 1 - MC 3Document58 pagesUnit 1 - MC 3Shreyas ShreyuNo ratings yet
- Antibacterilal Therapy of MastitisDocument8 pagesAntibacterilal Therapy of MastitisSunilNo ratings yet
- The Macrolide Antibiotics 1 1Document6 pagesThe Macrolide Antibiotics 1 1John PaulNo ratings yet
- Drug InfoDocument11 pagesDrug InfoArjun SinghNo ratings yet
- Product Knowledge (2) (26-8) 2-1Document38 pagesProduct Knowledge (2) (26-8) 2-1zeyad1234ali0No ratings yet
- Antimicrobial Drugs: Laboratory of Microbiology Medical Faculty Brawijaya UniversityDocument38 pagesAntimicrobial Drugs: Laboratory of Microbiology Medical Faculty Brawijaya UniversityYuu Ayu'k LifestarNo ratings yet
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 pagesChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةNo ratings yet
- m265 Lec 10 - Antimicrobial Agents and Resistance - Part 1 PDFDocument20 pagesm265 Lec 10 - Antimicrobial Agents and Resistance - Part 1 PDFHãnëën TwalbehNo ratings yet
- AmoxicillinDocument1 pageAmoxicillinAnthony BrookNo ratings yet
- Chemotherapy NotesDocument9 pagesChemotherapy Notesnileshkumarhjoshi942No ratings yet
- ANTIBIOTICS IN ORAL SURGERYs 123Document43 pagesANTIBIOTICS IN ORAL SURGERYs 123Puneet SinghNo ratings yet
- 9 - Anti Fungal DrugsDocument73 pages9 - Anti Fungal Drugszynab123No ratings yet
- Antibiotics FamiliesDocument5 pagesAntibiotics FamiliesTiffany SamanthaNo ratings yet
- Cephalosporins and other beta-lactam antibioticsDocument19 pagesCephalosporins and other beta-lactam antibioticsسلام شاكر حميد جميل 6506No ratings yet
- AntibiotikaDocument47 pagesAntibiotikaRaditya PutraNo ratings yet
- Chapter 044Document5 pagesChapter 044borisdevic223No ratings yet
- Antibiotics 11.05.19Document18 pagesAntibiotics 11.05.19dahiphale1No ratings yet
- Microbiology - Exercise 3e AntibiogramDocument5 pagesMicrobiology - Exercise 3e Antibiogramapi-253346521No ratings yet
- GENERIC NAME: Co-Amoxiclav (Amoxicillin & Clavulanic Acid) BRAND NAMES: Natravox, AddexDocument4 pagesGENERIC NAME: Co-Amoxiclav (Amoxicillin & Clavulanic Acid) BRAND NAMES: Natravox, AddexDRANo ratings yet
- Amoxicillin: A Beginner's 20-Minute Quick Guide Overview on its Use Cases to Treat Bacterial Infection and Side EffectsFrom EverandAmoxicillin: A Beginner's 20-Minute Quick Guide Overview on its Use Cases to Treat Bacterial Infection and Side EffectsNo ratings yet
- The Essential Guide to Amoxicillin: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Amoxicillin: Usage, Precautions, Interactions and Side Effects.No ratings yet
- ATLS Practice Questions FreeDocument4 pagesATLS Practice Questions Freeelcapitano vegetaNo ratings yet
- Zinex TabDocument4 pagesZinex Tabelcapitano vegetaNo ratings yet
- Voloxal TabletsDocument9 pagesVoloxal Tabletselcapitano vegetaNo ratings yet
- Magna Cill inDocument4 pagesMagna Cill inelcapitano vegetaNo ratings yet
- Erythrolet ErythrotabDocument5 pagesErythrolet Erythrotabelcapitano vegetaNo ratings yet
- Cefpo TabletDocument7 pagesCefpo Tabletelcapitano vegetaNo ratings yet
- ZetamycinDocument6 pagesZetamycinelcapitano vegetaNo ratings yet
- Zinex VialDocument5 pagesZinex Vialelcapitano vegetaNo ratings yet
- Profort VialDocument8 pagesProfort Vialelcapitano vegetaNo ratings yet
- Clindacin CapsDocument5 pagesClindacin Capselcapitano vegetaNo ratings yet
- Lari CidDocument5 pagesLari Cidelcapitano vegetaNo ratings yet
- CeproxxDocument6 pagesCeproxxelcapitano vegetaNo ratings yet
