You might also like
- Clinical Ophthalmology for UndergraduatesFrom EverandClinical Ophthalmology for UndergraduatesRating: 4 out of 5 stars4/5 (5)
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae TumNo ratings yet
- 1 - MyopiaDocument9 pages1 - MyopiaSpislgal PhilipNo ratings yet
- Acute Kidney InjuryDocument4 pagesAcute Kidney Injuryjumi jumdailNo ratings yet
- CA Eye and Ear DisorderDocument20 pagesCA Eye and Ear DisorderEsmareldah Henry Sirue100% (1)
- Dsa Cerebral AngiographyDocument20 pagesDsa Cerebral AngiographyLalaine De JesusNo ratings yet
- Positron Emission TomographyDocument2 pagesPositron Emission TomographyRadlinkSingaporeNo ratings yet
- Introduction To TCCC ASM Didactic Presentation (With Videos)Document43 pagesIntroduction To TCCC ASM Didactic Presentation (With Videos)thallesnetNo ratings yet
- Dry Eye: the Hidden Health Hazard: For Computer Users Concerned About Eye HealthFrom EverandDry Eye: the Hidden Health Hazard: For Computer Users Concerned About Eye HealthNo ratings yet
- TCCC Eye Injury CareDocument5 pagesTCCC Eye Injury CareSae TumNo ratings yet
- Eye Injuries: Skill InstructionsDocument3 pagesEye Injuries: Skill InstructionsSae TumNo ratings yet
- 14 - Eye InjuriesDocument4 pages14 - Eye InjuriesCarlos MaravilhaNo ratings yet
- Module 13: Eye Injuries: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document16 pagesModule 13: Eye Injuries: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Luis-alfredo Perez Bolde HernandezNo ratings yet
- Safety Talk For Painting WorkDocument3 pagesSafety Talk For Painting WorkBashir KhanNo ratings yet
- 5 Min ProtectingSight 10Document3 pages5 Min ProtectingSight 10Ani videozNo ratings yet
- Case Study Eyes 11Document2 pagesCase Study Eyes 11Carla May CaraNo ratings yet
- Patient Instruction Guide: Vistakon (Etafilcon A) Contact LensesDocument17 pagesPatient Instruction Guide: Vistakon (Etafilcon A) Contact LensessanieregianeeNo ratings yet
- Eye Trauma: Brief IntroductionDocument16 pagesEye Trauma: Brief IntroductionOchi D. GreenNo ratings yet
- Patient Instruction Guide: Vistakon (Galyfilcon A) Contact LensesDocument24 pagesPatient Instruction Guide: Vistakon (Galyfilcon A) Contact LensesTINALEETNT723No ratings yet
- TB 21 Eye Safety EngDocument1 pageTB 21 Eye Safety EngHSE 1No ratings yet
- Asm Course Speaker NotesDocument15 pagesAsm Course Speaker NotesJesse RobertNo ratings yet
- Ppe Eye and Face ProtectionDocument2 pagesPpe Eye and Face ProtectionMunaku TafadzwaNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- Eyes Wide Split - Managing Penetrating Eye TraumaDocument6 pagesEyes Wide Split - Managing Penetrating Eye Traumasen ANo ratings yet
- Module 02 - Medical Equipment: Speaker NotesDocument7 pagesModule 02 - Medical Equipment: Speaker NotesDERIL PRASETYONo ratings yet
- Module 02 - Medical Equipment: Speaker NotesDocument7 pagesModule 02 - Medical Equipment: Speaker NotesDERIL PRASETYONo ratings yet
- CPG Eye InjuryDocument4 pagesCPG Eye InjuryManuel AlvarezNo ratings yet
- Eye Injuries: Worksafe Western AustraliaDocument5 pagesEye Injuries: Worksafe Western AustraliaaezeadNo ratings yet
- ST073 - Text - Eye Damage Prevention 010301Document13 pagesST073 - Text - Eye Damage Prevention 010301malik jahanNo ratings yet
- Module 07 - Airway Management in TFC: Speaker NotesDocument7 pagesModule 07 - Airway Management in TFC: Speaker NotesSae TumNo ratings yet
