You might also like
- Bashar - 4th Dimension Vrs 4 DensityDocument2 pagesBashar - 4th Dimension Vrs 4 DensityMartin Spyyd Přidal100% (1)
- Activity 2Document5 pagesActivity 2api-492104888100% (1)
- Lab Report 4 Colligative PropertiesDocument9 pagesLab Report 4 Colligative Propertiesapi-436054247No ratings yet
- Safety Devices Manual 7300 KOBELCO Crawler CraneDocument71 pagesSafety Devices Manual 7300 KOBELCO Crawler CraneWilliam ColinsNo ratings yet
- Rabi3a Old Edittion 1985 Cairo University 2nd Petroleum 16Document319 pagesRabi3a Old Edittion 1985 Cairo University 2nd Petroleum 16Abdelaziz Mohamed Abdelmoaty Arafa100% (1)
- Saxophun PartirureDocument7 pagesSaxophun PartirureadamNo ratings yet
- Artificial Intelligence For Trading: Nanodegree Program SyllabusDocument18 pagesArtificial Intelligence For Trading: Nanodegree Program SyllabusAryan PegwarNo ratings yet
- Research Methods HandoutDocument32 pagesResearch Methods HandoutRaldie Atchaso0% (1)
- MM1114761-00 HP ELECTRICAL DIAGRAM (Analogic Version)Document23 pagesMM1114761-00 HP ELECTRICAL DIAGRAM (Analogic Version)Bruno Adrover100% (1)
- Integral Calculus: John Rey M. Pacturanan, CE, MPDocument2 pagesIntegral Calculus: John Rey M. Pacturanan, CE, MPNathanielle AndreaNo ratings yet
- Enumeration Data AnalysisDocument9 pagesEnumeration Data AnalysisLaura Acacia0% (1)
- UserManual 703Document733 pagesUserManual 703Gaetano GaetanoNo ratings yet
- Porsche Macan Técnical Service Information 2017Document52 pagesPorsche Macan Técnical Service Information 2017Jonas Dos Santos AndradeNo ratings yet
- AASHTO T288 Determining Minimum Laboratory Soil Resistivity- Đo Điện CựcDocument7 pagesAASHTO T288 Determining Minimum Laboratory Soil Resistivity- Đo Điện Cựcphạm anh túNo ratings yet
- 142 Ped Cystic FibrosisDocument9 pages142 Ped Cystic FibrosisritaNo ratings yet
- 0067 27Document5 pages0067 27Alex ChenNo ratings yet
- 144 Ped Foreign Body IngestionDocument3 pages144 Ped Foreign Body IngestionritaNo ratings yet
- Block 1Document22 pagesBlock 1ايات عبدالرحمنNo ratings yet
- 0001 01 PDFDocument10 pages0001 01 PDFAmmar Al-basitiNo ratings yet
- Ith in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsDocument6 pagesIth in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsAlex ChenNo ratings yet
- Item:: E L E EDocument7 pagesItem:: E L E Eshahbaz HazardousNo ratings yet
- Scan 27 Oct 2022Document11 pagesScan 27 Oct 2022Noha badrNo ratings yet
- Ati RN Proctored Maternal Newborn Form C 2016Document2 pagesAti RN Proctored Maternal Newborn Form C 2016Stevania96% (24)
- Ms Lecture 4 PDFDocument11 pagesMs Lecture 4 PDFAkash GolwalkarNo ratings yet
- Generic Control Panel For Plus - R02Document46 pagesGeneric Control Panel For Plus - R02juanNo ratings yet
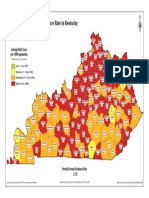
- Incidence Map 1111Document1 pageIncidence Map 1111WBKONo ratings yet
- Su ND: o o o o oDocument3 pagesSu ND: o o o o oAlex ChenNo ratings yet
- ScreenshotDocument1 pageScreenshotvokaNo ratings yet
- Su ND: Item: ADocument8 pagesSu ND: Item: AHawkElseNo ratings yet
- Incidence Map 111521Document1 pageIncidence Map 111521Debbie HarbsmeierNo ratings yet
- Laser Cutter Manual UeleleleDocument23 pagesLaser Cutter Manual UeleleleJ YapNo ratings yet
- Screenshot (177) (20 Files Merged)Document28 pagesScreenshot (177) (20 Files Merged)Frances Marie Z. CieloNo ratings yet
