You might also like
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Osteotomia Smith Petersen Original 1945Document11 pagesOsteotomia Smith Petersen Original 1945Traian UrsuNo ratings yet
- NCM 116 - PERCEPTION AND COORDINATION Musculoskeletal Part 2 Ms. Gayatin PDFDocument23 pagesNCM 116 - PERCEPTION AND COORDINATION Musculoskeletal Part 2 Ms. Gayatin PDFGabrielle Frances FernandezNo ratings yet
- Abrasion Arthroplasty Promotes Improvement of DegeDocument6 pagesAbrasion Arthroplasty Promotes Improvement of Degeestefania1994No ratings yet
- Molecular Basis of AgingDocument17 pagesMolecular Basis of Agingey_mieNo ratings yet
- Adobe Scan Apr 22, 2024 (L)Document12 pagesAdobe Scan Apr 22, 2024 (L)mayainst2022No ratings yet
- Treating Bone Deformities With Circular External Skeletal FixationDocument10 pagesTreating Bone Deformities With Circular External Skeletal Fixationtaner_soysurenNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- LID201112052004Document10 pagesLID201112052004Gia BảoNo ratings yet
- Artroplastia Partiala de Sold Tip Austin MooreDocument9 pagesArtroplastia Partiala de Sold Tip Austin MooreMyhay CretzuNo ratings yet
- Osteochondral Lesions of The Knee Differentiating The Most Common Entities at MRI ODLICNODocument18 pagesOsteochondral Lesions of The Knee Differentiating The Most Common Entities at MRI ODLICNOdrbane123No ratings yet
- Metabolic Bone DiseaseDocument6 pagesMetabolic Bone Diseasekartini ciatawiNo ratings yet
- Bone Remodelling: Scientific SectionDocument7 pagesBone Remodelling: Scientific SectionRohini TondaNo ratings yet
- Journal of Orthopaedic Science: Hidenori Matsubara, Hiroyuki TsuchiyaDocument8 pagesJournal of Orthopaedic Science: Hidenori Matsubara, Hiroyuki TsuchiyaNeta Aza MaineztNo ratings yet
- The Enthesis: A Review of The Tendon-To-Bone InsertionDocument10 pagesThe Enthesis: A Review of The Tendon-To-Bone InsertionLuis Briones Lau.LiNo ratings yet
- Recent Advances in The Pathogenesis and Treatment of OsteoporosisDocument5 pagesRecent Advances in The Pathogenesis and Treatment of OsteoporosisAnil JohnNo ratings yet
- Osseointegration and Bone BiologyDocument29 pagesOsseointegration and Bone BiologyHarini PadmanabhanNo ratings yet
- 2010 Miniscrew Assisted Nonsurgical PalatalDocument10 pages2010 Miniscrew Assisted Nonsurgical PalatalMariana SantosNo ratings yet
- Radiography in Osteoporosis: Sivasubramanian Srinivasan and Wilfred C. G. PehDocument16 pagesRadiography in Osteoporosis: Sivasubramanian Srinivasan and Wilfred C. G. PehAdriana NavaNo ratings yet
- Os 1 251Document7 pagesOs 1 251mukhlis akmalNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Biology of Normal Bone Remodeling 2017Document5 pagesBiology of Normal Bone Remodeling 2017Amani FezaiNo ratings yet
- JIAP January 2010 - Summers' Technique Modification For Sinus Floor Elevation Using A Connective Tissue Graft. A Case Report.Document4 pagesJIAP January 2010 - Summers' Technique Modification For Sinus Floor Elevation Using A Connective Tissue Graft. A Case Report.Dr. Silviu Andrei ConstantinescuNo ratings yet
- Srugical Treatment of Complex Meniscus Tear and DiseaseDocument11 pagesSrugical Treatment of Complex Meniscus Tear and DiseaseEfrain RodrigoNo ratings yet
- The Knife-Edge Tendency in Mandibular Residual Ridges in WomenDocument7 pagesThe Knife-Edge Tendency in Mandibular Residual Ridges in WomenSyed Abdul BasitNo ratings yet
- Complex Surgical Treatment of Non-United Fractures and False Joints of The FemurDocument12 pagesComplex Surgical Treatment of Non-United Fractures and False Joints of The FemurCentral Asian StudiesNo ratings yet
- Knee Potential RisksDocument84 pagesKnee Potential RisksAnil Chowadary Anil ChowadaryNo ratings yet
