You might also like
- Neurosurgery - Specific Considerations - Schwartz's Principles of Surgery ABSITE and Board Review, 9th EdDocument17 pagesNeurosurgery - Specific Considerations - Schwartz's Principles of Surgery ABSITE and Board Review, 9th Edvnnv101.raceacNo ratings yet
- Ap Psychology Multiple Choice QuestionsDocument9 pagesAp Psychology Multiple Choice Questionsapi-319829528No ratings yet
- Nursing Care Plan (COPD - IMBALANCE NUTRITION)Document2 pagesNursing Care Plan (COPD - IMBALANCE NUTRITION)Kathleen MartinezNo ratings yet
- Typical Signs and Symptoms of Psychiatric Illness DefinedDocument6 pagesTypical Signs and Symptoms of Psychiatric Illness DefinedElijah Manuel BibayNo ratings yet
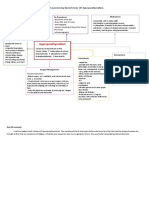
- List, Prioritize, Discuss Care For Patients Suffering An Acute Critical Neuro Emergency. Pick A Condition From This Chapter. and Create A Quick Concept MapDocument2 pagesList, Prioritize, Discuss Care For Patients Suffering An Acute Critical Neuro Emergency. Pick A Condition From This Chapter. and Create A Quick Concept MappsyNo ratings yet
- Risk For AspirationDocument2 pagesRisk For AspirationErica FabrigasNo ratings yet
- NCM 116 - RLE Activity#1 - VALDEZ PDFDocument6 pagesNCM 116 - RLE Activity#1 - VALDEZ PDFDexel Lorren ValdezNo ratings yet
- Delirium Screening PRISMEDocument1 pageDelirium Screening PRISMEWardah Fauziah El SofwanNo ratings yet
- Myasthenia GravisDocument18 pagesMyasthenia GravismarthanyalangluonyNo ratings yet
- HTP Tonic Clonic Seizure NeuroWardDocument5 pagesHTP Tonic Clonic Seizure NeuroWardMeryville JacildoNo ratings yet
- NCPDocument9 pagesNCPHendy Hency YunusNo ratings yet
- Drug Study-PsychDocument5 pagesDrug Study-Psychrc_lacampuinganyahooNo ratings yet
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosNo ratings yet
- Nursing Care Plan UlcerDocument2 pagesNursing Care Plan Ulcerxrampley2100% (2)
- Nursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationMarivic Yuson MalagarNo ratings yet
- Nursing Care Plan For Post Thyroidectomy and CholecystectomyDocument9 pagesNursing Care Plan For Post Thyroidectomy and Cholecystectomyirish m magracia100% (7)
- PantoprazoleDocument1 pagePantoprazolehahahahaaaaaaaNo ratings yet
- NcpsDocument10 pagesNcpskotoirNo ratings yet
- NCM 116 - Medical Surgical Nursing Lecture 01/26/2023: Spiritual CareDocument6 pagesNCM 116 - Medical Surgical Nursing Lecture 01/26/2023: Spiritual CareIvan A. EleginoNo ratings yet
- Case AnalysisDocument10 pagesCase AnalysisJuvida, Clarissa A.No ratings yet
- 6 - Et - Lect - Basic Concepts and Principles of Diet TheraphyDocument4 pages6 - Et - Lect - Basic Concepts and Principles of Diet TheraphyMa Ellen LumauagNo ratings yet
- Xiii. Discharge Planning: Carbohydrates NutrientsDocument4 pagesXiii. Discharge Planning: Carbohydrates Nutrientsgroupbsection1No ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- Marjorie ncp8Document2 pagesMarjorie ncp8Jovel CortezNo ratings yet
- Mental Health Anorexia NervosaDocument20 pagesMental Health Anorexia NervosaregisterednurseNo ratings yet
- Drug Study 5-14-23Document5 pagesDrug Study 5-14-23Daniela Villanueva RosalNo ratings yet
- NCM 116 Medical SurgicalDocument9 pagesNCM 116 Medical SurgicalIvan A. EleginoNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocument11 pagesAssessment Diagnosis Planning Implementation Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- KardexxxDocument3 pagesKardexxxمنوعات قرآن واحاديث واخبار وكرة قدمNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanKabang MoaNo ratings yet
- Assessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKSDocument3 pagesAssessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKStflorenzNo ratings yet
- Sian Selario HypertensionDocument2 pagesSian Selario HypertensionMaria Rosario Pangilinan SagmitNo ratings yet
- Parkinson's Disease Discharge PlanDocument2 pagesParkinson's Disease Discharge PlanCristine Joy Alarcon MonteroNo ratings yet
