You might also like
- To Diagnose Stage 1 and Early Stage 2 CKD To Diagnose More Advanced CKD (Late Stage 2-4)Document1 pageTo Diagnose Stage 1 and Early Stage 2 CKD To Diagnose More Advanced CKD (Late Stage 2-4)andreisandorNo ratings yet
- Diagnosing, Staging, and Treating Chronic Kidney Disease in Dog and CatsDocument4 pagesDiagnosing, Staging, and Treating Chronic Kidney Disease in Dog and CatsXenia FernandezNo ratings yet
- IRIS Pocket Guide To CKD 2023Document3 pagesIRIS Pocket Guide To CKD 2023CheyenneNo ratings yet
- IRIS Pocket Guide To CKD PDFDocument3 pagesIRIS Pocket Guide To CKD PDFJMilena2028No ratings yet
- IRIS Staging of CKD Modified 2019 PDFDocument5 pagesIRIS Staging of CKD Modified 2019 PDFJMilena2028No ratings yet
- Staging of CKD Based On Blood Creatinine Concentration: Mol/l MG/DLDocument5 pagesStaging of CKD Based On Blood Creatinine Concentration: Mol/l MG/DLLINDA BELMONTNo ratings yet
- 2 IRIS Staging of CKD 2023Document5 pages2 IRIS Staging of CKD 2023jhumira perez de la oNo ratings yet
- Insuf Renala - Trat in FCT de stadiuAUTHORPDFDocument12 pagesInsuf Renala - Trat in FCT de stadiuAUTHORPDFGrădinariu ViorelNo ratings yet
- Lab Evaluation Dogs Cats CKIDocument5 pagesLab Evaluation Dogs Cats CKIDarija LausNo ratings yet
- 003 5559.001 Iris Website Staging of CKD PDF 220116 FinalDocument9 pages003 5559.001 Iris Website Staging of CKD PDF 220116 FinalFuzti FauziaNo ratings yet
- Intro Kidney Test-Sdma TestDocument2 pagesIntro Kidney Test-Sdma TestWiekeS JuneNo ratings yet
- Diagnosing & Staging of Chronic Kidney Disease - WSAVA2009 - VINDocument5 pagesDiagnosing & Staging of Chronic Kidney Disease - WSAVA2009 - VINAnchang Don MaximNo ratings yet
- Diabetes ManagementDocument44 pagesDiabetes ManagementRahaf AlhubailNo ratings yet
- AKI Vs CKD Lecture Latest 3rd Dec 2018Document51 pagesAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessNo ratings yet
- MSU-IIT Nursing Student's Pharmacological Study of AmiodaroneDocument4 pagesMSU-IIT Nursing Student's Pharmacological Study of AmiodaroneBianca Mikaela DosdosNo ratings yet
- 1406b1f8cc PDFDocument1 page1406b1f8cc PDFAs RifahNo ratings yet
- Chronic Kidney Disease: For The Primary Care PhysicianDocument54 pagesChronic Kidney Disease: For The Primary Care PhysicianFlavia PolodeanuNo ratings yet
- K9 Kidney DiseaseDocument6 pagesK9 Kidney DiseaseKitch MallariNo ratings yet
- Detect Liver Disease with Liver Function TestsDocument15 pagesDetect Liver Disease with Liver Function TestsBishal JB KunworNo ratings yet
- Chronic Renal FailureDocument7 pagesChronic Renal Failuretantalizin marieNo ratings yet
- Idexx Sdma Test Algorithm PDFDocument2 pagesIdexx Sdma Test Algorithm PDFblueice999No ratings yet
- Capitle - Drug Study 2Document3 pagesCapitle - Drug Study 2Mary DeniseNo ratings yet
- IRIS-DOG-Treatment Recommendations 2023Document17 pagesIRIS-DOG-Treatment Recommendations 2023jhumira perez de la oNo ratings yet
- BUN and Creatinine LevelsDocument2 pagesBUN and Creatinine LevelsRadityo Galih PermadiNo ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- CH 071 Acute Kidney Injury in ChildrenDocument9 pagesCH 071 Acute Kidney Injury in Childrenarun babuNo ratings yet
- AKI Perioperatif 3Document6 pagesAKI Perioperatif 3Kevin JohanesNo ratings yet
- Penunjang Pemeriksaan KlinisDocument88 pagesPenunjang Pemeriksaan Klinisgrady_christian_9720No ratings yet
- Davao Doctors College Nursing Program Progress NotesDocument17 pagesDavao Doctors College Nursing Program Progress NotesABBEYGALE JOYHN GALANNo ratings yet
- NCP MS Ward 2ND RotationDocument2 pagesNCP MS Ward 2ND RotationIvan Jules P. PALMARESNo ratings yet
- NCP Online PortfolioDocument10 pagesNCP Online Portfolioapi-351011524No ratings yet
