You might also like
- Or Sample ChartingDocument3 pagesOr Sample ChartingPrincess Sarey88% (8)
- SMETA 6.1 Measurement Criteria PDFDocument96 pagesSMETA 6.1 Measurement Criteria PDFTuấn Mai vănNo ratings yet
- Nursing Cheat LabValuesDocument4 pagesNursing Cheat LabValuessasukenoneko100% (5)
- RSPH Level 4 Award in Haccp Management For Food ManufacturingDocument19 pagesRSPH Level 4 Award in Haccp Management For Food ManufacturingHema HemaNo ratings yet
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- Respiratory-Equations (Adam Hollingworth)Document4 pagesRespiratory-Equations (Adam Hollingworth)PkernNo ratings yet
- Answer Diagnosis: 1. RhythmDocument2 pagesAnswer Diagnosis: 1. RhythmSuggula Vamsi KrishnaNo ratings yet
- EKG RhythmsDocument10 pagesEKG RhythmsQueenNo ratings yet
- MK Combined PDFDocument93 pagesMK Combined PDFAnkit ChoudharyNo ratings yet
- Soap Note Example 3Document11 pagesSoap Note Example 3LorrieNo ratings yet
- Dysrhythmias Nursing InterventionsDocument7 pagesDysrhythmias Nursing InterventionsGail Lian Santos100% (1)
- ELECTROCARDIOGRAM by Aldrin Jayson AlmadenDocument23 pagesELECTROCARDIOGRAM by Aldrin Jayson AlmadenItsMe AJNo ratings yet
- Bundle Branch BlockDocument37 pagesBundle Branch BlocksyukronchalimNo ratings yet
- Warfarin: Prof DR Shah MuradDocument63 pagesWarfarin: Prof DR Shah Muradshahmurad653376No ratings yet
- 100 Beats Per Minute. Many DifferentDocument4 pages100 Beats Per Minute. Many Differentjovan teopizNo ratings yet
- Classification of MurmursDocument2 pagesClassification of MurmursNazneen SiddiquiNo ratings yet
- Ecg Crit - CareDocument55 pagesEcg Crit - CarekrismatactayNo ratings yet
- CardiomyopathyDocument8 pagesCardiomyopathyKarisaNo ratings yet
- Nephrologi NotesDocument43 pagesNephrologi NotesSigit Harya HutamaNo ratings yet
- HaematologyDocument28 pagesHaematologyfh fgNo ratings yet
- Key AnatomyDocument12 pagesKey Anatomyjoedeegan_No ratings yet
- Arteriolar Dilator Decreases After Load Ejection FractionDocument1 pageArteriolar Dilator Decreases After Load Ejection FractionJack GuccioneNo ratings yet
- Concise SEO-Optimized Title for Clotting DocumentDocument3 pagesConcise SEO-Optimized Title for Clotting DocumentRyan TurnerNo ratings yet
- NCM 103 (LEC) : Electrocardiogram (ECG) ElectrocardiogramDocument10 pagesNCM 103 (LEC) : Electrocardiogram (ECG) ElectrocardiogramJohn Protacio50% (2)
- Heart Failure RevisionDocument4 pagesHeart Failure RevisionBlanaid MargaretNo ratings yet
- Medicowesome - AnatomyDocument19 pagesMedicowesome - AnatomySubhashNo ratings yet
- Basic Medical Wide QRS ArrhythmiaDocument39 pagesBasic Medical Wide QRS ArrhythmiaJee JunpyoNo ratings yet
- (PED2) 3.03 Pediatric Hematology - Castro (Final V.2)Document25 pages(PED2) 3.03 Pediatric Hematology - Castro (Final V.2)Sam MataNo ratings yet
- Post-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeDocument5 pagesPost-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeEben Ezar Dela CruzNo ratings yet
- Pleural Infection - Past, Present, and Future DirectionsDocument15 pagesPleural Infection - Past, Present, and Future DirectionsCamilo VidalNo ratings yet
- Lec 2 - Blood VesselsDocument12 pagesLec 2 - Blood VesselsJeffrey LübbertNo ratings yet
- Examination of The Central Nervous SystemDocument3 pagesExamination of The Central Nervous Systemkenners100% (13)