- Handout Therapy Increased Intestinal Permeability ClinicianDocument2 pagesHandout Therapy Increased Intestinal Permeability ClinicianThe Machi WellnessNo ratings yet
- Need/Nursing Diagnosis/Cues Need: Physiologic Need Nursing Diagnosis: - Nutrition ImbalancedDocument1 pageNeed/Nursing Diagnosis/Cues Need: Physiologic Need Nursing Diagnosis: - Nutrition ImbalancedmawelNo ratings yet
- Geria FinalsDocument14 pagesGeria FinalsAlliah RodriguezNo ratings yet
- Geria UNIT 3Document5 pagesGeria UNIT 3Raiden VizcondeNo ratings yet
- COLON CANCER NCP-impaired nutrITIONDocument3 pagesCOLON CANCER NCP-impaired nutrITIONNicole cuencosNo ratings yet
- Intuitive Eating in Treatment of Eating Disorders by Evelyn Tribole, MS, RDDocument5 pagesIntuitive Eating in Treatment of Eating Disorders by Evelyn Tribole, MS, RDEvelyn Tribole, MS, RD100% (1)
- 88 FinalDocument4 pages88 FinalEshiebel OrganistaNo ratings yet
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- BARANDINO, Jia Laurice (Gouty Arthritis)Document18 pagesBARANDINO, Jia Laurice (Gouty Arthritis)Deinielle Magdangal RomeroNo ratings yet
- NURSING CARE PLAN (For Case Study)Document2 pagesNURSING CARE PLAN (For Case Study)Kathleen Martinez100% (1)
- Eating DisordersDocument3 pagesEating DisordersJim Louise C. GALANGNo ratings yet
- SBS Management 01Document1 pageSBS Management 01Daniel RuizNo ratings yet
- Good Practices, Foods, and Nutrition For The Brain: Journal of Health Informatics & ManagementDocument2 pagesGood Practices, Foods, and Nutrition For The Brain: Journal of Health Informatics & ManagementRebecacel PalattaoNo ratings yet
- Prenatal Care Common Discomforts During PregnancyDocument5 pagesPrenatal Care Common Discomforts During PregnancyKarina MadriagaNo ratings yet
- Assessment Diagnosis Rationale Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Rationale Planning Intervention Rationale EvaluationMonica RamboyongNo ratings yet
- Cardaic Emergency Drugs.Document13 pagesCardaic Emergency Drugs.Alma SusanNo ratings yet
- CALCITRIOLDocument2 pagesCALCITRIOLdesshe09No ratings yet
- Total Parenteral NutritionDocument59 pagesTotal Parenteral NutritionMARIAH ALEXIE GASALNo ratings yet
- Ni LUNADocument17 pagesNi LUNAjimwelluismNo ratings yet
- Activity 5 NCPDocument5 pagesActivity 5 NCPAl-Mujib TanogNo ratings yet
- Gestational Diabetes NCP SelDocument1 pageGestational Diabetes NCP Selcherrymae mata60% (5)
- BASIC - Sedation Nutrition Prophylaxis 2019Document33 pagesBASIC - Sedation Nutrition Prophylaxis 2019dragon66No ratings yet
- Nursing Care Plan - CancerDocument3 pagesNursing Care Plan - CancerChristineAla0% (1)
- Diarrhea (AGE)Document2 pagesDiarrhea (AGE)NursesLabs.com100% (1)
- HTPDocument4 pagesHTPAlyssa Jade SandovalNo ratings yet
- Lecture-In-P e - Q2Document6 pagesLecture-In-P e - Q2Thirdee SumilongNo ratings yet
- LIVER CIRRHOSIS - SeminarrDocument12 pagesLIVER CIRRHOSIS - Seminarrعمار ياسرNo ratings yet
- Sian Selario HypertensionDocument2 pagesSian Selario HypertensionMaria Rosario Pangilinan SagmitNo ratings yet
- Dave CourseworkDocument7 pagesDave CourseworkTrisha Isobel DaveNo ratings yet
- Transform Your Body and Mind with Intermittent Fasting: A Comprehensive GuideFrom EverandTransform Your Body and Mind with Intermittent Fasting: A Comprehensive GuideNo ratings yet
- Intermittent Fasting For Women: A Beginner’s Transformation Made EasyFrom EverandIntermittent Fasting For Women: A Beginner’s Transformation Made EasyNo ratings yet
- ParkinsonsDocument2 pagesParkinsonspsyNo ratings yet
- Anaphylactic Shock Due To Contrast Dye Allergy HF Due To Left Ventricle Damage and MIDocument3 pagesAnaphylactic Shock Due To Contrast Dye Allergy HF Due To Left Ventricle Damage and MIpsyNo ratings yet
- ParkinsonsDocument2 pagesParkinsonspsyNo ratings yet
- ECG Description:: Ventricular FibrillationDocument2 pagesECG Description:: Ventricular FibrillationpsyNo ratings yet
- Physiological Integrity: Draw A Quick Concept Map Comparing Right Vs Left Heart FailureDocument1 pagePhysiological Integrity: Draw A Quick Concept Map Comparing Right Vs Left Heart FailurepsyNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- Neuro AgingDocument1 pageNeuro AgingpsyNo ratings yet