- CRSTEurope Practical Management of A Dropped NucleusDocument1 pageCRSTEurope Practical Management of A Dropped NucleusCalvinNo ratings yet
- ICU Eye Care Guidelines for Preventing DiseaseDocument6 pagesICU Eye Care Guidelines for Preventing DiseaseKiki dwi PratiwiNo ratings yet
- Eye Injuries and PreventionDocument2 pagesEye Injuries and PreventionSher DilNo ratings yet
- Hand Injury PreventionDocument5 pagesHand Injury PreventionCarlos Andre Soares SantosNo ratings yet
- 20_SurpriseStartleResilienceDocument33 pages20_SurpriseStartleResilienceHani BoudiafNo ratings yet
- SOS-Saving Our Sight: Safety EyewearDocument3 pagesSOS-Saving Our Sight: Safety EyewearSantos RexNo ratings yet
- Ocular Injuries - A Review: VN SukatiDocument9 pagesOcular Injuries - A Review: VN SukatiDede GunawanNo ratings yet
- 05 DamageEye2017Document6 pages05 DamageEye2017sudhirksingh27No ratings yet
- What Is PPE (Personal Protective Equipment) - The PM HQ PDFDocument18 pagesWhat Is PPE (Personal Protective Equipment) - The PM HQ PDFshreyas100% (1)
- Module 03 - Care Under Fire: Speaker NotesDocument12 pagesModule 03 - Care Under Fire: Speaker NotesSae TumNo ratings yet
- Eye Protection in The WorkplaceDocument3 pagesEye Protection in The WorkplaceVel MuruganNo ratings yet
- 6 Nonpenetrating Eye Injuries in Children2020Document13 pages6 Nonpenetrating Eye Injuries in Children2020Josue Enrique Jacobo MendozaNo ratings yet
- Workplace Eye Safety EssentialsDocument2 pagesWorkplace Eye Safety EssentialsRaza salaut RehmatNo ratings yet
- Eye Injury Prevention: WWW - Worksafesask.caDocument20 pagesEye Injury Prevention: WWW - Worksafesask.cafrancisNo ratings yet
- Eye and Face ProtectionDocument34 pagesEye and Face ProtectionDriss EddeniaNo ratings yet
- HPI - Workplace Occupational Health and SafetyDocument4 pagesHPI - Workplace Occupational Health and Safetyeuniceedina.riveroNo ratings yet
- 20 Questions Eye EmergenciesDocument4 pages20 Questions Eye EmergenciesZoe ZooNo ratings yet
- Trauma Suturing Techniques: Key PointsDocument10 pagesTrauma Suturing Techniques: Key PointsAstidya MirantiNo ratings yet
- Eye ProtectionDocument8 pagesEye ProtectionRaad AljuboryNo ratings yet
- EYE SAFETY TIPS TOOL BOX TALKDocument1 pageEYE SAFETY TIPS TOOL BOX TALKAl DubNo ratings yet
- EMEA V1 Tech-Data-Bulletin-192-Eye-Protection-For-Infectious-DiseaseDocument3 pagesEMEA V1 Tech-Data-Bulletin-192-Eye-Protection-For-Infectious-DiseaseHamidNo ratings yet
- An Even Bigger Danger: Contact Lenses Corneal UlcersDocument10 pagesAn Even Bigger Danger: Contact Lenses Corneal UlcersZa FranNo ratings yet
- Personal Protective Equipment - Eye and Face Protection: Risk Control Resources, LLC Printed On: 01/29/2009Document71 pagesPersonal Protective Equipment - Eye and Face Protection: Risk Control Resources, LLC Printed On: 01/29/2009M_E_AdamsNo ratings yet
- Uses of PpeDocument1 pageUses of Ppevishal aroraNo ratings yet
- 41 - Ocular TraumaDocument2 pages41 - Ocular TraumaChristine Danica BiteraNo ratings yet
- Eye SafetyDocument4 pagesEye Safetymnkoanyane16No ratings yet
- Eye Health in The WorkplaceDocument3 pagesEye Health in The WorkplaceMert Gencay ÖzdoğanNo ratings yet
- Eye Protection Safety TrainingDocument32 pagesEye Protection Safety TrainingImthiyaz MulkiNo ratings yet
- Proper Use and Care of Eye PPEDocument3 pagesProper Use and Care of Eye PPEJessicaNo ratings yet
