You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Maternity Nursing!Document138 pagesMaternity Nursing!cheenapberber100% (2)
- Impaired Gas ExchangeDocument22 pagesImpaired Gas ExchangecheenapberberNo ratings yet
- NCM 101 Skills Finals: Care of Mother, Child and FamilyDocument38 pagesNCM 101 Skills Finals: Care of Mother, Child and FamilycheenapberberNo ratings yet
- Prehypertension: Average (And Ranges) Average (And Ranges)Document3 pagesPrehypertension: Average (And Ranges) Average (And Ranges)cheenapberberNo ratings yet
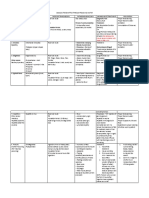
- Intranatal Table and InferenceDocument3 pagesIntranatal Table and InferencecheenapberberNo ratings yet
- Gerontological NursingDocument422 pagesGerontological Nursingcheenapberber100% (1)
- Hand Hygiene Why How and When BrochureDocument7 pagesHand Hygiene Why How and When BrochureLeis FatwaNo ratings yet
- CPDProgram Nurse 111919Document982 pagesCPDProgram Nurse 111919alchemist-at-lawNo ratings yet
- Geriatric Care: Presented by DR Nikhil Bansal J.N.M.C.,WardhaDocument99 pagesGeriatric Care: Presented by DR Nikhil Bansal J.N.M.C.,WardhacheenapberberNo ratings yet
- Management Trends, Issues and Problems: PresentersDocument26 pagesManagement Trends, Issues and Problems: PresenterscheenapberberNo ratings yet
- Theories of AgingDocument9 pagesTheories of AgingcheenapberberNo ratings yet
- CMO 15 S 2017 PDFDocument63 pagesCMO 15 S 2017 PDFJamal P. AlawiyaNo ratings yet
- Diseases Transmitted Through Food and WaterDocument2 pagesDiseases Transmitted Through Food and WatercheenapberberNo ratings yet
- 004 LabsDiagnosticsManualDocument64 pages004 LabsDiagnosticsManualRaju Niraula100% (1)
- Heart Anatomy & ECG InterpretationDocument3 pagesHeart Anatomy & ECG InterpretationcheenapberberNo ratings yet
- Gastrointestinal Diseases1Document17 pagesGastrointestinal Diseases1cheenapberberNo ratings yet
- Commonly Used Medical AbbreviationsDocument3 pagesCommonly Used Medical AbbreviationscheenapberberNo ratings yet
- Hand Hygiene Why How and When BrochureDocument7 pagesHand Hygiene Why How and When BrochureLeis FatwaNo ratings yet
- First AidDocument126 pagesFirst AidVishwanath SinduvadiNo ratings yet
- Diabetes Mellitus Prepared By: LORI R. LARA, R.NDocument14 pagesDiabetes Mellitus Prepared By: LORI R. LARA, R.NNovie Carla0% (1)
- Geria 2Document101 pagesGeria 2cheenapberberNo ratings yet
- CA1 '2 of 2' Funda 2019-2020Document164 pagesCA1 '2 of 2' Funda 2019-2020cheenapberberNo ratings yet
- PH Red Cross First Aid and BLSDocument71 pagesPH Red Cross First Aid and BLSctuagent74% (19)
- Fundamentals Notetaking1Document5 pagesFundamentals Notetaking1cheenapberberNo ratings yet
- General Considerations Prior To ActionDocument2 pagesGeneral Considerations Prior To ActioncheenapberberNo ratings yet
- Geria 1Document56 pagesGeria 1cheenapberberNo ratings yet
- The correct answer is a. A urine specimen obtained through catheterization is a random urine specimenDocument55 pagesThe correct answer is a. A urine specimen obtained through catheterization is a random urine specimencheenapberberNo ratings yet
- Heart FailureDocument1 pageHeart FailurecheenapberberNo ratings yet
- Theories of AgingDocument9 pagesTheories of AgingcheenapberberNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Foundations On Expansive Soils: 3.1. BackgroundDocument31 pagesFoundations On Expansive Soils: 3.1. BackgroundbiniNo ratings yet