- Warfarin Q and ADocument40 pagesWarfarin Q and AAbdul-Rhman Hamdy KishkNo ratings yet
- ECG ReviewDocument146 pagesECG ReviewThea DinoNo ratings yet
- FUN1 Pharmacology TableDocument10 pagesFUN1 Pharmacology TableRebecca MarshallNo ratings yet
- Normal Lab Values (USMLE Step 1)Document12 pagesNormal Lab Values (USMLE Step 1)nmp274No ratings yet
- IVMS Classic Cause-Findings Flash FactsDocument1,214 pagesIVMS Classic Cause-Findings Flash FactsMarc Imhotep Cray, M.D.No ratings yet
- Cardiology HX - PEDocument34 pagesCardiology HX - PEjjNo ratings yet
- Glutamate: Neurotransmitters Disturbed Increased Sympathetic Stimulation Increased Autonomic StimulationDocument3 pagesGlutamate: Neurotransmitters Disturbed Increased Sympathetic Stimulation Increased Autonomic StimulationCM NajitoNo ratings yet
- CVS Examination EditedDocument134 pagesCVS Examination EditedThilak JayalathNo ratings yet
- Harrison tables Raynaud's classification amyloid proteins IBD geneticsDocument5 pagesHarrison tables Raynaud's classification amyloid proteins IBD geneticsSANTHILAL ADHIKARLANo ratings yet
- Chapter 1 Compatible ModeDocument93 pagesChapter 1 Compatible ModeJyha KhariNo ratings yet
- CVA or StrokeDocument14 pagesCVA or StrokeJoenalyn AliguinNo ratings yet
- Patent Ductus Arteriosus 6. Aortic Stenosis: Signs and Symptoms: Signs and SymptomsDocument3 pagesPatent Ductus Arteriosus 6. Aortic Stenosis: Signs and Symptoms: Signs and SymptomsKIANA LOUISE ROMANONo ratings yet
- Medication Error 2017Document51 pagesMedication Error 2017Christina100% (1)
- Acute Coronary Syndrome: Case PresentationDocument4 pagesAcute Coronary Syndrome: Case PresentationJunathan L. DelgadoNo ratings yet
- Subject Sub-Subject Topic NameDocument6 pagesSubject Sub-Subject Topic NameHemanth Manikanta Sai PosaNo ratings yet
- Liver & PancreasDocument3 pagesLiver & Pancreasameerabest100% (1)
- Step-Wise Approaches in Clinical Examination - SampleDocument8 pagesStep-Wise Approaches in Clinical Examination - Samplecsbully913No ratings yet
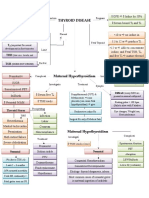
- Thyroid DiseaseDocument1 pageThyroid DiseaseZiyadNo ratings yet
- Genetics Dysmorphology in Pediatrics - MedicoNotesDocument1 pageGenetics Dysmorphology in Pediatrics - MedicoNotesJ KPNo ratings yet
- Name: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionDocument46 pagesName: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionAbdirahman Abdillahi FarahNo ratings yet
- Differential Diagnosis of Valvular Heart DiseaseDocument10 pagesDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNo ratings yet
- Nephrology Review NotesDocument6 pagesNephrology Review NotesEdilberto HernandezNo ratings yet
- DIT Pharmacology MnemonicsDocument5 pagesDIT Pharmacology MnemonicsqiqizNo ratings yet
- Anatomy Shelf Notes Dw9Document200 pagesAnatomy Shelf Notes Dw9Zain ul abedinNo ratings yet
- Diabetes diagnosis and managementDocument25 pagesDiabetes diagnosis and managementjljoioiuNo ratings yet
- Peripheral Vascular Medicine - Dr. Deduyo PDFDocument14 pagesPeripheral Vascular Medicine - Dr. Deduyo PDFMedisina101No ratings yet
- Toronto Notes Nephrology 2015 22Document1 pageToronto Notes Nephrology 2015 22JUSASB0% (1)
