You might also like
- Test Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiDocument479 pagesTest Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiBetsy Brown Byersmith90% (134)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
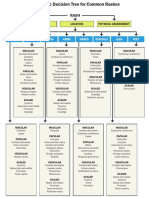
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
- Cardiovascular System SheetDocument11 pagesCardiovascular System SheetBetsy Brown ByersmithNo ratings yet
- Exam 4 Study Guide (1386)Document11 pagesExam 4 Study Guide (1386)S. MartinezNo ratings yet
- HeartDocument7 pagesHeartKaryll AguilaNo ratings yet
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- Lecture 3 Cardiovascular System 1Document54 pagesLecture 3 Cardiovascular System 1hafiz patah100% (1)
- Cardiovascular System BSN 1Document16 pagesCardiovascular System BSN 1Arianne Jen GenotivaNo ratings yet
- Heart Anatomy Only StudentsDocument34 pagesHeart Anatomy Only Studentscharlene.jadulcoNo ratings yet
- Components of The Cardiovascular SystemDocument23 pagesComponents of The Cardiovascular SystemMr. DummyNo ratings yet
- Chapter 19 Heart Marie BDocument29 pagesChapter 19 Heart Marie BomarNo ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- NCM Responses To Altered Oxygenation Cardiac FunctionDocument14 pagesNCM Responses To Altered Oxygenation Cardiac FunctionJeson Vien GuerraNo ratings yet
- Regulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowDocument20 pagesRegulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowShveta MahajanNo ratings yet
- Module 5 CardioVascular SystemDocument7 pagesModule 5 CardioVascular SystemWai KikiNo ratings yet
- Conduction System of HeartDocument7 pagesConduction System of HeartThakur KanchanNo ratings yet
- Cardiovascular and Circulatory FunctionDocument271 pagesCardiovascular and Circulatory FunctionARAGON GEMMA LYNNo ratings yet
- Week 10 Study GuideDocument12 pagesWeek 10 Study GuideCharli ParachinniNo ratings yet
- Heart ChambersDocument14 pagesHeart Chambersberniebernie20No ratings yet
- THE HEART HandoutDocument61 pagesTHE HEART HandoutMitha PelangiNo ratings yet
- Ecg 1Document4 pagesEcg 1Lindsay Ann Garcia MariacaNo ratings yet
- Lecture Notes NCM 102: Union Christian College College of NursingDocument77 pagesLecture Notes NCM 102: Union Christian College College of Nursingnarswiponshistoryan100% (1)
- Oral RevDocument6 pagesOral RevjjolaguerNo ratings yet
- Cardionursing 110207023802 Phpapp01Document18 pagesCardionursing 110207023802 Phpapp01LudwigJayBarayuga100% (5)
- MS CVS ReviewDocument41 pagesMS CVS ReviewShayesra-Radina Laja SahibadNo ratings yet
- Cardiogenic ShockDocument14 pagesCardiogenic ShockZellanien hdNo ratings yet
- CardioDocument30 pagesCardioPamela LusungNo ratings yet
- Lesson 4: Function of The Human Heart: Report byDocument29 pagesLesson 4: Function of The Human Heart: Report byAngelo Julius NuqueNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- The Cardiovascular SystemDocument13 pagesThe Cardiovascular SystemCaraDeleNo ratings yet
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- Cardio PulmonaryDocument4 pagesCardio PulmonaryAyessa CortesNo ratings yet
- STPM BIOLOGY TransportDocument18 pagesSTPM BIOLOGY Transportwkwhui100% (2)
- SM - AnimalPhysiology - CirculatorySystem Taught Until 22.10.2018 PDFDocument19 pagesSM - AnimalPhysiology - CirculatorySystem Taught Until 22.10.2018 PDFMudit GeraNo ratings yet
- Cardiovascular System - Transportation 1Document28 pagesCardiovascular System - Transportation 1Louise Mica Lee100% (1)