- HyperparathyroidismDocument2 pagesHyperparathyroidismpsyNo ratings yet
- Gather Patient HistoryDocument1 pageGather Patient HistorypsyNo ratings yet
- Nutrition Self-Monitored Blood GlucoseDocument3 pagesNutrition Self-Monitored Blood GlucosepsyNo ratings yet
- A Review On Atopic Dermatitis Etiology, Clinical Features, Pathogenesis, Diagnosis, and Various TreatmentsDocument12 pagesA Review On Atopic Dermatitis Etiology, Clinical Features, Pathogenesis, Diagnosis, and Various TreatmentsEditor IJTSRDNo ratings yet
- CNS Infection - NelsonDocument13 pagesCNS Infection - Nelsonsai saiNo ratings yet
- Nursing Care of A Child With Respiratory DisorderDocument69 pagesNursing Care of A Child With Respiratory DisorderTamil Villardo100% (1)
- Short Course - Virology & MycologyDocument1 pageShort Course - Virology & MycologyDamian HamzahNo ratings yet
- Devarajan, Dss DGN ArdsDocument4 pagesDevarajan, Dss DGN ArdsrantiadrianiNo ratings yet
- Introduction To Pain: MakassarDocument55 pagesIntroduction To Pain: MakassarNizwan ShamNo ratings yet
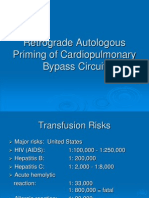
- Retrograde Autologous Priming of Cardiopulmonary Bypass CircuitDocument18 pagesRetrograde Autologous Priming of Cardiopulmonary Bypass CircuitMuhammad Badrushshalih100% (2)
- Infectious Diseases Oral RevalidaDocument22 pagesInfectious Diseases Oral RevalidaShella Mae UsquisaNo ratings yet
- Oral Thrush CausesDocument7 pagesOral Thrush CausesMichael Eka PutraNo ratings yet
- 3aatrialrhythms 110624075109 Phpapp02Document35 pages3aatrialrhythms 110624075109 Phpapp02Win Ichda AlfahleviNo ratings yet
- Wa0006Document30 pagesWa0006rushaliNo ratings yet
- Effectiveness of Manual Therapy On Chronic Pelvic PainDocument41 pagesEffectiveness of Manual Therapy On Chronic Pelvic PainMuhammadRizalN100% (1)
- Practice Questions 1 - YoungDocument12 pagesPractice Questions 1 - Youngejyoung928100% (1)
- Acute Kidney Injury (Acute Renal Failure) in Pregnancy - UpToDateDocument15 pagesAcute Kidney Injury (Acute Renal Failure) in Pregnancy - UpToDateZurya UdayanaNo ratings yet
- Cao Et Al-2013-Cochrane Database of Systematic ReviewsDocument30 pagesCao Et Al-2013-Cochrane Database of Systematic ReviewsIRMÃOS FOREVERNo ratings yet
- Systematic Review of Anti-Inflammatory Properties of Phyllanthus NiruriDocument4 pagesSystematic Review of Anti-Inflammatory Properties of Phyllanthus NiruriInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Medicinenet: Labor and Delivery Early and Later Signs of Labor ApproachingDocument27 pagesMedicinenet: Labor and Delivery Early and Later Signs of Labor ApproachingNamal No OorNo ratings yet
- Chapter 44: Nursing Care of The Client With An Hematologic DisordersDocument18 pagesChapter 44: Nursing Care of The Client With An Hematologic DisordersfLOR_ZIANE_MAENo ratings yet
- Clinicosocial Case Presentation PGI Gloria and Rompal 1Document42 pagesClinicosocial Case Presentation PGI Gloria and Rompal 1Jane GarciaNo ratings yet
- Actinobacillosis &actinomycosisDocument16 pagesActinobacillosis &actinomycosisVickypathoNo ratings yet
- Skills - Open Fracture ManagementDocument4 pagesSkills - Open Fracture ManagementFelixNo ratings yet
- CamaristaCM - HIV and AIDS (Questions and Answers)Document5 pagesCamaristaCM - HIV and AIDS (Questions and Answers)Coleen Mae CamaristaNo ratings yet
- Nursing Care Plan: CirrhosisDocument11 pagesNursing Care Plan: CirrhosisneuronurseNo ratings yet
- Assignment - HypertensionDocument6 pagesAssignment - HypertensionAyessa Salazar100% (2)
- Low Back Pain and Associated Risk Factors Among.8Document6 pagesLow Back Pain and Associated Risk Factors Among.8Teti HLCNo ratings yet
- Guideline. Rectal Cancer Version 2-2018.NCCN Clinical PracticeDocument29 pagesGuideline. Rectal Cancer Version 2-2018.NCCN Clinical PracticeTrí Cương NguyễnNo ratings yet
- Nihms 1519559Document20 pagesNihms 1519559SibaraniNo ratings yet