- The Osteocyte: From "Prisoner" To "Orchestrator": Carla Palumbo and Marzia FerrettiDocument17 pagesThe Osteocyte: From "Prisoner" To "Orchestrator": Carla Palumbo and Marzia FerrettiNadira NurinNo ratings yet
- Osteopathia Striata With Concomitant Fibroblastic Osteosarcoma of The Femur A Potential Malignant Risk 2472 016X 1000104Document4 pagesOsteopathia Striata With Concomitant Fibroblastic Osteosarcoma of The Femur A Potential Malignant Risk 2472 016X 1000104ritvikNo ratings yet
- Material and Nanomechanical Properties of Bone Structural Units of - 2022 - BoneDocument12 pagesMaterial and Nanomechanical Properties of Bone Structural Units of - 2022 - BoneGeorgiana BunghiuzNo ratings yet
- JCM 11 06434 v2Document17 pagesJCM 11 06434 v2NeelamNo ratings yet
- Percutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDocument7 pagesPercutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDouglas PrinaNo ratings yet
- Cellular Mechanisms of Bone RemodelingDocument9 pagesCellular Mechanisms of Bone RemodelingSilvia AlexandraNo ratings yet
- t3 Som 2014 2Document14 pagest3 Som 2014 2Julio AbarzuaNo ratings yet
- Osteoporosis: Pathophysiolog YDocument42 pagesOsteoporosis: Pathophysiolog YShared LifeNo ratings yet
- Toorthj 9 463Document12 pagesToorthj 9 463Jaume SanahujaNo ratings yet
- Research and Education: Section EditorDocument12 pagesResearch and Education: Section EditorMayra Ortiz HerreraNo ratings yet
- Melsen2007 PDFDocument14 pagesMelsen2007 PDFMarcelinoFernandezNo ratings yet
- Journal of Biomechanics: Petr Marcián, Libor Borák, Ji Ří Valášek, Jozef Kaiser, Zden Ěk Florian, Jan WolffDocument7 pagesJournal of Biomechanics: Petr Marcián, Libor Borák, Ji Ří Valášek, Jozef Kaiser, Zden Ěk Florian, Jan WolffAmrita FrancisNo ratings yet
- Computerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersDocument11 pagesComputerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersMasithaNo ratings yet
- Jurnal Fraktur TibiaDocument8 pagesJurnal Fraktur TibiaAnggi CalapiNo ratings yet
- NatlJMaxillofacSurg22120-6243637 172036Document9 pagesNatlJMaxillofacSurg22120-6243637 172036HARITHA H.PNo ratings yet
- 10 1097@SCS 0000000000003839Document3 pages10 1097@SCS 0000000000003839gustavo manzanedo carbajalNo ratings yet
- 179-Article Text-302-1-10-20171121 PDFDocument5 pages179-Article Text-302-1-10-20171121 PDFMichael XuNo ratings yet
- Osteomielitis PatelarDocument3 pagesOsteomielitis PatelarAlexander DanielNo ratings yet
- Fai 2009 0142Document8 pagesFai 2009 0142Mohamed GoudaNo ratings yet
- PIIS0030589809000881Document12 pagesPIIS0030589809000881dr. Joko WibowoNo ratings yet
- Biología Celular Metabolismo OseoDocument12 pagesBiología Celular Metabolismo Oseoandreaelisa17No ratings yet
- 2Document7 pages2Narito NianNo ratings yet
- Perez Et Al. - 2018 - Tissue Engineering and Cell-Based Therapies For Fractures and Bone DefectsDocument23 pagesPerez Et Al. - 2018 - Tissue Engineering and Cell-Based Therapies For Fractures and Bone DefectsAlif FakhriNo ratings yet
- To - Fraktur Mandibula IdealDocument70 pagesTo - Fraktur Mandibula IdealHayu Lesya PutriNo ratings yet
- Vertebroplasty and Kyphoplasty For The Treatment.6Document12 pagesVertebroplasty and Kyphoplasty For The Treatment.6cooperorthopaedicsNo ratings yet
- Alveolar Distraction Osteogenesis and ImplantologyDocument4 pagesAlveolar Distraction Osteogenesis and ImplantologyIJAR JOURNALNo ratings yet
- Advances in Magnetic Resonance Imaging Of.5Document10 pagesAdvances in Magnetic Resonance Imaging Of.5cooperorthopaedicsNo ratings yet
- jkhs-21-202 Ko enDocument9 pagesjkhs-21-202 Ko enlaurenNo ratings yet
- Osteoid Osteoma and Osteoblastoma: Review ArticleDocument12 pagesOsteoid Osteoma and Osteoblastoma: Review ArticleAnggi MartaNo ratings yet
- Bone Loss 2021Document27 pagesBone Loss 2021NexelsNo ratings yet
