You might also like
- A Memorandum for the President of the Royal Audiencia and Chancery Court of the City and Kingdom of GranadaFrom EverandA Memorandum for the President of the Royal Audiencia and Chancery Court of the City and Kingdom of GranadaNo ratings yet
- Su ND: Eft e E. FDocument3 pagesSu ND: Eft e E. FAlex ChenNo ratings yet
- Su ND: Item: ADocument8 pagesSu ND: Item: AHawkElseNo ratings yet
- Su ND: o o o o oDocument3 pagesSu ND: o o o o oAlex ChenNo ratings yet
- Su ND: ItemDocument3 pagesSu ND: ItemHawkElseNo ratings yet
- Ono Oano: / /min, /min /DL /MM'Document22 pagesOno Oano: / /min, /min /DL /MM'ايات عبدالرحمنNo ratings yet
- 23 Sur Deviated Nasal SeptumDocument3 pages23 Sur Deviated Nasal SeptumSardar jiNo ratings yet
- Su ND: Ly (/ /min, /minDocument3 pagesSu ND: Ly (/ /min, /minAlex ChenNo ratings yet
- LD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomDocument5 pagesLD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- 030 Med CytomegalovirusDocument5 pages030 Med CytomegalovirusArun Kumar ChaudharyNo ratings yet
- 142 Ped Cystic FibrosisDocument9 pages142 Ped Cystic FibrosisritaNo ratings yet
- 1 Q PDFDocument44 pages1 Q PDFMysheb SSNo ratings yet
- 144 Ped Foreign Body IngestionDocument3 pages144 Ped Foreign Body IngestionritaNo ratings yet
- R R R R R: M Sod M de Bo A E Ea M Ea E G Ase Meq Meq Meq MG MG D MG DDocument5 pagesR R R R R: M Sod M de Bo A E Ea M Ea E G Ase Meq Meq Meq MG MG D MG DMhmNo ratings yet
- HIRA For Stores ActivityDocument5 pagesHIRA For Stores ActivityRohit Singh100% (22)
- OmnixDocument1 pageOmnixKania LouisNo ratings yet
- 143 Ped DehydrationDocument4 pages143 Ped DehydrationritaNo ratings yet
- Air - Full ScoreDocument2 pagesAir - Full ScoreNader NaguiNo ratings yet
- Clones 3m1 OverdubDocument2 pagesClones 3m1 Overdubkeman91No ratings yet
- 0067 27Document5 pages0067 27Alex ChenNo ratings yet
- Risk Control Activities Contro L Catego RY Coso Components Control Attributes Control Classification TestingDocument7 pagesRisk Control Activities Contro L Catego RY Coso Components Control Attributes Control Classification TestingCaptain ObviousNo ratings yet
- 5mm PlateDocument1 page5mm PlateDeepak PawarNo ratings yet
- Format Nilai Gasal 2023-2024 - XiiDocument8 pagesFormat Nilai Gasal 2023-2024 - Xiikhoirulanam05No ratings yet
- Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SC2922)Document1 pageSilicon PNP Epitaxial Planar Transistor (Complement To Type 2SC2922)PETRONELA BADUNo ratings yet
- Form Checklist AC PDFDocument1 pageForm Checklist AC PDFSudar MawanNo ratings yet
- 2SB1647Document1 page2SB1647Julio barriosNo ratings yet
- Saxophun PartirureDocument7 pagesSaxophun PartirureadamNo ratings yet
- Non-Isothermal Reactor DesignDocument5 pagesNon-Isothermal Reactor Designnorpius7754No ratings yet
- General Walk-In Freezer Cálculo de Carga De: Temperatura Interna Temperatura ExternaDocument5 pagesGeneral Walk-In Freezer Cálculo de Carga De: Temperatura Interna Temperatura ExternaJair Cuesta GomezNo ratings yet
- Keuleneer Presentatie Waardebepaling NIVRADocument8 pagesKeuleneer Presentatie Waardebepaling NIVRAnalar22No ratings yet
- Overview Q595500Document1 pageOverview Q595500Asif Abbasov100% (1)
- Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SC5100)Document1 pageSilicon PNP Epitaxial Planar Transistor (Complement To Type 2SC5100)EdgarAlonsoNo ratings yet