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Electrolyte Imbalances: Causes, Signs, Symptoms and InterventionsDocument6 pagesElectrolyte Imbalances: Causes, Signs, Symptoms and InterventionsmkninnyNo ratings yet
- Conduction System: Rhythm Identification and TreatmentDocument12 pagesConduction System: Rhythm Identification and Treatmenthops23No ratings yet
- IM Part 1 and 2 CombinedDocument100 pagesIM Part 1 and 2 CombinedsasghfdgNo ratings yet
- How To: Read ECG?Document63 pagesHow To: Read ECG?Let BNo ratings yet
- Cardiac Rhythms and Dysrhythmias GuideDocument14 pagesCardiac Rhythms and Dysrhythmias GuideShawn Gaurav Jha100% (1)
- Cardiac Dysrhythmias For Heart PatientsDocument3 pagesCardiac Dysrhythmias For Heart PatientsAlaa OmarNo ratings yet
- DocumentDocument2 pagesDocumentWilbert GuerreroNo ratings yet
- Bioterrorism Nursing CE Course: 4.0 Ancc Contact Hours Aacn Category ADocument41 pagesBioterrorism Nursing CE Course: 4.0 Ancc Contact Hours Aacn Category AWilbert GuerreroNo ratings yet
- Band 8 SampleDocument16 pagesBand 8 SampleWilbert GuerreroNo ratings yet
- Tularemia: Section NavigationDocument3 pagesTularemia: Section NavigationWilbert GuerreroNo ratings yet
- Med ListDocument4 pagesMed ListCrystal MalicatNo ratings yet
- Plague: Section NavigationsymptomsDocument3 pagesPlague: Section NavigationsymptomsWilbert GuerreroNo ratings yet
- Bricks Process - Docx Version 1Document2 pagesBricks Process - Docx Version 1Wilbert GuerreroNo ratings yet
- Liz Essay Jan-Sep 2019Document10 pagesLiz Essay Jan-Sep 2019Wilbert GuerreroNo ratings yet
- Work Experience Sheet for Supervising PositionsDocument2 pagesWork Experience Sheet for Supervising PositionsCes Camello100% (1)
- Lbs MSD CV Format 2017Document9 pagesLbs MSD CV Format 2017DivinaNo ratings yet
- ANormal Values Saunders 6th, 7th, Uworld 2017 Jimir .Doc Version 1Document4 pagesANormal Values Saunders 6th, 7th, Uworld 2017 Jimir .Doc Version 1Wilbert GuerreroNo ratings yet
- Pressure InjuryDocument7 pagesPressure InjuryWilbert GuerreroNo ratings yet
- Lbs MSD CV Format 2017Document9 pagesLbs MSD CV Format 2017DivinaNo ratings yet
- IELTS Enquiry On Results Form Part A: Notes For Candidates On The Submission of Enquiries On Results (EOR)Document1 pageIELTS Enquiry On Results Form Part A: Notes For Candidates On The Submission of Enquiries On Results (EOR)Ayesha NoorNo ratings yet
- PositioningDocument1 pagePositioningWilbert GuerreroNo ratings yet
- ImmuneDocument5 pagesImmuneJayvee Montoya-PujanteNo ratings yet
- ANormal Values Saunders 6th, 7th, Uworld 2017 Jimir .Doc Version 1Document4 pagesANormal Values Saunders 6th, 7th, Uworld 2017 Jimir .Doc Version 1Wilbert GuerreroNo ratings yet
- Menstrual Cycle: From Wikipedia, The Free EncyclopediaDocument18 pagesMenstrual Cycle: From Wikipedia, The Free EncyclopediaZACHARIAH MANKIRNo ratings yet
- Mental NclexDocument14 pagesMental NclexJayvee Montoya-PujanteNo ratings yet
- U World ReproductiveDocument5 pagesU World ReproductiveAce LabosNo ratings yet
- U World Renal-Urinary FinalDocument7 pagesU World Renal-Urinary FinalNoel CabamonganNo ratings yet
- 5th Grade Reading Comprehension Worksheets - Fifth Grade Week 4Document2 pages5th Grade Reading Comprehension Worksheets - Fifth Grade Week 4Julius CesarNo ratings yet
- Adime 2Document13 pagesAdime 2api-496164982No ratings yet