- Prentice9e Im Chap22Document8 pagesPrentice9e Im Chap22api-281340024No ratings yet
- Eye Protection For Infection Control: US CDC/NIOSH RecommendationsDocument5 pagesEye Protection For Infection Control: US CDC/NIOSH RecommendationsPriskilla Grace TicoaluNo ratings yet
- Epiretinal Membrane MoorfieldsDocument4 pagesEpiretinal Membrane MoorfieldsAshley CheungNo ratings yet
- Eye Trauma - Doctor Print - Patient - Co.ukDocument10 pagesEye Trauma - Doctor Print - Patient - Co.ukbenitiyaNo ratings yet
- Foreign BodyDocument8 pagesForeign BodynusriniNo ratings yet
- Head-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedDocument1 pageHead-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedSae TumNo ratings yet
- Combat Lifesaver Guide to One-Person Bag Valve Mask VentilationDocument1 pageCombat Lifesaver Guide to One-Person Bag Valve Mask VentilationSae TumNo ratings yet
- Combat Lifesaver Guide to One-Person Bag Valve Mask VentilationDocument1 pageCombat Lifesaver Guide to One-Person Bag Valve Mask VentilationSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationDocument3 pagesSkills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationDocument2 pagesSkills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationSae TumNo ratings yet
- Combat lifesaver's one-handed tourniquet application guideDocument1 pageCombat lifesaver's one-handed tourniquet application guideSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Head-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedDocument1 pageHead-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedSae TumNo ratings yet
- One-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageOne-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Head-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedDocument1 pageHead-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedSae TumNo ratings yet
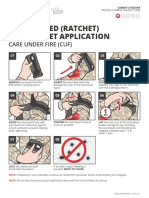
- Two-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageTwo-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Atbf Ista PDFDocument12 pagesAtbf Ista PDFSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Combat Lifesaver Drag and Carry TechniquesDocument5 pagesCombat Lifesaver Drag and Carry TechniquesSae TumNo ratings yet
- Module 03 - Care Under Fire: Speaker NotesDocument12 pagesModule 03 - Care Under Fire: Speaker NotesSae TumNo ratings yet
- Two-Person Drag/Carry: Kit or Arm DragDocument3 pagesTwo-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Evacuation Procedures: Skill InstructionsDocument3 pagesEvacuation Procedures: Skill InstructionsSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDocument7 pagesSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumNo ratings yet
- CLS Skill Instructions: Analgesia and Antibiotic AdministrationDocument3 pagesCLS Skill Instructions: Analgesia and Antibiotic AdministrationSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareDocument1 pageSkills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 7: Airway ManagementDocument6 pagesSkills Assessment Checklist: MODULE 7: Airway ManagementSae TumNo ratings yet
- Module 04 - Principles and Application of TFC: Speaker NotesDocument7 pagesModule 04 - Principles and Application of TFC: Speaker NotesSae TumNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae Tum0% (1)
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Chapter 411 - OsteoporosisDocument3 pagesChapter 411 - OsteoporosisgatNo ratings yet