- 029 00065 0 2sa1746Document1 page029 00065 0 2sa1746karimNo ratings yet
- DatasheetDocument1 pageDatasheetmixespirit73No ratings yet
- 0001 01 PDFDocument10 pages0001 01 PDFAmmar Al-basitiNo ratings yet
- R R R R R R: Q.LD: 2781 (Previous Ne T Lab Values Notes CalculatorDocument19 pagesR R R R R R: Q.LD: 2781 (Previous Ne T Lab Values Notes CalculatorMhmNo ratings yet
- 2SB1587 PDFDocument1 page2SB1587 PDFisaiasvaNo ratings yet
- Silicon PNP Epitaxial Planar Transistor: (Complement To Type 2SC2922)Document1 pageSilicon PNP Epitaxial Planar Transistor: (Complement To Type 2SC2922)busamawan wayanNo ratings yet
- ATS EngDocument1 pageATS EngOctavianus LinNo ratings yet
- Nilai Raport KLS Xi Upw 1 SMT 1Document16 pagesNilai Raport KLS Xi Upw 1 SMT 1artha wiriye negareNo ratings yet
- Nilai Raport KLS Xi Upw 1 SMT 2Document16 pagesNilai Raport KLS Xi Upw 1 SMT 2artha wiriye negareNo ratings yet
- FireNet Series Battery Calculator V3.057Document7 pagesFireNet Series Battery Calculator V3.057mujahid_islam85No ratings yet
- Before Exam SeeDocument4 pagesBefore Exam SeearpanpurkaitpersonalNo ratings yet
- pdf24 MergedDocument2 pagespdf24 MergedpriyaNo ratings yet
- Clones 1m1 OverdubDocument4 pagesClones 1m1 Overdubkeman91No ratings yet
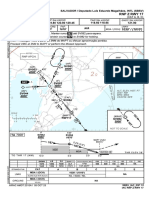
- SBSV Rnp-Z-Rwy-17 Iac 20231005Document1 pageSBSV Rnp-Z-Rwy-17 Iac 20231005Ulisses MalheirosNo ratings yet
- Neo Mob 601 001Document1 pageNeo Mob 601 001Edwin PrinceNo ratings yet
- 2SC2922Document1 page2SC2922zeckNo ratings yet
- Rac03 K PDFDocument6 pagesRac03 K PDFSimon AmplemanNo ratings yet
- Silicon NPN Epitaxial Planar Transistor (Complement To Type 2SA1860)Document1 pageSilicon NPN Epitaxial Planar Transistor (Complement To Type 2SA1860)ytnateNo ratings yet
- Response 9 ECC 2Document4 pagesResponse 9 ECC 2Steven HimawanNo ratings yet
- HW 12Document2 pagesHW 12haiNo ratings yet
- Rodrigo Gonçalves de Sousa - Two Movements For OrchestraDocument49 pagesRodrigo Gonçalves de Sousa - Two Movements For OrchestraRodrigo SousaNo ratings yet
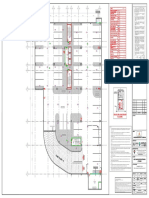
- CA01-L-ZL (84) 84CW95.001 - 3.0 - Isometric CA01-L-ZLDocument1 pageCA01-L-ZL (84) 84CW95.001 - 3.0 - Isometric CA01-L-ZLKreshna Wisnu BrataNo ratings yet
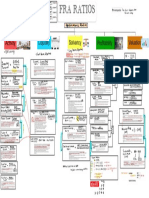
- Level 1 FRA Ratios 11Document1 pageLevel 1 FRA Ratios 11Duong TranNo ratings yet
- Tixf6 - : AlgebraDocument7 pagesTixf6 - : AlgebraShireen KiranNo ratings yet
- Clones 2m1aDocument8 pagesClones 2m1akeman91No ratings yet
- External Wiring: DVP04DA-S Arrangement of The TerminalsDocument2 pagesExternal Wiring: DVP04DA-S Arrangement of The Terminalsbebe_roalbaNo ratings yet
- Block 1Document22 pagesBlock 1ايات عبدالرحمنNo ratings yet
- Chemical Kinetics Mind MapDocument1 pageChemical Kinetics Mind MapSamridhi MoudgilNo ratings yet
- Vision TherapyDocument71 pagesVision TherapyXall143100% (1)
- Karl Avillo - MicrobiologyDocument16 pagesKarl Avillo - MicrobiologySanielle Karla Garcia LorenzoNo ratings yet
- Medical Emergencies: Oral & Maxillofacial Surgery 1Document7 pagesMedical Emergencies: Oral & Maxillofacial Surgery 1drpnnreddyNo ratings yet
- Calcium Metabolism: Presented by Ch. Likhita 1 Year P.GDocument113 pagesCalcium Metabolism: Presented by Ch. Likhita 1 Year P.GLikhita ChNo ratings yet
- The Effect of Skipping Rope Exercise On Physical and Cardiovascular Fitness Among Collegiate MalesDocument6 pagesThe Effect of Skipping Rope Exercise On Physical and Cardiovascular Fitness Among Collegiate MalesK. M. Junayed AhmedNo ratings yet
