You might also like
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportFrom EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNo ratings yet
- Fast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaFrom EverandFast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaNo ratings yet
- Diseases of The Bone Marrow and Blood Conditions That Can Occur When The Blood-Forming Cells in The Bone Marrow Become AbnormalDocument4 pagesDiseases of The Bone Marrow and Blood Conditions That Can Occur When The Blood-Forming Cells in The Bone Marrow Become AbnormalLuqman QadirNo ratings yet
- Myeloproliferative DisorderDocument36 pagesMyeloproliferative DisorderKalpana ShahNo ratings yet
- Myeloproliferative Disorders 18th Oct 2010Document62 pagesMyeloproliferative Disorders 18th Oct 2010saint5470No ratings yet
- Hemafinals 02Document27 pagesHemafinals 02Clarence SantosNo ratings yet
- Leukemias, Lymphomas, MyelomaDocument45 pagesLeukemias, Lymphomas, MyelomaYesyNo ratings yet
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Leukemia Lymphoma Skin Cancer - RubioDocument22 pagesLeukemia Lymphoma Skin Cancer - Rubiochristian pulmonesNo ratings yet
- Drowsiness Lethargy Tiredness Malaise Listlessness Weakness Muscular WeaknessDocument4 pagesDrowsiness Lethargy Tiredness Malaise Listlessness Weakness Muscular WeaknessCiariz CharisseNo ratings yet
- Pathophysiology of Anemia and Polycythemia Pathophysiology of Anemia and Polycythemia Pathophysiology of Anemia and PolycythemiaDocument48 pagesPathophysiology of Anemia and Polycythemia Pathophysiology of Anemia and Polycythemia Pathophysiology of Anemia and PolycythemiaSrishti GoenkaNo ratings yet
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Chronic Leukaemia 111Document15 pagesChronic Leukaemia 111Razib HasanNo ratings yet
- Aematology: Col Kamran AfzalDocument32 pagesAematology: Col Kamran AfzalZaraNo ratings yet
- CBC 150106153749 Conversion Gate02Document44 pagesCBC 150106153749 Conversion Gate02KhetanNo ratings yet
- Introduction To HematologyDocument23 pagesIntroduction To HematologyReba PhiliposeNo ratings yet
- OSPE (Hematology)Document19 pagesOSPE (Hematology)Taha100% (1)
- C B C I: Omplete Lood Ount NterpretationsDocument44 pagesC B C I: Omplete Lood Ount NterpretationsridhoniNo ratings yet
- Chronic Myeloid LeukaemiaDocument27 pagesChronic Myeloid Leukaemiaنواف الزهرانيNo ratings yet
- Platelet: Muhammad Nazarudin, S.STDocument15 pagesPlatelet: Muhammad Nazarudin, S.STFafha FafhaNo ratings yet
- Bleeding DisordersDocument137 pagesBleeding DisordersJosiah BimabamNo ratings yet
- Hematology 3 1 The Red Blood CellDocument25 pagesHematology 3 1 The Red Blood Cellpieterinpretoria391No ratings yet
- Trombositopenia Dan TrombositosisDocument33 pagesTrombositopenia Dan TrombositosisAim AimmaNo ratings yet
- Quiz YourselfDocument154 pagesQuiz YourselfKandykane05100% (1)
- Hemolytic AnaemiaDocument60 pagesHemolytic AnaemiaAthul GurudasNo ratings yet
- 2007 Nov 07 CompleteDocument62 pages2007 Nov 07 CompleteKay BristolNo ratings yet
- S0850alug 1670953860959-SEU HDocument56 pagesS0850alug 1670953860959-SEU HAziz KhwajaNo ratings yet
- Myeloproliferative Disorders (Bhs Inggris)Document57 pagesMyeloproliferative Disorders (Bhs Inggris)Denny DedenNo ratings yet
- Hematology Review 2021-2Document142 pagesHematology Review 2021-2Maram AbdullahNo ratings yet
- 01 Hemotological MalignaciesDocument92 pages01 Hemotological MalignaciesmarrymbigiNo ratings yet
- Acute and Chronic Leukemia FinalDocument68 pagesAcute and Chronic Leukemia FinalHannah LeiNo ratings yet
- SBRC HematologyOncology 2Document80 pagesSBRC HematologyOncology 2dalia khamoNo ratings yet
