You might also like
- Personality Disorders: Behaviors That Are Drastically Different From The Norm. An Individual ExhibitsDocument13 pagesPersonality Disorders: Behaviors That Are Drastically Different From The Norm. An Individual Exhibitsishika mehrotraNo ratings yet
- Infectious Diseases of Central Nervous SystemDocument1,684 pagesInfectious Diseases of Central Nervous SystemLuciano ArraesNo ratings yet
- Clones 3m1 OverdubDocument2 pagesClones 3m1 Overdubkeman91No ratings yet
- 6 Vios / Yaris (Cont. Next Page) : Engine ControlDocument5 pages6 Vios / Yaris (Cont. Next Page) : Engine ControlHenryHutabaratNo ratings yet
- HIRA For Stores ActivityDocument5 pagesHIRA For Stores ActivityRohit Singh100% (22)
- Saxophun PartirureDocument7 pagesSaxophun PartirureadamNo ratings yet
- Level 2 Hospital Research WorkDocument25 pagesLevel 2 Hospital Research WorkRamces Soliman100% (1)
- 2008 - Neurofibromatoses - KaufmnanDocument203 pages2008 - Neurofibromatoses - KaufmnanPablo Antonio Antonio100% (1)
- Gynaecological Ultrasound in Clinical PracticeDocument247 pagesGynaecological Ultrasound in Clinical Practiceyulb_1100% (5)
- Shaukat Khanum Memorial Cancer Hospital & Research CentreDocument1 pageShaukat Khanum Memorial Cancer Hospital & Research Centrekhurram ijazNo ratings yet
- NP1 1Document13 pagesNP1 1Lyca Berin100% (1)
- Wss - Tonight - PianoDocument5 pagesWss - Tonight - Pianoliebenstock96No ratings yet
- Item:: 0. LD: 2777 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomDocument10 pagesItem:: 0. LD: 2777 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomHawkElseNo ratings yet
- Su ND: Eft e E. FDocument3 pagesSu ND: Eft e E. FAlex ChenNo ratings yet
- Su ND: o o o o oDocument3 pagesSu ND: o o o o oAlex ChenNo ratings yet
- 23 Sur Deviated Nasal SeptumDocument3 pages23 Sur Deviated Nasal SeptumSardar jiNo ratings yet
- Su ND: ItemDocument3 pagesSu ND: ItemHawkElseNo ratings yet
- Ono Oano: / /min, /min /DL /MM'Document22 pagesOno Oano: / /min, /min /DL /MM'ايات عبدالرحمنNo ratings yet
- Su ND: Ly (/ /min, /minDocument3 pagesSu ND: Ly (/ /min, /minAlex ChenNo ratings yet
- 142 Ped Cystic FibrosisDocument9 pages142 Ped Cystic FibrosisritaNo ratings yet
- 144 Ped Foreign Body IngestionDocument3 pages144 Ped Foreign Body IngestionritaNo ratings yet
- LD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomDocument5 pagesLD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- 030 Med CytomegalovirusDocument5 pages030 Med CytomegalovirusArun Kumar ChaudharyNo ratings yet
- 1 Q PDFDocument44 pages1 Q PDFMysheb SSNo ratings yet
- 143 Ped DehydrationDocument4 pages143 Ped DehydrationritaNo ratings yet
- Block 1Document22 pagesBlock 1ايات عبدالرحمنNo ratings yet
- 41Document3 pages41Kiên PhạmNo ratings yet
- Full Score LW 2017 Act 1 5.16Document7 pagesFull Score LW 2017 Act 1 5.16ethanNo ratings yet
- R R R R R: M Sod M de Bo A E Ea M Ea E G Ase Meq Meq Meq MG MG D MG DDocument5 pagesR R R R R: M Sod M de Bo A E Ea M Ea E G Ase Meq Meq Meq MG MG D MG DMhmNo ratings yet
- 0067 27Document5 pages0067 27Alex ChenNo ratings yet
- Ith in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsDocument6 pagesIth in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsAlex ChenNo ratings yet