- Pathophysiology and Different Type of ShockDocument27 pagesPathophysiology and Different Type of Shockkhoulah hanifahNo ratings yet
- Emphysema: Presented By: Mis. M.K.Kaku Nursing TutorDocument10 pagesEmphysema: Presented By: Mis. M.K.Kaku Nursing TutorKaku ManishaNo ratings yet
- Horizontal Transmission P. Salmonis Wild Sub Antarctic Rainbow Trout Under Experimental ConditionsDocument12 pagesHorizontal Transmission P. Salmonis Wild Sub Antarctic Rainbow Trout Under Experimental Conditionsandres riofrioNo ratings yet
- MEHLMANMEDICAL Microbiology Assessment 1 1Document75 pagesMEHLMANMEDICAL Microbiology Assessment 1 1Feroz RaZa SoomrOoNo ratings yet
- Acute Tubular NecrosisDocument38 pagesAcute Tubular Necrosisganesa ekaNo ratings yet
- World Health Organization Updated COVID-19 Report-March 25Document12 pagesWorld Health Organization Updated COVID-19 Report-March 25CityNewsTorontoNo ratings yet
- NEET Test Series 2Document24 pagesNEET Test Series 2bal_thakreNo ratings yet
- CodesDocument19 pagesCodesAnonymous 6myGzJvANo ratings yet
- Coran - PS, 7th - Chapter 77 - Undescended Testis, Torsion, and VaricoceleDocument17 pagesCoran - PS, 7th - Chapter 77 - Undescended Testis, Torsion, and VaricoceleJessyMomoNo ratings yet
- What Is ApheresisDocument2 pagesWhat Is ApheresisRahma AlamNo ratings yet
- Imrad-ACG (AutoRecovered)Document5 pagesImrad-ACG (AutoRecovered)Zhanea VinsonNo ratings yet
- DR Putut B - Slide-Diagnostic Challenges in Functional Dyspepsia - (PIN PAPDI 2019) - PDFDocument24 pagesDR Putut B - Slide-Diagnostic Challenges in Functional Dyspepsia - (PIN PAPDI 2019) - PDFMuhammad Ahmad bin makruf syammakuNo ratings yet
- Nursing AssessmentDocument11 pagesNursing AssessmentStanford KerongoNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaReza Ridho PahleviNo ratings yet
- The Herbal Cure For Epilepsy: An: Review ArticleDocument6 pagesThe Herbal Cure For Epilepsy: An: Review ArticleNerissa AlvianaNo ratings yet
- Nursing Care Plan: Nursing Diagnosis Nursing Goals Nursing OutcomeDocument3 pagesNursing Care Plan: Nursing Diagnosis Nursing Goals Nursing OutcomemerryNo ratings yet
- Plant HormonesDocument2 pagesPlant HormonesMuhammad Noman BhattiNo ratings yet
- 3 Chemical Safety and Security Program - 3Document48 pages3 Chemical Safety and Security Program - 3Dessy NoorliaNo ratings yet
- Newsademic: The Informative Easy To Read Introduction To World NewsDocument20 pagesNewsademic: The Informative Easy To Read Introduction To World NewsStefcsik GáborNo ratings yet
- MPFL ReconstructionDocument16 pagesMPFL ReconstructiondrjorgewtorresNo ratings yet
- The Aga Khan University Hospital Pediatric SCU Course Final Exam Test Paper Name: - UnitDocument5 pagesThe Aga Khan University Hospital Pediatric SCU Course Final Exam Test Paper Name: - UnitUmar RashidNo ratings yet
- Pain Survey RevisedDocument10 pagesPain Survey RevisedSiva SankarNo ratings yet
- Suplementasi Vitamin D Pada Wanita Dengan: Polycystic Ovarian Syndrome (PCOS)Document9 pagesSuplementasi Vitamin D Pada Wanita Dengan: Polycystic Ovarian Syndrome (PCOS)Raihatil UmmiNo ratings yet
- Armed Forces Research Institute of Medical Sciences, 1960-2010Document30 pagesArmed Forces Research Institute of Medical Sciences, 1960-2010smith.kevin1420344No ratings yet
- IPDocument35 pagesIPxxsunflowerxxNo ratings yet