- 61246906-80 ATEX Plus IO Module For PanelDocument23 pages61246906-80 ATEX Plus IO Module For PaneljuanNo ratings yet
- Aabba: Aabbccdc A Aa - 'It Aabbccdc Aabbccc Aabbcca AabbccaDocument3 pagesAabba: Aabbccdc A Aa - 'It Aabbccdc Aabbccc Aabbcca Aabbccamaulana khadafiNo ratings yet
- MID22Document7 pagesMID22leh7989No ratings yet
- PsychiatryBlock 4QDocument13 pagesPsychiatryBlock 4Qboparai.navjantNo ratings yet
- Applelicious 1Document6 pagesApplelicious 1api-117237667No ratings yet
- WD14H460FF 01 Codes 2 PDFDocument27 pagesWD14H460FF 01 Codes 2 PDFBOSCHCLASSIXX1200No ratings yet
- Solution TextbookDocument126 pagesSolution Textbookteerapat8199No ratings yet
- 61246869-80 Plus IO Box - R03Document25 pages61246869-80 Plus IO Box - R03juanNo ratings yet
- AppleliciousDocument6 pagesAppleliciousapi-117237667No ratings yet
- Btruool Assocurrs Lp: ltti郡Document3 pagesBtruool Assocurrs Lp: ltti郡Simon YiuNo ratings yet
- S1 Chapter 5 NotesDocument4 pagesS1 Chapter 5 NotesmalvinalaiNo ratings yet
- PPH 23Document1 pagePPH 23ilhamNo ratings yet
- 6.6 THRU' 2 Nos: Forbes & Company LimitedDocument1 page6.6 THRU' 2 Nos: Forbes & Company LimitedChandru ChristurajNo ratings yet
- Chelsea Version2Document1 pageChelsea Version2Health BrookNo ratings yet
- Img 20221014 0006Document1 pageImg 20221014 0006philipNo ratings yet
- Item:: 0. LD: 2777 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomDocument10 pagesItem:: 0. LD: 2777 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomHawkElseNo ratings yet
- Solar Cell I-V Cuk ConverterDocument1 pageSolar Cell I-V Cuk ConverterKORAKRIT ANANTA-AUOYPORNNo ratings yet
- Chapter 2Document18 pagesChapter 2Hadi SleemNo ratings yet
- 20.Worktng Ranges: Sk200 (Lc) Ⅶ Sk210くLc) ⅦDocument5 pages20.Worktng Ranges: Sk200 (Lc) Ⅶ Sk210くLc) ⅦHậu MinhNo ratings yet
- iSTYLE UAE Iphone 6 Invoice PDFDocument1 pageiSTYLE UAE Iphone 6 Invoice PDFsawantsamir06No ratings yet
- ABE-34 Document Submittal LogDocument209 pagesABE-34 Document Submittal LogFranklyn GenoveNo ratings yet
- Catalogo 2018 DIODocument133 pagesCatalogo 2018 DIOSamara Maya100% (1)
- 61211302-80 Large Junction Box R12Document21 pages61211302-80 Large Junction Box R12juanNo ratings yet
- Salmon Roses: Want Ol:1r TopDocument1 pageSalmon Roses: Want Ol:1r ToprcfNo ratings yet
- MCR3 Funcional PDFDocument4 pagesMCR3 Funcional PDFLucas Mathias Lobos EtcheverriaNo ratings yet
- PDY-81-41-06338 - E14-Rev-1ADocument1 pagePDY-81-41-06338 - E14-Rev-1Aisan.structural TjsvgalavanNo ratings yet
- 23 Sur Deviated Nasal SeptumDocument3 pages23 Sur Deviated Nasal SeptumSardar jiNo ratings yet
- Tricky Maths (Arithmetic) Sunil Khurab (Sscstudy - Com)Document289 pagesTricky Maths (Arithmetic) Sunil Khurab (Sscstudy - Com)sdeepika_bNo ratings yet
- Kootenay Lake Pennywise November 14, 2017Document41 pagesKootenay Lake Pennywise November 14, 2017Pennywise PublishingNo ratings yet
- Clel083e138 MVSWG Exe WDG 603Document41 pagesClel083e138 MVSWG Exe WDG 603arielaparicioNo ratings yet
- Incidence Map 10152021Document1 pageIncidence Map 10152021Debbie HarbsmeierNo ratings yet
- Calibración Termohigrometro 2019Document1 pageCalibración Termohigrometro 2019Chirley Jazmin Bayona BautistaNo ratings yet