- โพย EconoMidtermDocument2 pagesโพย EconoMidtermYk KNo ratings yet
- 0001 01 PDFDocument10 pages0001 01 PDFAmmar Al-basitiNo ratings yet
- 2SB1587 PDFDocument1 page2SB1587 PDFisaiasvaNo ratings yet
- 2SB1647Document1 page2SB1647Julio barriosNo ratings yet
- Marks Spliting Sheet (1 To 20)Document33 pagesMarks Spliting Sheet (1 To 20)Sri JalakamNo ratings yet
- ATS EngDocument1 pageATS EngOctavianus LinNo ratings yet
- Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SC5100)Document1 pageSilicon PNP Epitaxial Planar Transistor (Complement To Type 2SC5100)EdgarAlonsoNo ratings yet
- Fault Switch 1: Headlights InopDocument4 pagesFault Switch 1: Headlights InopLong HàNo ratings yet
- ARL300 SynchronousDocument29 pagesARL300 SynchronousBrahim CherguiNo ratings yet
- BGB (Ground Floor)Document1 pageBGB (Ground Floor)A.K.M Shafiq MondolNo ratings yet
- Darlington: Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SD2439)Document1 pageDarlington: Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SD2439)Elcio BrembattiNo ratings yet
- DatasheetDocument1 pageDatasheetmixespirit73No ratings yet
- 029 00065 0 2sa1746Document1 page029 00065 0 2sa1746karimNo ratings yet
- 37 Sequoia (Cont. Next Page)Document2 pages37 Sequoia (Cont. Next Page)وليدمطهر الشجاعNo ratings yet
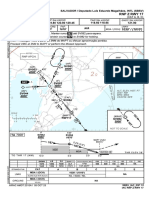
- SBSP Rnp-T-Rwy-17l Iac 20210909Document1 pageSBSP Rnp-T-Rwy-17l Iac 20210909Patrick ReisNo ratings yet
- Havana NightDocument30 pagesHavana NightもりMoriNo ratings yet
- 02 Grav Exe Gro Fe R+1 BS 311 0B PDFDocument1 page02 Grav Exe Gro Fe R+1 BS 311 0B PDFNguyen Khac DatNo ratings yet
- First FloorDocument1 pageFirst FloorQawi Pg SofryNo ratings yet
- First FloorDocument1 pageFirst FloorQawi Pg SofryNo ratings yet
- Darlington: Silicon NPN Triple Diffused Planar Transistor (Complement To Type 2SB1687)Document1 pageDarlington: Silicon NPN Triple Diffused Planar Transistor (Complement To Type 2SB1687)mundomusicalmeriaNo ratings yet
- Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SC2922)Document1 pageSilicon PNP Epitaxial Planar Transistor (Complement To Type 2SC2922)PETRONELA BADUNo ratings yet
- Power Wiring For Eb DG Panel Notes: Apparent Power Control SystemsDocument1 pagePower Wiring For Eb DG Panel Notes: Apparent Power Control SystemssaravananNo ratings yet
- Rodrigo Gonçalves de Sousa - Two Movements For OrchestraDocument49 pagesRodrigo Gonçalves de Sousa - Two Movements For OrchestraRodrigo SousaNo ratings yet
- 2SC2922Document1 page2SC2922zeckNo ratings yet
- 2017 October Qas: Liuu @tilDocument25 pages2017 October Qas: Liuu @tilJason Evan AndalesNo ratings yet
- Gobelin Miniscore: OxygenDocument17 pagesGobelin Miniscore: OxygenLaimonas MaseviciusNo ratings yet
- SBSP - Sid Rnav Porbi 2a Rwy 17r - 17l - Sid - 20171012Document2 pagesSBSP - Sid Rnav Porbi 2a Rwy 17r - 17l - Sid - 20171012mike jackNo ratings yet
- DAPOT LAYOUT lt2 VASIN 2017 PDFDocument1 pageDAPOT LAYOUT lt2 VASIN 2017 PDFZevanyaRolandTualakaNo ratings yet
- Darlington: Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SD2561)Document1 pageDarlington: Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SD2561)Daniel de la CrruzNo ratings yet
- SBSV Rnp-Z-Rwy-17 Iac 20231005Document1 pageSBSV Rnp-Z-Rwy-17 Iac 20231005Ulisses MalheirosNo ratings yet
