You might also like
- Ectopic Pregnancy Case StudyDocument37 pagesEctopic Pregnancy Case StudyJoule Peirre83% (6)
- Crohn's and Colitis: Understanding and Managing IBDFrom EverandCrohn's and Colitis: Understanding and Managing IBDRating: 5 out of 5 stars5/5 (3)
- Cbs BookDocument294 pagesCbs Bookadmiralninja100% (1)
- Resume AncDocument15 pagesResume Ancdwi pratiwiNo ratings yet
- MSU Buug College Nursing Assessment for Abdominal PainDocument30 pagesMSU Buug College Nursing Assessment for Abdominal Painllanelli.graciaNo ratings yet
- Askep B IngDocument19 pagesAskep B IngbalqisNo ratings yet
- Eti Junia Astuti ENGLISHDocument12 pagesEti Junia Astuti ENGLISHEti JuniaNo ratings yet
- Askep - Stroke Hemoragic - Ni Luh Putu Mey Ani - kdp2021Document24 pagesAskep - Stroke Hemoragic - Ni Luh Putu Mey Ani - kdp2021LuhSuandewiNo ratings yet
- Patient Assessment Database for Lung Tuberculosis PatientDocument6 pagesPatient Assessment Database for Lung Tuberculosis PatientRyan KaisooNo ratings yet
- 2B - Askep TB Paru - R.teratai A enDocument46 pages2B - Askep TB Paru - R.teratai A enPutri MeylisaNo ratings yet
- Case Study About Cystic Fibrosis GeneDocument40 pagesCase Study About Cystic Fibrosis GeneEvora, Sichem D.No ratings yet
- Format Pengkajian Bahasa InggrisDocument3 pagesFormat Pengkajian Bahasa InggrisSapnahNo ratings yet
- Nursing Document Nursing Care at MR.D With Hypertermia: Dengue Haemorogic Fever (DHF) in Mawar Room Dr. R. Soeprapto Cepu HospitalDocument9 pagesNursing Document Nursing Care at MR.D With Hypertermia: Dengue Haemorogic Fever (DHF) in Mawar Room Dr. R. Soeprapto Cepu Hospitalanggarani saskiaNo ratings yet
- English Nursing AssignmentsDocument12 pagesEnglish Nursing AssignmentsElsa karuniatiNo ratings yet
- Asuhan Keperawatan Ny. N dengan StrumaDocument14 pagesAsuhan Keperawatan Ny. N dengan Strumanora cyeanirNo ratings yet
- Quality Form Poltekkes Kemenkes Denpasar Midwifery Care Documentation For Pregnant WomenDocument9 pagesQuality Form Poltekkes Kemenkes Denpasar Midwifery Care Documentation For Pregnant WomenVince DethanNo ratings yet
- Askep Bahasa Inggris SaneDocument12 pagesAskep Bahasa Inggris SaneRio FernandoNo ratings yet
- Revisi MuluDocument20 pagesRevisi MuluMiskan FebrianiNo ratings yet
- Askep KLP 3 Kebutuhan Cairan-DiareDocument19 pagesAskep KLP 3 Kebutuhan Cairan-Diarepandawa love7000No ratings yet
- Nursing Assesement of Typhoid FeverDocument9 pagesNursing Assesement of Typhoid FeverNurhanifahNo ratings yet
- Soap Anc Inc PNC BBLDocument34 pagesSoap Anc Inc PNC BBLida nurfaridaNo ratings yet
- Nursing Process Group 4Document32 pagesNursing Process Group 4Ari NingsihNo ratings yet
- ASKEP Abses Abdomen NavaDocument18 pagesASKEP Abses Abdomen NavaNava UsmanNo ratings yet
- Cyctocyle - Care PlanDocument22 pagesCyctocyle - Care Planarchana vermaNo ratings yet
- Ritah's Very Reproductive Health PortifolioDocument18 pagesRitah's Very Reproductive Health PortifolioDerick AaronNo ratings yet
- GROUP 2 - NEW-OB-RISK-NICU-CASE-STUDY-FORMAT-for-2nd-yearDocument28 pagesGROUP 2 - NEW-OB-RISK-NICU-CASE-STUDY-FORMAT-for-2nd-yearReymart EstebanNo ratings yet
- LK KDP KELOMPOK 2 RevDocument22 pagesLK KDP KELOMPOK 2 RevTutik DhakirohNo ratings yet
- DR - ERLIN FixDocument31 pagesDR - ERLIN FixFelicia Angela KanzilNo ratings yet
- Askep EnglishDocument10 pagesAskep EnglishDayu AriNo ratings yet
- Nursing Process On MRS.T With Medical Diagnosis Post SC With DKP Indication in Srikandi Ward Nyi Ageng Serang HospitalDocument15 pagesNursing Process On MRS.T With Medical Diagnosis Post SC With DKP Indication in Srikandi Ward Nyi Ageng Serang HospitalVitaNo ratings yet