- Stem Cell and OrthodonticsDocument13 pagesStem Cell and OrthodonticsJhon EstupiñanNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- PIIS0031395514001801Document2 pagesPIIS0031395514001801DavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
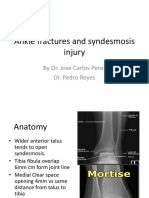
- Ankle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDocument11 pagesAnkle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDavidBeatonComuladaNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Rheumatoid Hand and Wrist Surgery Soft Tissue.99323Document9 pagesRheumatoid Hand and Wrist Surgery Soft Tissue.99323DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Panel Chss 2016Document57 pagesPanel Chss 2016Amit PatelNo ratings yet
- Surgical Site Marking Protocols and PolicyDocument8 pagesSurgical Site Marking Protocols and PolicyVitria Sari DewiNo ratings yet
- Provider Number Provider NameDocument14 pagesProvider Number Provider NameSara RaiNo ratings yet
- Club FootDocument38 pagesClub FootNamakau MuliloNo ratings yet
- Stretchers, Mobile, HospitalDocument59 pagesStretchers, Mobile, HospitalLee ThoongNo ratings yet
- Balanced Suspension Skeletal TractionDocument4 pagesBalanced Suspension Skeletal Tractionfegerilene100% (1)
- Shoulder Arthroscopy, Anatomy and Variants - Part 1Document6 pagesShoulder Arthroscopy, Anatomy and Variants - Part 1Raluca CostandacheNo ratings yet
- The Privacy Isuues of AppleDocument7 pagesThe Privacy Isuues of Applephysicser15No ratings yet
- TELEMEDICINEDocument39 pagesTELEMEDICINEValarmathi100% (1)
- Daftar PustakaDocument3 pagesDaftar Pustakasusi candra winaNo ratings yet
- Link Download Ebook Gratis Anesthesiology and Intensive CareDocument10 pagesLink Download Ebook Gratis Anesthesiology and Intensive CarearifNo ratings yet
- John Olson-Job 20 Report 2Document3 pagesJohn Olson-Job 20 Report 2api-406063178No ratings yet
- Nursing Intervention (Risk For Trauma) RationaleDocument5 pagesNursing Intervention (Risk For Trauma) RationaleJay VillasotoNo ratings yet
- Introduction To Clubfoot - PhysiopediaDocument13 pagesIntroduction To Clubfoot - PhysiopediavaishnaviNo ratings yet
- Hand Therapy Brochure PDFDocument12 pagesHand Therapy Brochure PDFPrioteasa RaduNo ratings yet
- Synthes LCPDocument24 pagesSynthes LCPRoubeel KPNo ratings yet
- Kick Off Plan Health Pack 2020Document22 pagesKick Off Plan Health Pack 2020Aneesh PrabhakaranNo ratings yet
- Design & Development of C Arm X Ray SystemDocument5 pagesDesign & Development of C Arm X Ray Systemswapnil pandeNo ratings yet
- Basilar Invagination - C1-C2 DistractionDocument6 pagesBasilar Invagination - C1-C2 DistractionSri Vijay Anand K SNo ratings yet
- NW0508 Rev D 6875 Hana Owners Manual - enDocument77 pagesNW0508 Rev D 6875 Hana Owners Manual - enRonald ThorpeNo ratings yet
- Mayo CurveDocument6 pagesMayo CurveDanielle Marie SimoraNo ratings yet
- QUALITY Indicator 5th EditionDocument6 pagesQUALITY Indicator 5th EditionPrabhat Kumar89% (18)
- Jewett and Cash BraceDocument19 pagesJewett and Cash BraceucssNo ratings yet
- Overseas Student Health Cover SA S 20230522 131410Document3 pagesOverseas Student Health Cover SA S 20230522 131410vishavkhaira6027No ratings yet
- There Are 14 Types of Surgeons Recognized by The American College of Surgeons AreDocument2 pagesThere Are 14 Types of Surgeons Recognized by The American College of Surgeons AreAurea Jasmine DacuycuyNo ratings yet
- Case Study#5: March 7th, 2017Document17 pagesCase Study#5: March 7th, 2017Joaquín Norambuena EscalonaNo ratings yet
- DCS & DHS PDFDocument34 pagesDCS & DHS PDFMyhay Cretzu100% (1)
- Jurnal Problem Foot ChildrenDocument5 pagesJurnal Problem Foot ChildrenAbu Bakar SiddiqNo ratings yet
- Jurnal Ortho 12Document4 pagesJurnal Ortho 12Santika IndahsariNo ratings yet
- Ejercicio: Choose The Best Answer. What Do You Do?Document4 pagesEjercicio: Choose The Best Answer. What Do You Do?LenNo ratings yet