- Cushing's Disease PathophysiologyDocument3 pagesCushing's Disease PathophysiologyAj MacotoNo ratings yet
- Methadone HCLDocument2 pagesMethadone HCLtiffanald100% (1)
- Drug Study of FurosemideDocument5 pagesDrug Study of FurosemideAntonette Lei100% (1)
- Background ConclusionDocument70 pagesBackground ConclusionResa Shahana UlfaNo ratings yet
- Swift River Medication AdministrationDocument4 pagesSwift River Medication AdministrationmattNo ratings yet
- Drug Study 1Document3 pagesDrug Study 1G4 AMOYO ANGELICA NICOLENo ratings yet
- Chronic Kidney Disease: Diagnosis and TherapyDocument21 pagesChronic Kidney Disease: Diagnosis and TherapyLindsNo ratings yet
- RFT Theory NotesDocument13 pagesRFT Theory NotesammuNo ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- Parameter Penyakit Ginjal Kronis PentingDocument16 pagesParameter Penyakit Ginjal Kronis PentingMahdawwNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticeErwin SiahaanNo ratings yet
- Post Covid 13.12Document13 pagesPost Covid 13.12ram krishnaNo ratings yet
- Post COVID follow up guidelinesDocument13 pagesPost COVID follow up guidelinesHumas PDPINo ratings yet
- Non-Protein Nitrogen Compounds1 (FINALS)Document60 pagesNon-Protein Nitrogen Compounds1 (FINALS)Marydith Ortillo100% (1)
- CRFDocument27 pagesCRFNatalie WNo ratings yet
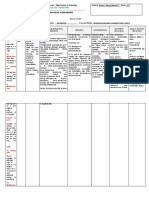
- College of Nursing and Midwifery: Mabini Colleges Daet, Camarines NorteDocument1 pageCollege of Nursing and Midwifery: Mabini Colleges Daet, Camarines NorteMa. Sheenadel ZamudioNo ratings yet
- Simpo 3 - Dr. Bowo SP - pd-kEMD - How TPatients With Co-Formulation InsulinDocument35 pagesSimpo 3 - Dr. Bowo SP - pd-kEMD - How TPatients With Co-Formulation InsulinAgnes Irene ZagotoNo ratings yet
- Living Donor Kidney Transplantation - Jonathon Oldsburgh - UOM 21.8.19Document106 pagesLiving Donor Kidney Transplantation - Jonathon Oldsburgh - UOM 21.8.19Renal Association MauritiusNo ratings yet
- Reports Weakness, and Flu-Like Symptom For 3-4 DaysDocument2 pagesReports Weakness, and Flu-Like Symptom For 3-4 DaysAlliana Denice VicencioNo ratings yet
- NCPDocument2 pagesNCPJanelle Cabida Supnad100% (1)
- Cumbria and Lancs KCN Algorithm PDFDocument18 pagesCumbria and Lancs KCN Algorithm PDFratih83No ratings yet
- Jurnal Dr. Tri Hadi-29 Des 2021Document17 pagesJurnal Dr. Tri Hadi-29 Des 2021aldyNo ratings yet
- Emergency Renal Referral PathwayDocument3 pagesEmergency Renal Referral PathwayYadi SupriyadiNo ratings yet
- CKD Assessment Algorithm Identification and ReferralDocument1 pageCKD Assessment Algorithm Identification and ReferralSirsefti AnggiNo ratings yet
- Diagnosis and Management of Complete Kawasaki Disease in ChildrenDocument13 pagesDiagnosis and Management of Complete Kawasaki Disease in ChildrenJ SNo ratings yet
- Acute Kidney InjuryDocument5 pagesAcute Kidney InjuryisnaazmutNo ratings yet
- Chronic Kidney Disease Bhakti MuliaDocument24 pagesChronic Kidney Disease Bhakti MuliaCOVID RSHJNo ratings yet
- Clinical Diabetes Research: Methods and TechniquesFrom EverandClinical Diabetes Research: Methods and TechniquesMichael RodenNo ratings yet
- Stadializare IRISDocument1 pageStadializare IRISandreisandorNo ratings yet
- Idexx Sdma Test Algorithm PDFDocument2 pagesIdexx Sdma Test Algorithm PDFblueice999No ratings yet
- BBJ Product Card 2010Document2 pagesBBJ Product Card 2010blueice999No ratings yet
- Global Economic Crisis - Compiled by RuthvikDocument14 pagesGlobal Economic Crisis - Compiled by Ruthvikblueice999No ratings yet
- JE Rottw Judges Handbook 021108Document28 pagesJE Rottw Judges Handbook 021108blueice999No ratings yet