- Understanding Knowledge and Attitudes of Depo Provera Acceptors Towards Weight GainDocument14 pagesUnderstanding Knowledge and Attitudes of Depo Provera Acceptors Towards Weight GainRianaNurFatimahNo ratings yet
- DHF Case Report Nursing Care for Mr. IDocument9 pagesDHF Case Report Nursing Care for Mr. ISriarliza FebrianiNo ratings yet
- Developing Nursing Process AssessmentDocument49 pagesDeveloping Nursing Process AssessmentAhmad BuchoriNo ratings yet
- FNCP LeprosyDocument7 pagesFNCP LeprosyChristian Eduard de DiosNo ratings yet
- KehamilanDocument9 pagesKehamilanEsawitri ApriliaNo ratings yet
- Child Case StudyDocument33 pagesChild Case StudyBhageshwar ChaudharyNo ratings yet
- WVSU College of Nursing Gynecological AssessmentDocument12 pagesWVSU College of Nursing Gynecological AssessmentelleNo ratings yet
- Antenatal ExaminationDocument8 pagesAntenatal ExaminationAli 13No ratings yet
- DOKUMENTASI ASUHAN IBU NIFAS FIX 2-6 HARI - Id.enDocument5 pagesDOKUMENTASI ASUHAN IBU NIFAS FIX 2-6 HARI - Id.entirtaNo ratings yet
- Peptic Ulcer2Document84 pagesPeptic Ulcer2NICAIRA MARIE PERTUBALNo ratings yet
- Askep Bahasa InggrisDocument5 pagesAskep Bahasa InggrisRinalstNo ratings yet
- Makalah Long Case MF 21.11Document18 pagesMakalah Long Case MF 21.11Mejestha SimanjuntakNo ratings yet
- CR4 - Dea BKDocument45 pagesCR4 - Dea BKThadea Odilia TandiNo ratings yet
- Nursing Case Study ApaleDocument14 pagesNursing Case Study ApaleAna LuisaNo ratings yet
- Askeb Ny - Siti Nurafifah 3 HariDocument6 pagesAskeb Ny - Siti Nurafifah 3 HariJunita RahmaningtyasNo ratings yet
- Department Social Case StudyDocument28 pagesDepartment Social Case StudySathish100% (1)
- LONG CASE DR OcaDocument20 pagesLONG CASE DR OcanurfadillahNo ratings yet
- C2120060 Askep Kadek Ari Nesilawati Post AppendiktomiDocument23 pagesC2120060 Askep Kadek Ari Nesilawati Post Appendiktomiadila sayangNo ratings yet
- St. Anne College Lucena Inc. Diversion Road G-Gulang Lucena CityDocument22 pagesSt. Anne College Lucena Inc. Diversion Road G-Gulang Lucena CitymcensoredNo ratings yet
- UL Darmawan Murdono EngDocument48 pagesUL Darmawan Murdono EngpermatamoNo ratings yet
- Martini Ulok Edit1Document62 pagesMartini Ulok Edit1RonnyRahardjaNo ratings yet
- Askep HivDocument17 pagesAskep Hivputri d dianiNo ratings yet
- Laporan Kompre Iufd - FixDocument14 pagesLaporan Kompre Iufd - FixAkhid FalikhuddinNo ratings yet
- ASKEP GOUT TN.SDocument13 pagesASKEP GOUT TN.Smicchella16No ratings yet
- Askep Angina Pectoris Bhs InggrisDocument16 pagesAskep Angina Pectoris Bhs InggrisMillitio ChristiantoroNo ratings yet
- English Nursing Care Plan for Diabetes PatientDocument7 pagesEnglish Nursing Care Plan for Diabetes PatientMuhammad Amin KutbiNo ratings yet
- Health History Documentation Form ChristinaDocument6 pagesHealth History Documentation Form Christinaapi-545542584No ratings yet
- Case Press Ob WardDocument9 pagesCase Press Ob Wardjohn castroNo ratings yet
- Askep INC KPD - MEI DWI FEMILA - 2001032005Document19 pagesAskep INC KPD - MEI DWI FEMILA - 2001032005Hairul HasanNo ratings yet
- Nursing in Ny. S Post SC WITH Disproportion Head Hip (DKP)Document21 pagesNursing in Ny. S Post SC WITH Disproportion Head Hip (DKP)ika dwiNo ratings yet
- Hope in Cancer Therapy: A holistic approach to cancer with curcumin, b17, insulin, methadone & co.From EverandHope in Cancer Therapy: A holistic approach to cancer with curcumin, b17, insulin, methadone & co.No ratings yet
