You might also like
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Impaired Gas ExchangeDocument3 pagesImpaired Gas ExchangeBenedicto RosalNo ratings yet
- Nursing Diagnosis Impaired Gas ExchangeDocument7 pagesNursing Diagnosis Impaired Gas ExchangeZycon Rodney Ae'zecquel Gachallan50% (2)
- Ineffective Airway Clearance Nursing Care PlanDocument2 pagesIneffective Airway Clearance Nursing Care Planrois romaNo ratings yet
- NCP Copd4Document15 pagesNCP Copd4Alessa Marie Crisostomo Salazar100% (1)
- Nursing Care PlanDocument22 pagesNursing Care PlanjamNo ratings yet
- Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDocument8 pagesWhich It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNo ratings yet
- Guaifenesin Drug CardDocument1 pageGuaifenesin Drug CardJessie JenningsNo ratings yet
- NCP BronchopneumoniaDocument8 pagesNCP BronchopneumoniaCrisantaCasliNo ratings yet
- Nursing Care Plans For UTIDocument2 pagesNursing Care Plans For UTIHannah Pin67% (3)
- Asthma Impaired Gas ExchangeDocument2 pagesAsthma Impaired Gas ExchangeNedeve Ozned100% (5)
- Nursing Care PlanDocument7 pagesNursing Care PlanRhitzle Ann100% (1)
- NCP For StokeDocument5 pagesNCP For StokeMemedNo ratings yet
- Ineffective Airway Clearance - PTBDocument2 pagesIneffective Airway Clearance - PTBIrish Eunice FelixNo ratings yet
- Ineffective Breathing PatternDocument185 pagesIneffective Breathing PatternSusi LambiyantiNo ratings yet
- Risk For Impaired SwallowingDocument3 pagesRisk For Impaired SwallowingCalimlim Kim100% (1)
- Nursing Care Plan For AIDS HIVDocument3 pagesNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- Nursing Diagnosis: Impaired Gas ExchangeDocument4 pagesNursing Diagnosis: Impaired Gas ExchangeShen Paril0% (1)
- Activity IntoleranceDocument2 pagesActivity Intolerancejunex123No ratings yet
- Nursing Care PlanDocument14 pagesNursing Care PlanVin Landicho100% (1)
- Student Nurses' Community: Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesStudent Nurses' Community: Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale Evaluationgreyciee은No ratings yet
- Risk For Aspiration: Risk For Aspiration: at Risk For Entry of Gastrointestinal Secretions, Oropharyngeal SecretionDocument6 pagesRisk For Aspiration: Risk For Aspiration: at Risk For Entry of Gastrointestinal Secretions, Oropharyngeal SecretionAngie MandeoyaNo ratings yet
- Nursing Care Plan: Risk For Disuse SyndromeDocument2 pagesNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurNo ratings yet
- Activity IntoleranceDocument2 pagesActivity Intoleranceayra_alegreNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document1 pageChronic Obstructive Pulmonary Disease (COPD)Bheru LalNo ratings yet
- NCPDocument4 pagesNCPMark Benedict Ocampo VelardeNo ratings yet
- NCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsDocument3 pagesNCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsSarah Ann Jamilla FaciolanNo ratings yet
- NCP (BODY WEAKNESS)Document3 pagesNCP (BODY WEAKNESS)Jum ChumNo ratings yet
- NCP Inffective Tissue PerfusionDocument3 pagesNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- NCP BMDocument1 pageNCP BMSourabh MehraNo ratings yet
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- NCPDocument10 pagesNCPMack Jhed AnarconNo ratings yet
- Nursing Care Plan 7 Knowledge DeficitDocument8 pagesNursing Care Plan 7 Knowledge Deficitdbryant0101100% (8)
- Ineffective Airway ClearanceDocument2 pagesIneffective Airway Clearancejancel_bollaNo ratings yet
- 1 Ineffective Breathing PatternDocument8 pages1 Ineffective Breathing PatternNoel MontemayorNo ratings yet
- Nursing Care Plan 2Document6 pagesNursing Care Plan 2KM TopacioNo ratings yet
- Medical Diagnosis: Bronchial Asthma Impaired Gas ExchangeDocument2 pagesMedical Diagnosis: Bronchial Asthma Impaired Gas ExchangeAndrea Chua BuadoNo ratings yet
- NCP - Ineffective Airway ClearanceDocument4 pagesNCP - Ineffective Airway ClearanceKim Gabrielle Exene LeeNo ratings yet
- Ncp-Impaired Gas ExchangeDocument2 pagesNcp-Impaired Gas ExchangeSJ Abunda0% (1)
- Ineffective Airway Clearance-Nursing Care Plan For COPDDocument2 pagesIneffective Airway Clearance-Nursing Care Plan For COPDRnspeakcom100% (1)
- Concept Map PEDocument3 pagesConcept Map PERobert MariasiNo ratings yet
- University of Northern PhilippinesDocument1 pageUniversity of Northern PhilippinesCezanne CruzNo ratings yet
- NCPDocument7 pagesNCPMarius Clifford BilledoNo ratings yet
- Gi-Rle - NCP For Deficient Fluid VolumeDocument2 pagesGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- NCP - Pulmonary TuberculosisDocument6 pagesNCP - Pulmonary TuberculosisastrijuNo ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- Nursing Care Plan: Name: DRT Age: 67 Diagnosis: Cva 2° To HPNDocument3 pagesNursing Care Plan: Name: DRT Age: 67 Diagnosis: Cva 2° To HPNKristina Marie Parulan RnNo ratings yet
- Septic ShockDocument1 pageSeptic ShockShaine Wolfe100% (1)
- Immobility Care Plan For NursesDocument3 pagesImmobility Care Plan For NursesColleen Murray67% (9)
- NCP For BreathingDocument17 pagesNCP For BreathingCeleste Sin Yee100% (1)
- Chapter 47 Diabetes Mellitus PDFDocument14 pagesChapter 47 Diabetes Mellitus PDFRLLT100% (1)
- Impaired Breathing PatternDocument1 pageImpaired Breathing PatternHanya Bint PotawanNo ratings yet
- Drug StudyDocument20 pagesDrug StudydjanindNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanSharmaine Grace Florig100% (2)
- Nursing Care Plan Risk For InjuryDocument1 pageNursing Care Plan Risk For InjuryAce Dioso TubascoNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanElijah S GomezNo ratings yet
- NCP Intra FinalDocument7 pagesNCP Intra FinalRoxanne Ganayo ClaverNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Choanal AtresiaDocument9 pagesNursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Choanal AtresiaJinaan MahmudNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Bronchopulmonary DisplasiaDocument9 pagesNursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Bronchopulmonary DisplasiaJinaan MahmudNo ratings yet
- NCM 101 Skills Finals: Care of Mother, Child and FamilyDocument38 pagesNCM 101 Skills Finals: Care of Mother, Child and FamilycheenapberberNo ratings yet
- Intranatal Table and InferenceDocument3 pagesIntranatal Table and InferencecheenapberberNo ratings yet
- Prehypertension: Average (And Ranges) Average (And Ranges)Document3 pagesPrehypertension: Average (And Ranges) Average (And Ranges)cheenapberberNo ratings yet
- Maternity Nursing!Document138 pagesMaternity Nursing!cheenapberber100% (2)
- CPDProgram Nurse 111919Document982 pagesCPDProgram Nurse 111919alchemist-at-lawNo ratings yet
- Management Trends, Issues and Problems: PresentersDocument26 pagesManagement Trends, Issues and Problems: PresenterscheenapberberNo ratings yet
- Hand Hygiene Why How and When BrochureDocument7 pagesHand Hygiene Why How and When BrochureLeis FatwaNo ratings yet
- Gerontological NursingDocument422 pagesGerontological Nursingcheenapberber100% (1)
- Commonly Used Medical AbbreviationsDocument3 pagesCommonly Used Medical AbbreviationscheenapberberNo ratings yet
- Theories of AgingDocument9 pagesTheories of AgingcheenapberberNo ratings yet
- Gastrointestinal Diseases1Document17 pagesGastrointestinal Diseases1cheenapberberNo ratings yet
- Diseases Transmitted Through Food and WaterDocument2 pagesDiseases Transmitted Through Food and WatercheenapberberNo ratings yet
- 004 LabsDiagnosticsManualDocument64 pages004 LabsDiagnosticsManualRaju Niraula100% (1)
- Heart Anatomy & ECG InterpretationDocument3 pagesHeart Anatomy & ECG InterpretationcheenapberberNo ratings yet
- Diabetes Mellitus Prepared By: LORI R. LARA, R.NDocument14 pagesDiabetes Mellitus Prepared By: LORI R. LARA, R.NNovie Carla0% (1)
- Geriatric Care: Presented by DR Nikhil Bansal J.N.M.C.,WardhaDocument99 pagesGeriatric Care: Presented by DR Nikhil Bansal J.N.M.C.,WardhacheenapberberNo ratings yet
- F & E Imbalance 2Document41 pagesF & E Imbalance 2cheenapberberNo ratings yet
- First AidDocument126 pagesFirst AidVishwanath SinduvadiNo ratings yet
- Hand Hygiene Why How and When BrochureDocument7 pagesHand Hygiene Why How and When BrochureLeis FatwaNo ratings yet
- Fundamentals Notetaking1Document5 pagesFundamentals Notetaking1cheenapberberNo ratings yet
- PH Red Cross First Aid and BLSDocument71 pagesPH Red Cross First Aid and BLSctuagent74% (19)
- CA1 '2 of 2' Funda 2019-2020Document164 pagesCA1 '2 of 2' Funda 2019-2020cheenapberberNo ratings yet
- General Considerations Prior To ActionDocument2 pagesGeneral Considerations Prior To ActioncheenapberberNo ratings yet
- Geria 2Document101 pagesGeria 2cheenapberberNo ratings yet
- Theories of AgingDocument9 pagesTheories of AgingcheenapberberNo ratings yet
- Geria 1Document56 pagesGeria 1cheenapberberNo ratings yet
- CMO 15 S 2017 PDFDocument63 pagesCMO 15 S 2017 PDFJamal P. AlawiyaNo ratings yet
- The correct answer is a. A urine specimen obtained through catheterization is a random urine specimenDocument55 pagesThe correct answer is a. A urine specimen obtained through catheterization is a random urine specimencheenapberberNo ratings yet
- Heart FailureDocument1 pageHeart FailurecheenapberberNo ratings yet
- Full Download Test Bank For Goulds Pathophysiology For The Health Professions 5th Edition by Vanmeter PDF Full ChapterDocument35 pagesFull Download Test Bank For Goulds Pathophysiology For The Health Professions 5th Edition by Vanmeter PDF Full Chapteramurcousomentumnsk1100% (15)
- Disorders of The Digestive SystemDocument3 pagesDisorders of The Digestive SystemɪQ ʟᴇᴠᴇʟ 148ˊˎ-No ratings yet
- Pathology in Clinical Practice 50 Case Studies - 2009Document224 pagesPathology in Clinical Practice 50 Case Studies - 2009Omar SarvelNo ratings yet
- The Mangled Extremity Score and Amputation Time FoDocument17 pagesThe Mangled Extremity Score and Amputation Time FoTrisendi YogaNo ratings yet
- Case Alcohol Abuse and Unusual Abdominal Pain in A 49-Year-OldDocument7 pagesCase Alcohol Abuse and Unusual Abdominal Pain in A 49-Year-OldPutri AmeliaNo ratings yet
- C+F-Intracranial Pressure in Dogs and CatsDocument13 pagesC+F-Intracranial Pressure in Dogs and Catstaner_soysuren100% (2)
- Transient Ischemic AttacksDocument10 pagesTransient Ischemic AttacksfabianounifenasNo ratings yet
- Pharm Stroke: Care PadaDocument38 pagesPharm Stroke: Care PadaDimas RfNo ratings yet
- Isman Firdaus, DR, SP - JP (K), FIHA: QualificationDocument38 pagesIsman Firdaus, DR, SP - JP (K), FIHA: QualificationGhinna Septhiana PratiwiNo ratings yet
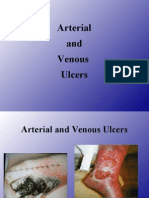
- 4 - Arterial & Venous UlcersDocument86 pages4 - Arterial & Venous Ulcerscharity kalinowsky100% (13)
- Causes of Atrial Fibrillation: PIRATESDocument4 pagesCauses of Atrial Fibrillation: PIRATESbibbiNo ratings yet
- Acute Coronary Syndrome Update: Charles Shoalmire, MSN, RN, ACNP-BCDocument31 pagesAcute Coronary Syndrome Update: Charles Shoalmire, MSN, RN, ACNP-BCDwi Akbarina YahyaNo ratings yet
- 1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeDocument15 pages1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeElvaNo ratings yet
- Coronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdDocument99 pagesCoronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdMwanja MosesNo ratings yet
- Wa0013.Document102 pagesWa0013.Cynthia GNo ratings yet
- Cell Injury Patho LabDocument17 pagesCell Injury Patho LabRUTUJA DILIP GADENo ratings yet
- Livanova - Bi-Flow CannulaDocument3 pagesLivanova - Bi-Flow CannulaAhmadNo ratings yet
- Acute Renal FailureDocument30 pagesAcute Renal FailureCarmina SalvañaNo ratings yet
- Innovations in Cardiovascular Disease ManagementDocument183 pagesInnovations in Cardiovascular Disease ManagementGopal Kumar DasNo ratings yet
- Coronary Artery DiseaseDocument13 pagesCoronary Artery DiseaseChristianHanjokarNo ratings yet
- NS3 Ncp-FdarDocument5 pagesNS3 Ncp-FdarArdiene Shallouvette GamosoNo ratings yet
- Vascular Diseases: Idar Mappangara Department of Cardiology Hasanuddin UniversityDocument31 pagesVascular Diseases: Idar Mappangara Department of Cardiology Hasanuddin UniversityriniNo ratings yet
- Cerebrovascular AccidentDocument15 pagesCerebrovascular AccidentBeeshma BirjasinghNo ratings yet
- Coronary Artery DiseaseDocument10 pagesCoronary Artery DiseaseStephanie ValerioNo ratings yet
- Csbpr7 Acute Stroke Management Module Final Eng 2022Document161 pagesCsbpr7 Acute Stroke Management Module Final Eng 2022Vigneshwara NagarajanNo ratings yet
- Noninvasive Ventilation in Acute Respiratory Failure in AdultsDocument12 pagesNoninvasive Ventilation in Acute Respiratory Failure in AdultsferrevNo ratings yet
- Unstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowDocument27 pagesUnstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowCyntia KhairaniNo ratings yet
- Ischemic Heart Disease PWDocument13 pagesIschemic Heart Disease PWEunica RamosNo ratings yet
- HBOT and Stroke - TBIDocument24 pagesHBOT and Stroke - TBIStemCellMDNo ratings yet
- Step 2 CK Review - CardiologyDocument28 pagesStep 2 CK Review - Cardiologyrsmd1986100% (1)