- Research ArticleDocument9 pagesResearch ArticlebejarhasanNo ratings yet
- DRM 503 Final Requirement - Cruzat - Fontilar - Maravilla - Miranda - RelopezDocument12 pagesDRM 503 Final Requirement - Cruzat - Fontilar - Maravilla - Miranda - RelopezEy-ey ChioNo ratings yet
- Daftar Pustaka: Jakarta: Badan Penelitian Dan Pengembangan Kesehatan DepartemenDocument3 pagesDaftar Pustaka: Jakarta: Badan Penelitian Dan Pengembangan Kesehatan DepartemenAndrew SebastianNo ratings yet
- Effectiveness of Training Program On Community Based Psychosocial Disaster Preparedness For Community VolunteersDocument15 pagesEffectiveness of Training Program On Community Based Psychosocial Disaster Preparedness For Community VolunteersDivya ChokNo ratings yet
- Sports Script - 2021-22Document11 pagesSports Script - 2021-22Cool WritzNo ratings yet
- Carcinogenicity Assessment of Biologics: June 13, 2013Document41 pagesCarcinogenicity Assessment of Biologics: June 13, 2013claudedNo ratings yet
- General School Operations: 118.01 1 Updated 19 20 Wis. StatsDocument76 pagesGeneral School Operations: 118.01 1 Updated 19 20 Wis. Statsapi-271033247No ratings yet
- Blood Transfusion Reaction Vsim - Sept 16 22 NSGD 2106Document5 pagesBlood Transfusion Reaction Vsim - Sept 16 22 NSGD 2106api-631170779No ratings yet
- EMERGING INFECTION DISEASE CDCvol 24 No 8 2018 PDFDocument216 pagesEMERGING INFECTION DISEASE CDCvol 24 No 8 2018 PDFanyNo ratings yet
- Thesis msc40Document83 pagesThesis msc40Mominah MayamNo ratings yet
- Bma Specialty Doctor Specialist and Consultant Roles and Responsibilities Comparison Table Jul 2021Document1 pageBma Specialty Doctor Specialist and Consultant Roles and Responsibilities Comparison Table Jul 2021Shahab AnsariNo ratings yet
- Multiple SclerosisDocument3 pagesMultiple SclerosisCarmella CollantesNo ratings yet
- Four Handed DentistryDocument114 pagesFour Handed DentistryLie FelixNo ratings yet
- Introduction To The Principles of Food Hygiene and SafetyDocument15 pagesIntroduction To The Principles of Food Hygiene and SafetyYasiqyhaidarNo ratings yet
- Health CultureDocument26 pagesHealth CultureSeleccion de personaNo ratings yet
- 4 ADocument50 pages4 Aucnursingcesdev2008No ratings yet
- Joyce Et Al 2018.PMID - 29903782Document9 pagesJoyce Et Al 2018.PMID - 29903782Ara PalmaNo ratings yet
- Latihan Soal TERMINOLOGI MEDISDocument10 pagesLatihan Soal TERMINOLOGI MEDISdelia yuliantiNo ratings yet
- 11-12-21 COVID Vaccine Letter W-Consent FormDocument2 pages11-12-21 COVID Vaccine Letter W-Consent FormNewsChannel 9No ratings yet
- The Application of The Principles of ResDocument25 pagesThe Application of The Principles of Resphucnguyen.31221023675No ratings yet
- Module 6 - Sexual SelfDocument14 pagesModule 6 - Sexual SelfFlorence de LeonNo ratings yet
- Nursing ProcessDocument20 pagesNursing Processwideyatma100% (2)
- Total Quit KitDocument47 pagesTotal Quit Kitrahul.mishraNo ratings yet
- L51 - Home Collection KRL (Kolkata Reference Lab) Premises No - 031-0199 Plot No - CB 31/1 Street 199 Action Area 1C, KOLKATADocument3 pagesL51 - Home Collection KRL (Kolkata Reference Lab) Premises No - 031-0199 Plot No - CB 31/1 Street 199 Action Area 1C, KOLKATADebraj Das0% (1)
- School ViolenceDocument7 pagesSchool Violencekhalilmanai769No ratings yet
- Pregnancy BrochureDocument2 pagesPregnancy Brochureapi-464628523No ratings yet