- LD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomDocument5 pagesLD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- Full Ati RN Proctored Fundamentals Form B 2016 PDF Docx Full Chapter ChapterDocument35 pagesFull Ati RN Proctored Fundamentals Form B 2016 PDF Docx Full Chapter Chapterprosaism.horologe.fuu88100% (22)
- Magellan - BA Z8AD DB Battery BDocument1 pageMagellan - BA Z8AD DB Battery Baung kokoNo ratings yet
- Full Ati RN Proctored Nursing Care of Children 2016 Form C PDF Docx Full Chapter ChapterDocument34 pagesFull Ati RN Proctored Nursing Care of Children 2016 Form C PDF Docx Full Chapter Chapterprosaism.horologe.fuu88100% (21)
- Instant Centers of Velocities: P. Nikravesh, AME, U of ADocument15 pagesInstant Centers of Velocities: P. Nikravesh, AME, U of ANguyen PhanNo ratings yet
- Making Materials Matter: Product CatalogueDocument7 pagesMaking Materials Matter: Product Cataloguemustafasenbagci3693No ratings yet
- (August 15, 2018) Diagnostic TestDocument5 pages(August 15, 2018) Diagnostic TestReyniel Layson VergaraNo ratings yet
- Change Yourself: Golang Cheat SheetDocument2 pagesChange Yourself: Golang Cheat SheetZerihunNo ratings yet
- Ass2sqlqueries Enyo Ahovi Juliette HoedemakersDocument12 pagesAss2sqlqueries Enyo Ahovi Juliette Hoedemakersapi-269609223No ratings yet
- Barthel Index For Stroke Trials Development, Properties, and ApplicationDocument6 pagesBarthel Index For Stroke Trials Development, Properties, and ApplicationDewi HidajatiNo ratings yet
- Abu Madi - Performance Characteristics Correlation For Round Tube and Plate Finned Heat ExchangersDocument11 pagesAbu Madi - Performance Characteristics Correlation For Round Tube and Plate Finned Heat Exchangersmios30129800% (1)
- Cfaf240320a0 024SC A1 1Document15 pagesCfaf240320a0 024SC A1 1João Paulo Da S NogueiraNo ratings yet
- Thii 111Document62 pagesThii 111Tăng Anh TuấnNo ratings yet
- "Page Replacement Algorithms": - A-28 Manasi Dhote A-32 Akshat Gandhi A-63 Dhruv MistryDocument18 pages"Page Replacement Algorithms": - A-28 Manasi Dhote A-32 Akshat Gandhi A-63 Dhruv MistryManasiNo ratings yet
- A Study of An Analytic Solution of 1D Heat Equation: April 21, 2019Document31 pagesA Study of An Analytic Solution of 1D Heat Equation: April 21, 2019manikandanNo ratings yet
- Q3 Summative #2 ScienceDocument7 pagesQ3 Summative #2 ScienceSonny MatiasNo ratings yet
- Manual-PST-15S 30S 60SDocument33 pagesManual-PST-15S 30S 60SrayNo ratings yet
- Electrical Supply SustemDocument13 pagesElectrical Supply SustemZulHilmi ZakariaNo ratings yet
- The Growth Curve of CellsDocument3 pagesThe Growth Curve of CellsRisky KikiNo ratings yet
- DAC-4 Data Sheet E R13 20151005Document12 pagesDAC-4 Data Sheet E R13 20151005Ricardo Felipe Cortes MenayNo ratings yet
- TraceDocument394 pagesTraceМакс МорданьNo ratings yet
- Quiz I Review Probabilistic Systems Analysis 6.041/6.431: October 7, 2010Document27 pagesQuiz I Review Probabilistic Systems Analysis 6.041/6.431: October 7, 2010Birbhadra DhunganaNo ratings yet
- Becknam-Ref VrednostiDocument44 pagesBecknam-Ref VrednostialisaNo ratings yet
- Math Corrproblems 2019Document4 pagesMath Corrproblems 2019weng paraleNo ratings yet
- How To Specify A Variable Frequency Drive PDFDocument4 pagesHow To Specify A Variable Frequency Drive PDFVinit JoryNo ratings yet