You might also like
- Full Download Test Bank For Introduction To Clinical Psychology 8 e 8th Edition Geoffrey P Kramer Douglas A Bernstein Vicky Phares PDF Full ChapterDocument36 pagesFull Download Test Bank For Introduction To Clinical Psychology 8 e 8th Edition Geoffrey P Kramer Douglas A Bernstein Vicky Phares PDF Full Chaptermichaelharvey16101989bkm100% (19)
- Burn - Concept MapDocument1 pageBurn - Concept MapAaron RafaelNo ratings yet
- BRONZE STAR POWERPOINT PRESENTATIONDocument34 pagesBRONZE STAR POWERPOINT PRESENTATIONwaranchaiNo ratings yet
- Drug StudyDocument4 pagesDrug StudyXio PauNo ratings yet
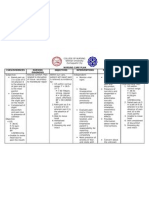
- PHINMA - UNIVERSITY OF ILOILO DRUG STUDY ON ROPIVACAINE/BUPIVACAINEDocument2 pagesPHINMA - UNIVERSITY OF ILOILO DRUG STUDY ON ROPIVACAINE/BUPIVACAINErica sebabillonesNo ratings yet
- Drug Study FinalDocument5 pagesDrug Study FinalJackie Ann Marie DapatNo ratings yet
- DRUG STUDY CLOBETASOL CREAMrevisedDocument2 pagesDRUG STUDY CLOBETASOL CREAMrevisedswitchlers anneNo ratings yet
- DRUG STUDY Allopurinol (Purinase)Document2 pagesDRUG STUDY Allopurinol (Purinase)DennMarkTaponNo ratings yet
- Azithromycin Drug StudyDocument2 pagesAzithromycin Drug StudySHEILA MAE SACLOTNo ratings yet
- Sal But AmolDocument2 pagesSal But AmolCalimlim KimNo ratings yet
- DRUG-STUDY - BALLON, Karlo CDocument6 pagesDRUG-STUDY - BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- PrednisoneDocument22 pagesPrednisoneAlthea AlicandoNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationAbigail BascoNo ratings yet
- Nursing Considerations for MeropenemDocument2 pagesNursing Considerations for MeropenemKullin RainNo ratings yet
- Epirubicin 10Document1 pageEpirubicin 10PdianghunNo ratings yet
- UROKINASE (Kinlytic)Document4 pagesUROKINASE (Kinlytic)Mikaela Gabrielle GeraliNo ratings yet
- Verapamil HCLDocument3 pagesVerapamil HCLMae Ann Bueno CastillonNo ratings yet
- Drug StudyDocument7 pagesDrug StudyHerwincayeNo ratings yet
- Drug StudyDocument7 pagesDrug StudyRej Gallien PontalbaNo ratings yet
- Apixaban 5 PDFDocument2 pagesApixaban 5 PDFWanie Al-basriNo ratings yet
- New DS3Document3 pagesNew DS3dakieNo ratings yet
- Perphenazine Drug StudyDocument4 pagesPerphenazine Drug Studyshadow gonzalezNo ratings yet
- Cefotaxime Drug Class, Uses, Side EffectsDocument3 pagesCefotaxime Drug Class, Uses, Side EffectsKristi WrayNo ratings yet
- Cefipime HCL (AXERA)Document2 pagesCefipime HCL (AXERA)Kristine YoungNo ratings yet
- Atropine SulfateDocument1 pageAtropine SulfateTrishaaMayolNo ratings yet
- Drug StudyDocument21 pagesDrug StudyShyla Garnace JavillonarNo ratings yet
- Drug mechanism indication contraindication side effects nursingDocument1 pageDrug mechanism indication contraindication side effects nursinghahahahaaaaaaaNo ratings yet
- NafarinDocument2 pagesNafarinianecunar100% (2)
- DrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Document2 pagesDrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Coleen Mae CamaristaNo ratings yet
- DRUG STUDY (Diphenhydramine)Document2 pagesDRUG STUDY (Diphenhydramine)Avianna CalliopeNo ratings yet
- Insuget Drug StudyDocument1 pageInsuget Drug StudydollythesheepNo ratings yet
- Drug Study: Phinma University of PangasinanDocument1 pageDrug Study: Phinma University of PangasinanVoid LessNo ratings yet
- NeostigmineDocument4 pagesNeostigmineDonna Lyn B. DizonNo ratings yet
- Activase for Acute Ischemic Stroke and Heart ConditionsDocument3 pagesActivase for Acute Ischemic Stroke and Heart Conditionsmharjoe pulmanoNo ratings yet
- PrednisoloneDocument2 pagesPrednisoloneKatie McPeekNo ratings yet
- College of Nursing: Cebu Normal UniversityDocument3 pagesCollege of Nursing: Cebu Normal UniversityShiva TorinsNo ratings yet
- Example of Drug StudyDocument2 pagesExample of Drug Studydonna mae junioNo ratings yet