- T2-1 MS PDFDocument27 pagesT2-1 MS PDFManav NairNo ratings yet
- PW 160-Taliban Fragmentation Fact Fiction and Future-PwDocument28 pagesPW 160-Taliban Fragmentation Fact Fiction and Future-Pwrickyricardo1922No ratings yet
- ANNEX III-Site Components Drawings SetDocument96 pagesANNEX III-Site Components Drawings SetDenice Erika ManzanoNo ratings yet
- Haloalkanes and Haloarenes Notes GoodDocument21 pagesHaloalkanes and Haloarenes Notes GoodAnitesh DharamNo ratings yet
- HORIZONTAL DISTRIBUTION OF FORCES - Part 1-2Document1 pageHORIZONTAL DISTRIBUTION OF FORCES - Part 1-2Inna PotesNo ratings yet
- 02.casebook - BLDG Repairs & Maint - Chapter 1 - 2011 (Water Seepage)Document13 pages02.casebook - BLDG Repairs & Maint - Chapter 1 - 2011 (Water Seepage)Hang kong TseNo ratings yet
- ORPHEUS by GRS Mead - Electronic Text EditionDocument199 pagesORPHEUS by GRS Mead - Electronic Text EditionMartin EuserNo ratings yet
- Electric Charges and Fields Bank of Board QuestionsDocument11 pagesElectric Charges and Fields Bank of Board QuestionsNishy GeorgeNo ratings yet
- GCS Activity 2003Document33 pagesGCS Activity 2003donnottryNo ratings yet
- Consumer Notebook Price List For September 2010Document4 pagesConsumer Notebook Price List For September 2010Anand AryaNo ratings yet
- Value YourselfDocument7 pagesValue YourselfTalha KhalidNo ratings yet
- A Rite of SpringDocument10 pagesA Rite of SpringLucius Gregory MeredithNo ratings yet
- The Separation of Coherent and Incoherent Compton X-Ray ScatteringDocument8 pagesThe Separation of Coherent and Incoherent Compton X-Ray ScatteringFaisal AmirNo ratings yet
- Top Answers to Mahout Interview QuestionsDocument6 pagesTop Answers to Mahout Interview QuestionsPappu KhanNo ratings yet
- Analysis On Forgery Patterns For GPS Civil Spoofing SignalsDocument4 pagesAnalysis On Forgery Patterns For GPS Civil Spoofing SignalsMadhu KrishnaNo ratings yet
- wizBRAINeng20 2Document4 pageswizBRAINeng20 2Deepika AgrawalNo ratings yet
- DP-10/DP-10T/DP-11/DP-15/DP-18 Digital Ultrasonic Diagnostic Imaging SystemDocument213 pagesDP-10/DP-10T/DP-11/DP-15/DP-18 Digital Ultrasonic Diagnostic Imaging SystemDaniel JuarezNo ratings yet
- AllareDocument16 pagesAllareGyaniNo ratings yet
- A Detailed Lesson Plan in (Teaching Science)Document8 pagesA Detailed Lesson Plan in (Teaching Science)Evan Jane Jumamil67% (3)
- The Secret Science of Shaktipat - Guide To Initiation 13 September 2020Document77 pagesThe Secret Science of Shaktipat - Guide To Initiation 13 September 2020Patrick JenksNo ratings yet
- GRP 10 JV'sDocument43 pagesGRP 10 JV'sManas ChaturvediNo ratings yet
- Articulos 2022-2Document11 pagesArticulos 2022-2Nilser Enrique Valle HernandezNo ratings yet
- My CV - Rose ChebetDocument5 pagesMy CV - Rose ChebetSammy WatimaNo ratings yet
- 4684Document2 pages4684Harish Kumar M0% (1)
- Kiro Urdin BookDocument189 pagesKiro Urdin BookDane BrdarskiNo ratings yet
- R4850G2 Rectifier Data Sheet 05Document2 pagesR4850G2 Rectifier Data Sheet 05PP CharlyNo ratings yet
- XII Class Assignment Programs 2023-24Document8 pagesXII Class Assignment Programs 2023-24Sudhir KumarNo ratings yet
- Mikes ResumeDocument2 pagesMikes Resumeapi-312645878No ratings yet