- WEEK 1 MEDSURG AsynchDocument12 pagesWEEK 1 MEDSURG AsynchLeigh Angelika Dela CruzNo ratings yet
- CH 11 Heart NotesDocument2 pagesCH 11 Heart Notesummnicole0% (1)
- LIFS1902 Heart and CVS Revision NotesDocument6 pagesLIFS1902 Heart and CVS Revision NotesmystudylifechloeNo ratings yet
- 2 Anatomy and Physiology CVSDocument12 pages2 Anatomy and Physiology CVSambrosekiplangat6No ratings yet
- Common Cardiac Anomalies Seen Within The Cardiac Catheterization LabDocument23 pagesCommon Cardiac Anomalies Seen Within The Cardiac Catheterization Labapi-356406300No ratings yet
- Capillary: Nutrients To, and Take Wastes Away From, CellsDocument7 pagesCapillary: Nutrients To, and Take Wastes Away From, CellseyhethNo ratings yet
- Lecture Outline: Cardiovascular PhysiologyDocument146 pagesLecture Outline: Cardiovascular PhysiologyAlyssaNo ratings yet
- Chapter 5 Care of The Clients With Cardiovascular DisordersDocument226 pagesChapter 5 Care of The Clients With Cardiovascular DisordersDon Felicisimo EbronNo ratings yet
- Chapter 18 - The Heart Study Guide: Save Date: Wednesday, March 25, 2009 4:18:00 PMDocument7 pagesChapter 18 - The Heart Study Guide: Save Date: Wednesday, March 25, 2009 4:18:00 PMBettina RosuNo ratings yet
- Structure and Function of The Cardiovascular System PDFDocument9 pagesStructure and Function of The Cardiovascular System PDFteuuuuNo ratings yet
- NCMMSN Notes - Sacramento, Karl SebastianDocument96 pagesNCMMSN Notes - Sacramento, Karl SebastianRHEA MAY CAPORNo ratings yet
- Anaphy HeartDocument6 pagesAnaphy HeartAngellene GraceNo ratings yet
- Cardiovascular SystemDocument7 pagesCardiovascular SystemJoão EusébioNo ratings yet
- Heart Anatomy: LocationDocument45 pagesHeart Anatomy: LocationZaira100% (1)
- Chapter 20 A&P 2Document7 pagesChapter 20 A&P 2Jilian McGuganNo ratings yet
- Jantung PDFDocument1 pageJantung PDFKarensa JanetNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Beating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartFrom EverandBeating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartNo ratings yet
- Advanced Pharm From QuizletDocument62 pagesAdvanced Pharm From QuizletBetsy Brown Byersmith100% (1)
- Cardiovascular System SheetDocument11 pagesCardiovascular System SheetBetsy Brown ByersmithNo ratings yet
- Pharmacology ReviewDocument64 pagesPharmacology ReviewRichard BakerNo ratings yet
- AcutePrescribingLimits FINALDocument1 pageAcutePrescribingLimits FINALBetsy Brown ByersmithNo ratings yet
- Anemia ChartDocument1 pageAnemia ChartBetsy Brown ByersmithNo ratings yet
- Diuretics For CardiacDocument6 pagesDiuretics For CardiacBetsy Brown ByersmithNo ratings yet
- Top-200-Drug ETSYDocument31 pagesTop-200-Drug ETSYBetsy Brown ByersmithNo ratings yet
- DRUG Card FormDocument4 pagesDRUG Card FormBetsy Brown ByersmithNo ratings yet
- Advanced Pharmacology Study Guide II PDFDocument77 pagesAdvanced Pharmacology Study Guide II PDFBetsy Brown Byersmith100% (1)
- Guidelines For Complete SOAP2Document2 pagesGuidelines For Complete SOAP2Betsy Brown Byersmith100% (1)
- A2-Questions On Analyzing Nutrition ClaimsDocument3 pagesA2-Questions On Analyzing Nutrition ClaimsBetsy Brown ByersmithNo ratings yet
- What Are Analgesics?Document10 pagesWhat Are Analgesics?Betsy Brown ByersmithNo ratings yet
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocument77 pages2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryBetsy Brown ByersmithNo ratings yet