- Hemostasis - Hematology BlockDocument40 pagesHemostasis - Hematology BlockamandaNo ratings yet
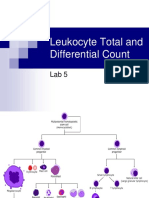
- Leukocyte Total and Differential CountDocument37 pagesLeukocyte Total and Differential CountHend HamedNo ratings yet
- Myeloid Neoplastic Disorders SummaryDocument5 pagesMyeloid Neoplastic Disorders SummaryNoor AlsheikhNo ratings yet
- Myeloproliferative Extra NotesDocument5 pagesMyeloproliferative Extra NotesRashed ShatnawiNo ratings yet
- Chronic Leukemia: Carlos Alfredo Cedeño RodríguezDocument24 pagesChronic Leukemia: Carlos Alfredo Cedeño RodríguezCarlos CedeñoNo ratings yet
- Myeloproliferative Disorders: Classification CML AMM PV ETDocument58 pagesMyeloproliferative Disorders: Classification CML AMM PV ETashuNo ratings yet
- Peripheral Smear Examination PDFDocument91 pagesPeripheral Smear Examination PDFtufis02No ratings yet
- Acute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMDocument52 pagesAcute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMJamilNo ratings yet
- 39 LeukemiaDocument16 pages39 Leukemiakolusam beveeNo ratings yet
- Megaloblastic AnemiaDocument13 pagesMegaloblastic AnemiaManchlaNo ratings yet
- Myelodisplastic Syndrome, Reaksi Leukemoid, Multipel MielomaDocument57 pagesMyelodisplastic Syndrome, Reaksi Leukemoid, Multipel MielomaWindhaNo ratings yet
- LeukemiasDocument3 pagesLeukemiasAli TARARNo ratings yet
- Plasma Cell DyscrasiasDocument10 pagesPlasma Cell DyscrasiasRazib HasanNo ratings yet
- Myeloproliferative Disorders (MPD) : Pathogenesis Clinical Laboratory FindingsDocument2 pagesMyeloproliferative Disorders (MPD) : Pathogenesis Clinical Laboratory FindingskakuNo ratings yet
- Gangguan TrombositDocument47 pagesGangguan TrombositLayli Nur ArniatiNo ratings yet
- Topic 6 - Anemia 1Document24 pagesTopic 6 - Anemia 1Vince Martin ManaigNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- Learnin ObjectiveDocument19 pagesLearnin ObjectivemadeNo ratings yet
- Interpreting Blood CountsDocument9 pagesInterpreting Blood CountsncetcsedeptNo ratings yet
- ThrombocytopeniaDocument49 pagesThrombocytopeniaMaria EnjelinaNo ratings yet
- Hem OncDocument26 pagesHem OncJim XieNo ratings yet
- Haemoglobinopathies 2Document53 pagesHaemoglobinopathies 2Igwe SolomonNo ratings yet
- Malignant Disorders of Leukocytes: Supachai A. Basit, RMT, PHDDocument109 pagesMalignant Disorders of Leukocytes: Supachai A. Basit, RMT, PHDChatie PipitNo ratings yet
- Hematology 1Document61 pagesHematology 1katz_hotchickNo ratings yet
- Laser: Light Amplification by Stimulated Emission RadiationDocument28 pagesLaser: Light Amplification by Stimulated Emission RadiationLuqman QadirNo ratings yet
- X RaysDocument18 pagesX RaysLuqman QadirNo ratings yet
- CT Scanner PDFDocument17 pagesCT Scanner PDFLuqman QadirNo ratings yet
- OPTICAL FIBER (Autosaved)Document16 pagesOPTICAL FIBER (Autosaved)Luqman QadirNo ratings yet
- Ultrasound Presentation PDFDocument35 pagesUltrasound Presentation PDFLuqman QadirNo ratings yet
- Correction of Errors. (Noun)Document3 pagesCorrection of Errors. (Noun)Luqman QadirNo ratings yet
- SteroidsDocument22 pagesSteroidsLuqman QadirNo ratings yet
- Sentence and Its TypeDocument4 pagesSentence and Its TypeLuqman QadirNo ratings yet
- Intravenous Anesthetic Agents: by Miss Maidah MehtabDocument49 pagesIntravenous Anesthetic Agents: by Miss Maidah MehtabLuqman QadirNo ratings yet
- Antibody Identification PenalDocument2 pagesAntibody Identification PenalLuqman QadirNo ratings yet