- MetrozoleDocument5 pagesMetrozoleelcapitano vegetaNo ratings yet
- Ultracin CapletDocument5 pagesUltracin Capletelcapitano vegetaNo ratings yet
- CefalexDocument4 pagesCefalexelcapitano vegetaNo ratings yet
- Bepen VKDocument5 pagesBepen VKelcapitano vegetaNo ratings yet
- CefadroxDocument4 pagesCefadroxelcapitano vegetaNo ratings yet
- Azimex CapsDocument6 pagesAzimex Capselcapitano vegetaNo ratings yet
- Cefixon VialDocument7 pagesCefixon Vialelcapitano vegetaNo ratings yet
- Azimex SuspensionDocument7 pagesAzimex Suspensionelcapitano vegetaNo ratings yet
- AmoxitidDocument5 pagesAmoxitidelcapitano vegetaNo ratings yet
- CHARTINGDocument7 pagesCHARTINGGEN COLLANTESNo ratings yet
- KROK2 3 профиль (88Qs) 2004-2005Document14 pagesKROK2 3 профиль (88Qs) 2004-2005Ali ZeeshanNo ratings yet
- Gliomas Linea Media 1Document9 pagesGliomas Linea Media 1JOHN LOPERANo ratings yet
- PharmCal Chapters 13Document19 pagesPharmCal Chapters 13Alexa Claire CabalbalNo ratings yet
- Preventive Aspect of Vyayama (Physical Exercise) : January 2015Document8 pagesPreventive Aspect of Vyayama (Physical Exercise) : January 2015priyanka sharmaNo ratings yet
- Schedule Ismi HottiDocument23 pagesSchedule Ismi HottisigitNo ratings yet
- Chapter 5 Prep U.odtDocument6 pagesChapter 5 Prep U.odtLivan MartellNo ratings yet
- Multiplepregnancy 100515015745 Phpapp01Document29 pagesMultiplepregnancy 100515015745 Phpapp01haisureshNo ratings yet
- Mbbs Freshers ResumeDocument9 pagesMbbs Freshers ResumeTalha Noorani50% (2)
- Or Drug StudyDocument7 pagesOr Drug StudyNikki M. ArapolNo ratings yet
- A Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in The PhilippinesDocument17 pagesA Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in The PhilippinesYukiko CalimutanNo ratings yet
- Fracture Complications PDFDocument3 pagesFracture Complications PDFlemootpNo ratings yet
- Chapter 20 HomeworkDocument9 pagesChapter 20 HomeworkKvn4N6No ratings yet
- Introduction to Continuous Renal Replacement Therapy (CRRT) in ICUDocument25 pagesIntroduction to Continuous Renal Replacement Therapy (CRRT) in ICUyamtotlNo ratings yet
- Translate These Into Communicative EnglishDocument2 pagesTranslate These Into Communicative Englishjuwita lestariNo ratings yet
- B. Inggris TongueDocument2 pagesB. Inggris TongueP17211211007 NURUL HUDANo ratings yet
- Multiple SclerosisDocument96 pagesMultiple SclerosisDrGasnasNo ratings yet
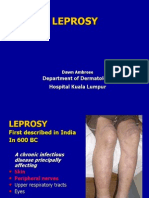
- 10 LeprosyDocument27 pages10 LeprosyMakWohWeiNo ratings yet
- A Comparative Clinical Study To Evaluate The Efficacy of Koshataki Ksharasutra in The Management of Bhagandara With Special Reference To Fistula in AnoDocument7 pagesA Comparative Clinical Study To Evaluate The Efficacy of Koshataki Ksharasutra in The Management of Bhagandara With Special Reference To Fistula in AnoEditor IJTSRDNo ratings yet
- LAPORAN DATA KESAKITAN ICD XDocument5,181 pagesLAPORAN DATA KESAKITAN ICD XReyni ThasariNo ratings yet
- 2006, Vol.19, Issues 2, Ocular Anesthesia PDFDocument156 pages2006, Vol.19, Issues 2, Ocular Anesthesia PDFalvyandaniNo ratings yet
- Erosion of Cardiovascular Implantable Device: Conservative Therapy or Extraction?Document4 pagesErosion of Cardiovascular Implantable Device: Conservative Therapy or Extraction?Randa TabbahNo ratings yet
- BLS-First Aid (FTP-OJT) - 1Document43 pagesBLS-First Aid (FTP-OJT) - 1TMRU TCPSNo ratings yet
- Confidentiality and JusticeDocument3 pagesConfidentiality and JusticeRaseff Tesorero50% (2)