- Chemistry I The Atomic Bomb Elizabeth Byersmith February 26, 2009 Mercy College Professor KinglseyDocument3 pagesChemistry I The Atomic Bomb Elizabeth Byersmith February 26, 2009 Mercy College Professor KinglseyBetsy Brown ByersmithNo ratings yet
- Wound Care in Orthopaedic Case-Borromeus HospitalDocument96 pagesWound Care in Orthopaedic Case-Borromeus HospitalDavid DavidNo ratings yet
- Mesalamine ThesisDocument5 pagesMesalamine ThesisMary Montoya100% (2)
- Second Class UveitisDocument42 pagesSecond Class Uveitisabhishek tNo ratings yet
- Ais Student Medical and Health Declaration Form 2023-24Document7 pagesAis Student Medical and Health Declaration Form 2023-24hafizvy6No ratings yet
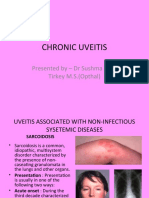
- Dr. Rozhan Yassin Khalil: Presented byDocument37 pagesDr. Rozhan Yassin Khalil: Presented bySyasya NanaNo ratings yet
- Clil Multikey Lesson Plan: Correlate Nutrition and HealthDocument13 pagesClil Multikey Lesson Plan: Correlate Nutrition and HealthMobiNo ratings yet
- Movie AnalysisDocument7 pagesMovie Analysisapi-542795774No ratings yet
- Plymouth University Postgraduate International Student Application FormDocument6 pagesPlymouth University Postgraduate International Student Application FormagusnestaalbugisyNo ratings yet
- Seminar ON: Birth InjuriesDocument38 pagesSeminar ON: Birth Injuriesvishnu100% (1)
- Influenza FormDocument2 pagesInfluenza FormDipendra PoudelNo ratings yet
- Picture of America PreventionDocument9 pagesPicture of America PreventionHuỳnh Bảo Anh NguyênNo ratings yet
- 26 Contoh Soal Analytical Exposition TextDocument9 pages26 Contoh Soal Analytical Exposition Textsayakentang23No ratings yet
- Assessmentof IranianNurses' KnowledgeandAnxietyToward COVID-19DuringtheCurrentOutbreakinIranDocument5 pagesAssessmentof IranianNurses' KnowledgeandAnxietyToward COVID-19DuringtheCurrentOutbreakinIranSergio Losada AmayaNo ratings yet
- English 10 - Q4 - M2 - EXTENDED DEFINITION FINAL 2.finalpdfDocument15 pagesEnglish 10 - Q4 - M2 - EXTENDED DEFINITION FINAL 2.finalpdfDennis Douglas Alo Jr.No ratings yet
- Bai Tap Nang Cao Tieng Anh Lop 12 Unit 2 Urbanisation 1Document26 pagesBai Tap Nang Cao Tieng Anh Lop 12 Unit 2 Urbanisation 1Đào HiếuNo ratings yet
- Chapter 5Document20 pagesChapter 5Berihu GirmayNo ratings yet
- Mod 3Document16 pagesMod 3Gin CruzNo ratings yet
- Lecture Notes On PsychiatryDocument38 pagesLecture Notes On Psychiatrygemazy123No ratings yet
- Learning Task 7.3: Digging The CircumstancesDocument2 pagesLearning Task 7.3: Digging The CircumstancesTakafumi KikuchiNo ratings yet
- Public Health Thesis IdeasDocument6 pagesPublic Health Thesis Ideaspamelawatkinsjackson100% (2)
- Southern Tagalog ChapterDocument4 pagesSouthern Tagalog ChapterwiltechworksNo ratings yet
- Paper Tendinitis Supraespinoso 10Document10 pagesPaper Tendinitis Supraespinoso 10Erika ParedesNo ratings yet
- 1 BEtextDocument34 pages1 BEtextSergio MontesNo ratings yet
- ADA Develops Guidance On Dental Emergency, Nonemergency CareDocument4 pagesADA Develops Guidance On Dental Emergency, Nonemergency CareAlejandro OrtizNo ratings yet
- NCLEX Questions PulmDocument27 pagesNCLEX Questions PulmAnthony Hawley100% (2)
- GPAQDocument6 pagesGPAQChibi ChanNo ratings yet
- Addison DiseaseDocument23 pagesAddison DiseaseKompari EvansNo ratings yet
- Making Swedish BittersDocument8 pagesMaking Swedish Bittersdeaqth100% (2)
- Gastrostomy FeedingDocument8 pagesGastrostomy FeedingAwol AregaNo ratings yet
- AIDS EssayDocument15 pagesAIDS EssayYasmin DisneyNo ratings yet