- Silicon NPN Triple Diffused Planar Transistor (High Voltage and High Speed Switchihg Transistor)Document1 pageSilicon NPN Triple Diffused Planar Transistor (High Voltage and High Speed Switchihg Transistor)José BenavidesNo ratings yet
- Silicon PNP Epitaxial Planar Transistor: (Complement To Type 2SC2922)Document1 pageSilicon PNP Epitaxial Planar Transistor: (Complement To Type 2SC2922)busamawan wayanNo ratings yet
- Covalent Bonding and Hybridization 2Document1 pageCovalent Bonding and Hybridization 2domcruz0308No ratings yet
- Zegar - 4xIN12B Ex SMDsDocument1 pageZegar - 4xIN12B Ex SMDsMaciej FierdonekNo ratings yet
- Asm Charitable Super Specialty Hospital and Medical CollegeDocument20 pagesAsm Charitable Super Specialty Hospital and Medical CollegeTripurari KumarNo ratings yet
- Alternative and Complementary Medicine: AlterativeDocument9 pagesAlternative and Complementary Medicine: AlterativemuhammadriazNo ratings yet
- Oet 2.0 Writing Lesson: ReviewDocument12 pagesOet 2.0 Writing Lesson: ReviewDandlers MurrayNo ratings yet
- SCIF1111 Notes For Susan Hardy First TestDocument5 pagesSCIF1111 Notes For Susan Hardy First TestOliverNo ratings yet
- Fistula in Ano Final For PresentationDocument41 pagesFistula in Ano Final For PresentationRhajeeb Aennas SugalaNo ratings yet
- Maceradora Vortex VortexPlusDocument5 pagesMaceradora Vortex VortexPlusGaijin Elizabeth Fuentes AlvearNo ratings yet
- Mebo OintmentDocument17 pagesMebo OintmentFarahNo ratings yet
- Welcome To The University of Göttingen: Guide For International ResearchersDocument79 pagesWelcome To The University of Göttingen: Guide For International Researchersdapias09No ratings yet
- Interpret Your CapnogramDocument5 pagesInterpret Your CapnogramMayHnin KhaingNo ratings yet
- Treatment For Gangrene A. DryDocument2 pagesTreatment For Gangrene A. DryKey LomonovNo ratings yet
- PeritonitisDocument21 pagesPeritonitisNirav SharmaNo ratings yet
- Malignant Hypertension - Dr. Todung PDFDocument12 pagesMalignant Hypertension - Dr. Todung PDFMuhammad Khoirul SodiqNo ratings yet
- DPD and BPDDocument6 pagesDPD and BPDKamilah Haniyah MunawarNo ratings yet
- Peter Paul Lucas, Et. Al. v. Dr. TuañoDocument10 pagesPeter Paul Lucas, Et. Al. v. Dr. TuañoRachel CayangaoNo ratings yet
- Pizotifen To Prevent Migraine Headaches 1Document2 pagesPizotifen To Prevent Migraine Headaches 1William ImpNo ratings yet
- Gynaecological History TakingDocument16 pagesGynaecological History TakingnelsonNo ratings yet
- Subjective Examination Template 2022Document5 pagesSubjective Examination Template 2022LibbyNo ratings yet
- Tugas Ilmu Penyakit ViralDocument4 pagesTugas Ilmu Penyakit ViralHelda AudyaNo ratings yet
- HematuriaDocument7 pagesHematuriaAgi TaronNo ratings yet
- JC Arrive Trial PresentationDocument45 pagesJC Arrive Trial PresentationNamrata Dhital BhusalNo ratings yet
- Super Arrow Flex Sheath - Brochure - EN PDFDocument3 pagesSuper Arrow Flex Sheath - Brochure - EN PDFbiomedical_com_brNo ratings yet
- Manual Therapy: H. Wittink, R. Engelbert, T. TakkenDocument8 pagesManual Therapy: H. Wittink, R. Engelbert, T. TakkenJor ChavezNo ratings yet
- Nursing Care Plan: Al Greig S. Samedra, BSN, RNDocument4 pagesNursing Care Plan: Al Greig S. Samedra, BSN, RNAl GreigNo ratings yet