- Drug study analyzes sertraline for factitious disorderDocument5 pagesDrug study analyzes sertraline for factitious disorderCamille SanguyoNo ratings yet
- Filgrastim Boosts Neutrophil Recovery After ChemotherapyDocument3 pagesFilgrastim Boosts Neutrophil Recovery After ChemotherapyKyla Barrera TabungarNo ratings yet
- Biperiden Generic and Brand Names, Uses, Side EffectsDocument1 pageBiperiden Generic and Brand Names, Uses, Side EffectsMFQ.RN100% (2)
- ColistinDocument2 pagesColistinGwyn RosalesNo ratings yet
- DantriumDocument2 pagesDantriumAdrianne BazoNo ratings yet
- AtroventDocument2 pagesAtroventKatie McPeekNo ratings yet
- A Drug Study On Vincristine SulfateDocument9 pagesA Drug Study On Vincristine SulfateTrio San LuisNo ratings yet
- Depot-Ped: 3 Months: 11.25 MG or 30 MG Q12weeks. (SQ) Lupron: Children: Initially, 50Document3 pagesDepot-Ped: 3 Months: 11.25 MG or 30 MG Q12weeks. (SQ) Lupron: Children: Initially, 50thuey epeNo ratings yet
- Final Eb ReflectionDocument2 pagesFinal Eb Reflectionapi-238460511No ratings yet
- Insulin Mechanism of Action and Nursing ResponsibilitiesDocument7 pagesInsulin Mechanism of Action and Nursing ResponsibilitiesGrape JuiceNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJan Lianne BernalesNo ratings yet
- DS (Fenofibrate)Document5 pagesDS (Fenofibrate)Mary April MendezNo ratings yet
- Azithromycin Nursing RationaleDocument2 pagesAzithromycin Nursing RationaleYamete KudasaiNo ratings yet
- NCP Mandibular)Document5 pagesNCP Mandibular)yellarfNo ratings yet
- Tramadol and Ciprofloxacin: Key Information for NursesDocument2 pagesTramadol and Ciprofloxacin: Key Information for NursesatchiekNo ratings yet
- Aripiprazole Drug Study - Rhuby AbenojaDocument1 pageAripiprazole Drug Study - Rhuby AbenojaRHUBY ABENOJANo ratings yet
- Drug Study - CefradoxilDocument13 pagesDrug Study - CefradoxilJohara G'naid0% (1)
- Drug study cilostazol intermittent claudicationDocument2 pagesDrug study cilostazol intermittent claudicationart_mutantNo ratings yet
- Drug Study - Voltaren@cefuroxime (Kefox)Document3 pagesDrug Study - Voltaren@cefuroxime (Kefox)Claudette CayetanoNo ratings yet
- Obat Ayu (Anestesi)Document11 pagesObat Ayu (Anestesi)Ayu PratiwiNo ratings yet
- Fentanyl ParenteralDocument7 pagesFentanyl Parenteralstring44No ratings yet
- Local Anesthetics (Slide Show)Document24 pagesLocal Anesthetics (Slide Show)Sheena Lou Regencia SalomonNo ratings yet
- Drug Study..DokcyDocument7 pagesDrug Study..DokcyPeArl Peralta0% (1)
- Iligan - DiazepamDocument6 pagesIligan - DiazepamJamaicah IliganNo ratings yet
- Cloxacillin, Sodium: How Should I Take Cloxacillin?Document7 pagesCloxacillin, Sodium: How Should I Take Cloxacillin?Stacy MC PelitoNo ratings yet
- AmmoniumChloride PDFDocument3 pagesAmmoniumChloride PDFAP TOROBXNo ratings yet
- Aripiprazole Guide for NursesDocument4 pagesAripiprazole Guide for NursesAP TOROBX100% (1)
- Acetaminophen 1Document4 pagesAcetaminophen 1AP TOROBXNo ratings yet
- Timolol MaleateDocument3 pagesTimolol MaleateAP TOROBXNo ratings yet
- NormalSerumAlbumin PDFDocument3 pagesNormalSerumAlbumin PDFAP TOROBXNo ratings yet
- Aluminum Hydroxide Antacids and Phosphate BindersDocument3 pagesAluminum Hydroxide Antacids and Phosphate BindersAP TOROBXNo ratings yet
- Lipitor Lowers CholesterolDocument3 pagesLipitor Lowers CholesterolAP TOROBXNo ratings yet
- Vancomycin HydrochloridesDocument4 pagesVancomycin HydrochloridesAP TOROBXNo ratings yet
- Atropine SulfateDocument5 pagesAtropine SulfateAP TOROBXNo ratings yet
- AmantadineHydrochloride PDFDocument4 pagesAmantadineHydrochloride PDFAP TOROBXNo ratings yet
- ConversionDocument7 pagesConversionAP TOROBXNo ratings yet
- Deontological TheoryDocument22 pagesDeontological TheoryAP TOROBXNo ratings yet
- ConversionDocument7 pagesConversionAP TOROBXNo ratings yet