- Comparison of Alvarado Scores, Tzanakis Scores, and Ripasa Scores in The Diagnosis of Acute Appendicitis in Sanglah HospitalDocument6 pagesComparison of Alvarado Scores, Tzanakis Scores, and Ripasa Scores in The Diagnosis of Acute Appendicitis in Sanglah HospitalYosuaNo ratings yet
- Health Services ManagementDocument6 pagesHealth Services ManagementWanyonyi JustusNo ratings yet
- Developmental Difficulties in Early ChildhoodDocument120 pagesDevelopmental Difficulties in Early ChildhoodizzahtulNo ratings yet
- Dental Hygiene Resume - No ReferencesDocument2 pagesDental Hygiene Resume - No Referencesapi-313829416No ratings yet
- Enteral Tube Administration of Oral Chemotherapy DrugsDocument15 pagesEnteral Tube Administration of Oral Chemotherapy DrugsCoté HuertaNo ratings yet
- Infographic The Body As A Source of Big Data HealthIT InfographicDocument1 pageInfographic The Body As A Source of Big Data HealthIT InfographiciHT²100% (1)
- The Revised Cognitive Therapy Scale (CTS-R) : Psychometric PropertiesDocument16 pagesThe Revised Cognitive Therapy Scale (CTS-R) : Psychometric PropertiesCarolina UriarteNo ratings yet
- Biopharmaceutical Biopharmaceutical: Manufacturing Powerhouse ? Manufacturing Powerhouse ?Document2 pagesBiopharmaceutical Biopharmaceutical: Manufacturing Powerhouse ? Manufacturing Powerhouse ?Andy KurniawanNo ratings yet
- A. Historical Perspectives: Women's RolesDocument11 pagesA. Historical Perspectives: Women's RolesJoanne SarzonaNo ratings yet
- Letter of Recommendation For Patience Bekoe 1Document2 pagesLetter of Recommendation For Patience Bekoe 1api-302400912No ratings yet
- Intestinal Obstruction in ChildrenDocument63 pagesIntestinal Obstruction in Childreng1381821No ratings yet
- Health 10 - Q2 - WK5Document2 pagesHealth 10 - Q2 - WK5graceNo ratings yet
- Barret's Syndrome Case ReportDocument3 pagesBarret's Syndrome Case ReportResearch ParkNo ratings yet
- Regenics Pitch DeckDocument32 pagesRegenics Pitch DeckGrayson MillerNo ratings yet
- History of CounsellingDocument7 pagesHistory of Counsellingsam sangeethNo ratings yet
- Assignment-I Business Statistics: TOPIC: Abbott India LTDDocument14 pagesAssignment-I Business Statistics: TOPIC: Abbott India LTDAbhishek MohanpuriaNo ratings yet
- Module 7 Mental Health and Well-Being in Middle and Late AdolescenceDocument22 pagesModule 7 Mental Health and Well-Being in Middle and Late AdolescenceFaith CubillaNo ratings yet
- Health Benefits of CucumbersDocument6 pagesHealth Benefits of Cucumbersver_at_workNo ratings yet
- SOP Feedback Management and Customer Com-PlaintsDocument4 pagesSOP Feedback Management and Customer Com-Plaintslune assongmoNo ratings yet
- Juvenile DelinquencyDocument34 pagesJuvenile Delinquencyjihan latifahNo ratings yet
- ANE BelakangDocument3 pagesANE BelakangGustomo PanantroNo ratings yet
- Margolin GR 11 NegDocument22 pagesMargolin GR 11 NegbhupatinNo ratings yet
- Forensic Aspects of Consultation-Liaison PsychiatryDocument88 pagesForensic Aspects of Consultation-Liaison PsychiatryRaul GrapilonNo ratings yet
- Doh ProgramsDocument45 pagesDoh ProgramsVon Andre AposagaNo ratings yet
- A IsopathyDocument49 pagesA IsopathygoharNo ratings yet
- Bella Bolla - PrintInspectionDocument1 pageBella Bolla - PrintInspectionBryce AirgoodNo ratings yet
- Hyperbilirubinemia (Gerardo, Maria Maricar P)Document11 pagesHyperbilirubinemia (Gerardo, Maria Maricar P)Carlojay IniegoNo ratings yet
- Module 7: Stating The Biopsychosocial Theories of Crime CausationDocument13 pagesModule 7: Stating The Biopsychosocial Theories of Crime CausationNADAL NICA JOY L.100% (1)
- Hormonal TherapiesDocument39 pagesHormonal TherapiesJalal EltabibNo ratings yet
- Enc 1102 ReasearchdfinalDocument9 pagesEnc 1102 Reasearchdfinalapi-507725488No ratings yet