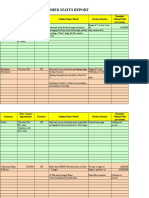
- Customer Status Update Report 27th January 2015 ColourDocument20 pagesCustomer Status Update Report 27th January 2015 ColourmaryNo ratings yet
- Primary Maths Dissertation ExamplesDocument8 pagesPrimary Maths Dissertation ExamplesPaperWritersAlbuquerque100% (1)
- Hotel Training ReportDocument14 pagesHotel Training ReportButchick Concepcion Malasa100% (1)
- Farmakoterapi Penyakit Infeksi: in Infectious Diseases Dewi Rahmawati, M.Farm-Klin.,AptDocument87 pagesFarmakoterapi Penyakit Infeksi: in Infectious Diseases Dewi Rahmawati, M.Farm-Klin.,AptYemima MNo ratings yet
- Tulsi Ka Kavya Aur Samanvay Ki ChestaDocument6 pagesTulsi Ka Kavya Aur Samanvay Ki Chestaaman singhNo ratings yet
- 65-1-3-D MathematicsDocument8 pages65-1-3-D MathematicsRohan YadavNo ratings yet
- Preschool ADHD QuestionnaireDocument2 pagesPreschool ADHD QuestionnaireAnnaNo ratings yet
- Section 6 - Diagnostic ProceduresDocument13 pagesSection 6 - Diagnostic Proceduresanon_152488453100% (1)
- Electric Potential and CapacitanceDocument30 pagesElectric Potential and CapacitanceRachita PatangiNo ratings yet
- I. VHF CommunicationsDocument12 pagesI. VHF CommunicationsSamuel OyelowoNo ratings yet
- Hospital Food Service: October 2019Document28 pagesHospital Food Service: October 2019Shaikh Sobiya 57No ratings yet
- Bungsuan NHS Then and Now in PerspectiveDocument2 pagesBungsuan NHS Then and Now in Perspectivedanicafayetamagos02No ratings yet
- Physics Universe ModelsDocument14 pagesPhysics Universe ModelsTracy zorca50% (2)
- TM Journal Class 5 Pharma Trademarks 2018Document1,192 pagesTM Journal Class 5 Pharma Trademarks 2018Tahir LabbeNo ratings yet
- Final CBLMDocument66 pagesFinal CBLMRanilyn UrbiztundoNo ratings yet
- All+DPPs+in+One+ +M+and+DDocument136 pagesAll+DPPs+in+One+ +M+and+DSumit RajNo ratings yet
- The Principles Taj MahalDocument2 pagesThe Principles Taj MahalVishnuMohanNo ratings yet
- Manual THT70 PDFDocument54 pagesManual THT70 PDFwerterNo ratings yet
- Lauren Tarshis - (I Survived 05) - I Survived The San Francisco Earthquake, 1906Document66 pagesLauren Tarshis - (I Survived 05) - I Survived The San Francisco Earthquake, 1906Olga de Ramos100% (1)
- Aquilion ONE GENESIS Edition Transforming CTDocument40 pagesAquilion ONE GENESIS Edition Transforming CTSemeeeJuniorNo ratings yet
- Ancient South Arabian TradeDocument16 pagesAncient South Arabian TradeAbo AliNo ratings yet
- The Vatican As A World Power (1939)Document481 pagesThe Vatican As A World Power (1939)sexylove1477No ratings yet
- Owner'S Manual: Dell Poweredge T110 Ii SystemsDocument130 pagesOwner'S Manual: Dell Poweredge T110 Ii SystemsDonNo ratings yet
- Oil Well Drilling Methods: University of Karbala College of Engineering Petroleum Eng. DepDocument8 pagesOil Well Drilling Methods: University of Karbala College of Engineering Petroleum Eng. DepAli MahmoudNo ratings yet
- Interconnection of Power SystemsDocument5 pagesInterconnection of Power SystemsRohan Sharma50% (2)
- Thesis Based On Digital Image ProcessingDocument7 pagesThesis Based On Digital Image Processingkristenwilsonpeoria100% (1)
- RRB NTPC Cut Off 2022 - CBT 2 Region Wise Cut Off Marks & Answer KeyDocument8 pagesRRB NTPC Cut Off 2022 - CBT 2 Region Wise Cut Off Marks & Answer KeyAkash guptaNo ratings yet
- 2016 Annual Report - Printer-ReadyDocument35 pages2016 Annual Report - Printer-ReadyDonna BrodberNo ratings yet
- Telecom Business Management Systems Net ProjectDocument68 pagesTelecom Business Management Systems Net ProjectRahul RaiNo ratings yet