- SHOTPUTDocument17 pagesSHOTPUTAP TOROBX100% (1)
- .archivetempNLE Tips - For NLE NOV 2017 PDFDocument4 pages.archivetempNLE Tips - For NLE NOV 2017 PDFElizabella Henrietta TanaquilNo ratings yet
- Diptiman Paramedical College and Hospital PresentationDocument47 pagesDiptiman Paramedical College and Hospital PresentationDharmaNo ratings yet
- Benefits at A Glance: TexasDocument10 pagesBenefits at A Glance: Texasakula_rupeshNo ratings yet
- Star Health Network Hospitals in NagpurDocument4 pagesStar Health Network Hospitals in NagpurNitinNo ratings yet
- Patient Health Questionnaire 9Document2 pagesPatient Health Questionnaire 9Mona NathNo ratings yet
- Facilitators and Barriers That Transfemoral Amputees Experience in Their Everyday LifeDocument8 pagesFacilitators and Barriers That Transfemoral Amputees Experience in Their Everyday LifeJuciara MouraNo ratings yet
- BMHP CSSD Data Usage 2019Document4 pagesBMHP CSSD Data Usage 2019Handri GumelarNo ratings yet
- Ys%, XLD M Dka S%L Iudcjd Ckrcfha .Eiü M %H: The Gazette of The Democratic Socialist Republic of Sri LankaDocument31 pagesYs%, XLD M Dka S%L Iudcjd Ckrcfha .Eiü M %H: The Gazette of The Democratic Socialist Republic of Sri LankaSanaka LogesNo ratings yet
- Overview of Indian Pharmaceutical Industry: A Project Report ONDocument65 pagesOverview of Indian Pharmaceutical Industry: A Project Report ONsanjana seth100% (1)
- Simulateur BekerDocument9 pagesSimulateur Bekerahmed larefNo ratings yet
- East Avenue Medical Center Burn Unit Provides Haven for PatientsDocument2 pagesEast Avenue Medical Center Burn Unit Provides Haven for PatientsDanilo Siquig Jr.No ratings yet
- Steps To Enter An Aged Care HomeDocument36 pagesSteps To Enter An Aged Care HomeSimran SekhonNo ratings yet
- Access Fast Fact 2019Document46 pagesAccess Fast Fact 2019see naaNo ratings yet
- Monitoring and Evaluating A Voluntary Blood Donation ProgramDocument16 pagesMonitoring and Evaluating A Voluntary Blood Donation Programddophlaak labdeptNo ratings yet
- Apotek Exonero Stok Obat TersisaDocument5 pagesApotek Exonero Stok Obat TersisaAprilia SilmiNo ratings yet
- Daftar Alat Berdasarkan ResikoDocument28 pagesDaftar Alat Berdasarkan ResikoLia MarliaNo ratings yet
- I N TR A V Enou S Cannul A Tion: OSC E ChecklistDocument2 pagesI N TR A V Enou S Cannul A Tion: OSC E ChecklistMostafa ShabanNo ratings yet
- Rebirth CBD Gummies CanadaDocument4 pagesRebirth CBD Gummies CanadabettytlutssNo ratings yet
- Sensitivity: InternalDocument1 pageSensitivity: Internalanon_588636119No ratings yet
- FRACTURAS DE PILON TIBIAL (Autoguardado)Document49 pagesFRACTURAS DE PILON TIBIAL (Autoguardado)laloNo ratings yet
- Ms. MantillaDocument3 pagesMs. MantillaJames Elwood DoyolaNo ratings yet
- Basic Research Laboratory and Survey of Medicinal PlantsDocument39 pagesBasic Research Laboratory and Survey of Medicinal PlantsmadhubalaNo ratings yet
- Affidavit For Un Employed PharmacistDocument1 pageAffidavit For Un Employed Pharmacistsudheer kollaNo ratings yet
- Dialogue Bed Bath Apr 2021Document2 pagesDialogue Bed Bath Apr 2021Gde UsadhaNo ratings yet
- SC Auto SurgDocument5 pagesSC Auto SurgBen Haim nanlonyNo ratings yet
- JOINS Keperawatan B 4Document5 pagesJOINS Keperawatan B 4Laila nurhafizahNo ratings yet
- EMA-HMPC-228759. Assessment Report On Senna Alexandrina Mill. (Cassia Senna L. Cassia Angustifolia Vahl) Folium and Fructus, 2016Document123 pagesEMA-HMPC-228759. Assessment Report On Senna Alexandrina Mill. (Cassia Senna L. Cassia Angustifolia Vahl) Folium and Fructus, 2016Maikel Perez NavarroNo ratings yet
- Emergency Meeting Information Memo 11092021Document2 pagesEmergency Meeting Information Memo 11092021NEWS CENTER MaineNo ratings yet
- WCA2024 - George Export - Labour AnalgesiaDocument55 pagesWCA2024 - George Export - Labour AnalgesiaSyahrul Mubarak Danar SumantriNo ratings yet