- Malignant Self LoveDocument7 pagesMalignant Self LoveMarjoryStewartBaxterNo ratings yet
- D&D 5E - Homebrew - Class ProfligateDocument7 pagesD&D 5E - Homebrew - Class Profligate19931214No ratings yet
- Acute Respiratory InfectionsDocument26 pagesAcute Respiratory InfectionsSuneel SagareNo ratings yet
- Project Report On Health & Safety PDFDocument3 pagesProject Report On Health & Safety PDFAakash SolankiNo ratings yet
- Implementing programs and projects for disaster risk managementDocument58 pagesImplementing programs and projects for disaster risk managementImtiaze Shafin RehadNo ratings yet
- PhobiasDocument4 pagesPhobiasOti VuraNo ratings yet
- Triethanolamine Safety ReportDocument6 pagesTriethanolamine Safety ReportMaria Inês HarrisNo ratings yet
- Test Bank For Burtons Microbiology For The Health Sciences 9 North Americanth Edition Paul G EngelkirkDocument10 pagesTest Bank For Burtons Microbiology For The Health Sciences 9 North Americanth Edition Paul G Engelkirkraphaelsophiep9f9100% (22)
- Adult Male and Female Height To Weight Ratio Chart PDFDocument4 pagesAdult Male and Female Height To Weight Ratio Chart PDFAkd DeshmukhNo ratings yet
- Cover Letter For Epidemiologist PositionDocument7 pagesCover Letter For Epidemiologist Positiongt7gb636100% (1)
- Pianakafinal Sa Lahatt RyannDocument14 pagesPianakafinal Sa Lahatt RyannPaul IglesiasNo ratings yet
- HISTORIA DE LA ORTODONCIADocument9 pagesHISTORIA DE LA ORTODONCIAcarmonao.carina94No ratings yet
- International Journal of Obstetric AnesthesiaDocument6 pagesInternational Journal of Obstetric Anesthesiaanita pratiwiNo ratings yet
- Behavioral Perspective On Mental Health and IllnessDocument12 pagesBehavioral Perspective On Mental Health and IllnessMonisha LakshminarayananNo ratings yet
- Depression Associated With Dementia With Lewy Bodies (DLB) and The Effect of SomatotherapyDocument6 pagesDepression Associated With Dementia With Lewy Bodies (DLB) and The Effect of SomatotherapyRaluca ElenaNo ratings yet
- Final Alcance Lis524Document112 pagesFinal Alcance Lis524Khristine alcanceNo ratings yet
- Denah Mixed Use LT 3 &4Document1 pageDenah Mixed Use LT 3 &4Jennifer MadenNo ratings yet
- English Passion Project 2Document9 pagesEnglish Passion Project 2api-462335192No ratings yet
- CLASSIC ARTICLE-Evaluation of The Factors Necessary To Develop Stability in Mandibular Dentures-Corwin R. WrightDocument10 pagesCLASSIC ARTICLE-Evaluation of The Factors Necessary To Develop Stability in Mandibular Dentures-Corwin R. WrightChander UdheyNo ratings yet
- ArbomapDocument1 pageArbomapNEWS CENTER MaineNo ratings yet
- Implementing of Rewards and Punishments Toward Students' Motivation in ELDocument13 pagesImplementing of Rewards and Punishments Toward Students' Motivation in ELAriska ChikaNo ratings yet
- CT 19 PropositionsDocument2 pagesCT 19 PropositionsGentlemen PowerNo ratings yet
- CWTS ProposalDocument5 pagesCWTS ProposalAllana de CastroNo ratings yet
- Cusa (Cavitron Ultrasonic Surgical Aspirator) "The New Armour of Periodontal Therapy"Document4 pagesCusa (Cavitron Ultrasonic Surgical Aspirator) "The New Armour of Periodontal Therapy"International Journal of Innovative Science and Research TechnologyNo ratings yet
- Cancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasDocument5 pagesCancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet