You might also like
- Govt. College of Nursing, Bilaspur (C.G.) Case Study Evaluation FormatDocument2 pagesGovt. College of Nursing, Bilaspur (C.G.) Case Study Evaluation FormatDivya ToppoNo ratings yet
- Lesson Plan On Induction of LaborDocument16 pagesLesson Plan On Induction of LaborPriyanka YadavNo ratings yet
- Clinical Evaluation Format BSC JIMSHDocument3 pagesClinical Evaluation Format BSC JIMSHKiran Mini RaviNo ratings yet
- Obg MSC 1st YearDocument10 pagesObg MSC 1st Yearniharika mishraNo ratings yet
- All India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicDocument12 pagesAll India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicFarheen khanNo ratings yet
- Lesson Plan of Fetal MeasureDocument5 pagesLesson Plan of Fetal Measuresuman guptaNo ratings yet
- Specific Teaching Objectives Contents Hr Resourse learning activities aids evaluation personDocument14 pagesSpecific Teaching Objectives Contents Hr Resourse learning activities aids evaluation personsandeepv08100% (1)
- Teacher-Led AV-Aided Lesson on Amniotic FluidDocument9 pagesTeacher-Led AV-Aided Lesson on Amniotic Fluidkrupapallavi nadimikeriNo ratings yet
- Obg Course PlanDocument4 pagesObg Course PlanDelphy VargheseNo ratings yet
- College Nursing Tips Master Rotation PlanDocument4 pagesCollege Nursing Tips Master Rotation PlanBisakha DeyNo ratings yet
- Lesson Plan On Genetic CounsellngDocument17 pagesLesson Plan On Genetic Counsellngrenu0% (1)
- Fourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric NursingDocument35 pagesFourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric Nursingsandeepv080% (1)
- Lesson Plan On Staffing FINALDocument7 pagesLesson Plan On Staffing FINALparushni dabNo ratings yet
- M.O.S.C College Psychiatric Nursing FormsDocument5 pagesM.O.S.C College Psychiatric Nursing FormsprashanthNo ratings yet
- Curriculum Research in Nursing-Lesson PlanDocument13 pagesCurriculum Research in Nursing-Lesson Planavinash dhameriyaNo ratings yet
- BSC 4 MidwiferyDocument14 pagesBSC 4 MidwiferySwarnima RobinsonNo ratings yet
- M.SC Nursing Master PlanDocument1 pageM.SC Nursing Master PlanShaikh SalimNo ratings yet
- PBBSc Nursing 1st Year Rotation Plan 2020-21Document1 pagePBBSc Nursing 1st Year Rotation Plan 2020-21Delphy VargheseNo ratings yet
- Kgmu College of Nursing Lesson Plan: Role of National, International and Voluntary Organization in Family PlanningDocument19 pagesKgmu College of Nursing Lesson Plan: Role of National, International and Voluntary Organization in Family PlanningNeha SinghNo ratings yet
- Lakshmi Micro TeachingDocument20 pagesLakshmi Micro Teachingduddela lakshmi100% (1)
- Micro Teaching MTP.00Document8 pagesMicro Teaching MTP.00Daily DoseNo ratings yet
- All India Institute of Medical Sciences, Jodhpur College of NursingDocument17 pagesAll India Institute of Medical Sciences, Jodhpur College of NursingFarheen khanNo ratings yet
- Lesson Plan On Postnatal AssessmentDocument11 pagesLesson Plan On Postnatal AssessmentMadhavi ModaNo ratings yet
- Lesson Plan ANPDocument24 pagesLesson Plan ANPKaruna NidhiNo ratings yet
- Handouts OBSTETRICS EMERGENCYDocument9 pagesHandouts OBSTETRICS EMERGENCYAshish GuptaNo ratings yet
- L P APHDocument11 pagesL P APHmoni khatkarNo ratings yet
- Antenatal Examination DemonstrationDocument10 pagesAntenatal Examination DemonstrationSamarpit Singh0% (1)
- Maruti Institute of Nursing, Itarsi: Maternal Nursing Child Health Nursing Medical Surgical Nursing Nursing FoundationDocument4 pagesMaruti Institute of Nursing, Itarsi: Maternal Nursing Child Health Nursing Medical Surgical Nursing Nursing FoundationHarshaNo ratings yet
- Pal College of Nursing & Medical Science, Haldwani: Fetal CirculationDocument10 pagesPal College of Nursing & Medical Science, Haldwani: Fetal CirculationpriyankaNo ratings yet
- Midwifery and Obstetric NursingDocument9 pagesMidwifery and Obstetric NursingANUM NOORINo ratings yet
- LESSON PLAN - AnagicisDocument22 pagesLESSON PLAN - AnagicisrenuNo ratings yet
- L T College of Nursing SNDT University Churchgate Lesson Plan On Nursing Care of A Patient With Menstrual DisordersDocument13 pagesL T College of Nursing SNDT University Churchgate Lesson Plan On Nursing Care of A Patient With Menstrual DisordersPriyanka NilewarNo ratings yet
- Unit Plan B.Sc. (Nursing) I Year Nutrition (Proteins)Document5 pagesUnit Plan B.Sc. (Nursing) I Year Nutrition (Proteins)Abhilasha Solomon100% (1)
- Examine Placenta Clinical LessonDocument6 pagesExamine Placenta Clinical LessonMiriward Zimba100% (1)
- Examination of Placenta for AbnormalitiesDocument3 pagesExamination of Placenta for AbnormalitiesPriyanka SheoranNo ratings yet
- Gracious College Nursing Master Rotation Plan 2019-20Document6 pagesGracious College Nursing Master Rotation Plan 2019-20Topeshwar TpkNo ratings yet
- Class Teaching ON Infertility: Perfoma For The Lesson PlanDocument32 pagesClass Teaching ON Infertility: Perfoma For The Lesson PlanAGERI PUSHPALATHA100% (1)
- Revised Proforma Guidelines Internal Assessment II PBBSC 011007Document58 pagesRevised Proforma Guidelines Internal Assessment II PBBSC 011007mljg30100% (2)
- Postnatal Exam: JIET Nursing Lesson on Postpartum AssessmentDocument11 pagesPostnatal Exam: JIET Nursing Lesson on Postpartum AssessmentDrPreeti Thakur ChouhanNo ratings yet
- b.sc.4th Yr Master RotationDocument2 pagesb.sc.4th Yr Master RotationHONEYNo ratings yet
- Lesson Plan On Operative DeliveryDocument13 pagesLesson Plan On Operative DeliveryArjun NeupaneNo ratings yet
- Complications of Pregnancy: Placenta PreviaDocument4 pagesComplications of Pregnancy: Placenta PreviaChristyl CalizoNo ratings yet
- Bhopal (M.P.) : Unit PlanDocument4 pagesBhopal (M.P.) : Unit PlanamitNo ratings yet
- Lesson Plan On Antenatal EXERCISESDocument43 pagesLesson Plan On Antenatal EXERCISESswatiNo ratings yet
- Explaining the Elaborate Development of the PlacentaDocument13 pagesExplaining the Elaborate Development of the PlacentaSudesh TomarNo ratings yet
- Biochemical Methods ObgDocument25 pagesBiochemical Methods ObgRupali AroraNo ratings yet
- B.Sc. Nursing rotation planDocument26 pagesB.Sc. Nursing rotation planpriyankaNo ratings yet
- HT On Hyperemesis GravidumDocument15 pagesHT On Hyperemesis GravidumPriyaNo ratings yet
- lESSONPLAN FOR RETURN DEMODocument6 pageslESSONPLAN FOR RETURN DEMOJay PaulNo ratings yet
- Topic Lesson Plan On Course Plan, Master Plan, Unit PlanDocument29 pagesTopic Lesson Plan On Course Plan, Master Plan, Unit PlanAnas khan0% (1)
- Leukemia Lesson PlanDocument5 pagesLeukemia Lesson PlanTopeshwar TpkNo ratings yet
- Course Plan: Obstetric & Gynaecological NursingDocument11 pagesCourse Plan: Obstetric & Gynaecological NursingPriya100% (3)
- Lesson Plan OBGYDocument12 pagesLesson Plan OBGYKirti kittuNo ratings yet
- Health Talk On ContraceptionDocument32 pagesHealth Talk On Contraceptionvaishali TMU studentNo ratings yet
- Front Cover of OBG FileDocument5 pagesFront Cover of OBG FilepriyankaNo ratings yet
- Full Lesson Plan On BSEDocument4 pagesFull Lesson Plan On BSEJyoti SamraNo ratings yet
- Unit Plan Obg Sem 6 Unit IVDocument6 pagesUnit Plan Obg Sem 6 Unit IVDelphy VargheseNo ratings yet
- Gynecological ThesisDocument117 pagesGynecological ThesisSUPRIYA SINGHNo ratings yet
- Maharashtra State Board Nursing FormsDocument26 pagesMaharashtra State Board Nursing FormsSwarnima Robinson100% (1)
- Proforma & Guideline For Case Presentation/Case StudyDocument9 pagesProforma & Guideline For Case Presentation/Case StudySwaraNo ratings yet
- Clinical Leadership As An Integral Curriculum Thread in Pre-RegisDocument18 pagesClinical Leadership As An Integral Curriculum Thread in Pre-RegisNeha SinghNo ratings yet
- Antenatal Care ProcedureDocument18 pagesAntenatal Care ProcedureNeha SinghNo ratings yet
- Combination of Pelvic Floor and Abdominal Muscle eDocument5 pagesCombination of Pelvic Floor and Abdominal Muscle eNeha SinghNo ratings yet
- Mgso 4Document1 pageMgso 4Neha SinghNo ratings yet
- Male Kegel ExDocument4 pagesMale Kegel Exkabshiel100% (1)
- Drug Presentation On Magnesium SulfateDocument1 pageDrug Presentation On Magnesium SulfateNeha SinghNo ratings yet
- Anorexia Nervosa and The KidneyDocument36 pagesAnorexia Nervosa and The Kidneywobblegobble100% (1)
- Sample Lesson Plan FormatDocument5 pagesSample Lesson Plan FormatNeha SinghNo ratings yet
- Birth Injuries 170507205454Document60 pagesBirth Injuries 170507205454Vyshak KrishnanNo ratings yet
- Personality TypeDocument23 pagesPersonality TypeBadidz Ong SucoNo ratings yet
- Types of ReliabilityDocument39 pagesTypes of ReliabilityAydila SaputriNo ratings yet
- Magnesium Sulfa-WPS OfficeDocument21 pagesMagnesium Sulfa-WPS OfficeNeha SinghNo ratings yet
- Assignment On Art Ethical and Legal IssuessDocument11 pagesAssignment On Art Ethical and Legal IssuessNeha SinghNo ratings yet
- Kgmu College of Nursing Lesson Plan: Role of National, International and Voluntary Organization in Family PlanningDocument19 pagesKgmu College of Nursing Lesson Plan: Role of National, International and Voluntary Organization in Family PlanningNeha SinghNo ratings yet
- Summated Scale: By-Neha Singh M.Sc. (N) 1 YearDocument16 pagesSummated Scale: By-Neha Singh M.Sc. (N) 1 YearNeha Singh75% (4)
- Planning and Organizing Ancillary Services: By-Ms. Farah NaazDocument46 pagesPlanning and Organizing Ancillary Services: By-Ms. Farah NaazNeha SinghNo ratings yet
- Kgmu College of Nursing Lesson Plan: Role of National, International and Voluntary Organization in Family PlanningDocument19 pagesKgmu College of Nursing Lesson Plan: Role of National, International and Voluntary Organization in Family PlanningNeha SinghNo ratings yet
- Personality TypeDocument23 pagesPersonality TypeBadidz Ong SucoNo ratings yet
- Decision Making: Presented by Rupali SinghDocument36 pagesDecision Making: Presented by Rupali SinghNeha SinghNo ratings yet
- Oxygen InsufficiencyDocument27 pagesOxygen InsufficiencyNeha SinghNo ratings yet
- Planning and Organizing Ancillary Services: By-Ms. Farah NaazDocument46 pagesPlanning and Organizing Ancillary Services: By-Ms. Farah NaazNeha SinghNo ratings yet
- Trends in Nursing EducationDocument6 pagesTrends in Nursing EducationNeha SinghNo ratings yet
- Assignment On Art Ethical and Legal IssuessDocument11 pagesAssignment On Art Ethical and Legal IssuessNeha SinghNo ratings yet
- Summated Scale: By-Neha Singh M.Sc. (N) 1 YearDocument16 pagesSummated Scale: By-Neha Singh M.Sc. (N) 1 YearNeha Singh75% (4)
- AACE-ACE - Practice Guidelines For Developing Diabete MellitusDocument87 pagesAACE-ACE - Practice Guidelines For Developing Diabete MellitusDottNo ratings yet
- Massage For PromotingDocument7 pagesMassage For PromotingcaipillanNo ratings yet
- Cefazolin Drug Study SummaryDocument4 pagesCefazolin Drug Study Summaryshadow gonzalezNo ratings yet
- Supervised Classification Techniques and Deep Learning For Mortality Prediction in Sepsis PatientsDocument6 pagesSupervised Classification Techniques and Deep Learning For Mortality Prediction in Sepsis PatientsFabian Alberto Jaimes BarraganNo ratings yet
- Historical Background of Murtala Muhammad Specialist Hospital KanoDocument10 pagesHistorical Background of Murtala Muhammad Specialist Hospital KanoLeenCo TechNo ratings yet
- Soper Resume-2Document2 pagesSoper Resume-2api-484953296No ratings yet
- Health Reporting: Winner - Bamuturaki Musinguzi, Daily MonitorDocument14 pagesHealth Reporting: Winner - Bamuturaki Musinguzi, Daily MonitorAfrican Centre for Media Excellence100% (1)
- EATMS - Discussion On Phlegm Damp WaterDocument4 pagesEATMS - Discussion On Phlegm Damp WaterfernabarbNo ratings yet
- Retinopathy of PrematurityDocument7 pagesRetinopathy of PrematurityDewi PermatasariNo ratings yet
- DDFGGDocument2 pagesDDFGGstrafforNo ratings yet
- Health VocabularyDocument13 pagesHealth VocabularyMaria RadaNo ratings yet
- Cupping/Hijama Times. 1 Issue: Section 3Document33 pagesCupping/Hijama Times. 1 Issue: Section 3Hala Elnouty78% (9)
- Notice: Grants and Cooperative Agreements Availability, Etc.: Women Living in Puerto Rico and U.S. Virgin Islands HIV Prevention ProgramDocument8 pagesNotice: Grants and Cooperative Agreements Availability, Etc.: Women Living in Puerto Rico and U.S. Virgin Islands HIV Prevention ProgramJustia.comNo ratings yet
- Bogash 1963Document5 pagesBogash 1963wahyu santikaNo ratings yet
- Cap 2019 04 01 PDFDocument58 pagesCap 2019 04 01 PDFRajeev PareekNo ratings yet
- Cautery To Little's Area: What Is Little's Area and Why Do I Need This Operation?Document4 pagesCautery To Little's Area: What Is Little's Area and Why Do I Need This Operation?Moustafa EzzatNo ratings yet
- Lumpy Skin DiseaseDocument99 pagesLumpy Skin DiseaseDaoud IssaNo ratings yet
- Panna Dhai Maa Subharti Nursing College, Meerut: Seminar On AbortionDocument31 pagesPanna Dhai Maa Subharti Nursing College, Meerut: Seminar On Abortionriya singhNo ratings yet
- CBDTRP Community Drug Rehab ProgramDocument15 pagesCBDTRP Community Drug Rehab ProgramErin SantosNo ratings yet
- Scrub and Circulating Practitioner Simulation Script - Salimbagat, UsmanDocument12 pagesScrub and Circulating Practitioner Simulation Script - Salimbagat, UsmanChristine Pialan SalimbagatNo ratings yet
- Gestational Diabetes Mellitus: Dr. R V S N Sarma., M.D., M.SC., (Canada)Document45 pagesGestational Diabetes Mellitus: Dr. R V S N Sarma., M.D., M.SC., (Canada)Yohannis AsefaNo ratings yet
- How China Is Fighting HIV/AIDS Stigma (Wang Longde)Document22 pagesHow China Is Fighting HIV/AIDS Stigma (Wang Longde)National Press FoundationNo ratings yet
- English-6-Q2-Module-1-Lesson-2-Palpallatoc - Lydia E. - FINALDocument15 pagesEnglish-6-Q2-Module-1-Lesson-2-Palpallatoc - Lydia E. - FINALDanielLarryAquinoNo ratings yet
- Health Promotion DiabetesDocument20 pagesHealth Promotion Diabetesharshotsai100% (1)
- AIIMS NORCET EXAM PATTERN - Watermark 1Document12 pagesAIIMS NORCET EXAM PATTERN - Watermark 1Poonam Yadav roll no.53No ratings yet
- Medical Laboratory in Abu DhabiDocument5 pagesMedical Laboratory in Abu DhabiPrime CureNo ratings yet
- Diabetes Self Management FinaleDocument76 pagesDiabetes Self Management FinaleAbdelaziz LazregNo ratings yet
- Checklist - Equipment - GPDocument1 pageChecklist - Equipment - GPMichael Phratama NugrahaNo ratings yet
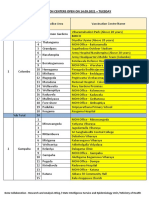
- Vaccination Centers On 14.09.2021Document8 pagesVaccination Centers On 14.09.2021Chanu On CTNo ratings yet
- Immediate Care of The NewbornDocument10 pagesImmediate Care of The NewbornRaffy100% (2)