- Tao of Balanced Diet: Regular Food Diet For Health and BeautyDocument19 pagesTao of Balanced Diet: Regular Food Diet For Health and BeautyAnirudhNo ratings yet
- Chapter 8 THE RESPIRATORY SYSTEMDocument40 pagesChapter 8 THE RESPIRATORY SYSTEMAlexander Santiago Parel100% (2)
- Ebook Blood Transfusion Guideline PDFDocument170 pagesEbook Blood Transfusion Guideline PDFFazley Izuddin100% (1)
- 260 - 261, Tribhuvan Complex, Ishwar Nagar, New Delhi - 110 065Document10 pages260 - 261, Tribhuvan Complex, Ishwar Nagar, New Delhi - 110 065Prabhjot KaurNo ratings yet
- Alec Reed Academy: (Biology)Document101 pagesAlec Reed Academy: (Biology)Fifa GamerNo ratings yet
- 1311 shXB5HduNO4dGZIN couHH - zNB1UMk2KDocument2 pages1311 shXB5HduNO4dGZIN couHH - zNB1UMk2KRischard Beny RiswantoNo ratings yet
- Leukopenia and Bone Marrow TransplantationDocument20 pagesLeukopenia and Bone Marrow Transplantationdhanya jayanNo ratings yet
- Apollo Centers ListDocument11 pagesApollo Centers Listanon_275845789No ratings yet
- Indrawati Et Al. (2019)Document5 pagesIndrawati Et Al. (2019)wahyu putri setiawatiNo ratings yet
- 2013 - 10 - 2309 - 50 - 52BC-6800 - Communication Protocol - V2.0 - ENDocument123 pages2013 - 10 - 2309 - 50 - 52BC-6800 - Communication Protocol - V2.0 - ENcijep47636No ratings yet
- God's Healing Way (Secured)Document100 pagesGod's Healing Way (Secured)Antonio BernardNo ratings yet
- Activity Xi - Serum and Plasma PrepartionDocument3 pagesActivity Xi - Serum and Plasma PrepartionJorelle NogoyNo ratings yet
- Blood Donation 1Document10 pagesBlood Donation 1chhayaraviNo ratings yet
- Fluid Management & Blood Component Therapy: Key ConceptsDocument31 pagesFluid Management & Blood Component Therapy: Key ConceptsMohammad Pino HakimNo ratings yet
- Complete Blood Count (CBC) Normal Laboratory Study Values: DefinitionDocument6 pagesComplete Blood Count (CBC) Normal Laboratory Study Values: DefinitionGlare RhayneNo ratings yet
- English For Medicine Part 2 PDFDocument161 pagesEnglish For Medicine Part 2 PDFVictoria VintuNo ratings yet
- SVG CEE 2007 General PaperDocument16 pagesSVG CEE 2007 General PaperKNAH TutoringNo ratings yet
- LORESCA - BB Ratio Activity 2Document14 pagesLORESCA - BB Ratio Activity 2Kaycee Gretz LorescaNo ratings yet
- PhlebotomyDocument183 pagesPhlebotomyFadhli AhmadNo ratings yet
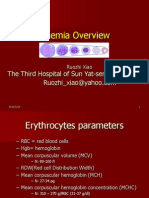
- Anemia Overview: The Third Hospital of Sun Yat-Sen UniversityDocument77 pagesAnemia Overview: The Third Hospital of Sun Yat-Sen UniversityMazlina MaidinNo ratings yet
- Unit 2 Biology and Geology 3rd ESODocument64 pagesUnit 2 Biology and Geology 3rd ESOPaulaNo ratings yet
- Haem Lecture 2.2016 PDFDocument12 pagesHaem Lecture 2.2016 PDFdorsa koraeiNo ratings yet
- Review Article: The Role of Thrombophilia in PregnancyDocument14 pagesReview Article: The Role of Thrombophilia in PregnancyTina GrosuNo ratings yet
- Bone Marrow Harvest Versus Peripheral Stem Cell CollectionDocument65 pagesBone Marrow Harvest Versus Peripheral Stem Cell CollectionJoBPNo ratings yet
- Thromboembolism in The Cat - WSAVA2005 - VINDocument8 pagesThromboembolism in The Cat - WSAVA2005 - VINPet Anjo DiademaNo ratings yet
- Platelets - The Lancet 2000Document9 pagesPlatelets - The Lancet 2000bluemleinNo ratings yet
- SOP Compatibility TestingDocument6 pagesSOP Compatibility Testingdavid mchembeNo ratings yet
- Biomedical Engineering Paper IIIDocument7 pagesBiomedical Engineering Paper IIINoor AhmedNo ratings yet
- 142 DefinitionsssDocument7 pages142 DefinitionsssAnonymous vXPYrefjGLNo ratings yet
- A Detailed Lesson Plan in Science 4Document10 pagesA Detailed Lesson Plan in Science 4Bella Mae Belle TaladuaNo ratings yet