You might also like
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- Lecture 1 - Development of Respiratory SystemDocument27 pagesLecture 1 - Development of Respiratory SystemRachmad MusyaffaNo ratings yet
- Pulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungFrom EverandPulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungNo ratings yet
- Lung Growth and Development: Suchita Joshi, Sailesh KotechaDocument6 pagesLung Growth and Development: Suchita Joshi, Sailesh KotechaAditya SanjayaNo ratings yet
- Development of Respiratory System: Dr. Saeed Vohra & Dr. Sanaa AlshaarawyDocument26 pagesDevelopment of Respiratory System: Dr. Saeed Vohra & Dr. Sanaa AlshaarawyChristineNo ratings yet
- 20 - Development of Respiratory SystemDocument33 pages20 - Development of Respiratory SystemDr.B.B.GosaiNo ratings yet
- 3-Embryology of Respiratory SystemDocument25 pages3-Embryology of Respiratory SystemNur HikmahNo ratings yet
- Pathophysiology of RDSDocument5 pagesPathophysiology of RDSsandyNo ratings yet
- Ultrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsDocument7 pagesUltrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsRafael JustinoNo ratings yet
- Embryo Exam 2: Respiratory System: Download The Android App!Document4 pagesEmbryo Exam 2: Respiratory System: Download The Android App!AzizNo ratings yet
- Development of Body Cavities and Diaphragm: Pleuro-Pericardial and Pleuro-Peritoneal MembraneDocument14 pagesDevelopment of Body Cavities and Diaphragm: Pleuro-Pericardial and Pleuro-Peritoneal MembraneÑäd ÉèmNo ratings yet
- Pediatric and Neonatal Respiratory Care DevelopmentDocument205 pagesPediatric and Neonatal Respiratory Care DevelopmentAlexander Santiago ParelNo ratings yet
- Vipin Sharma Embryogenesis of Respiratory SystemDocument31 pagesVipin Sharma Embryogenesis of Respiratory SystemRitvik SharmaNo ratings yet
- Lung Development and Anatomy ExplainedDocument91 pagesLung Development and Anatomy ExplainedPrarthanaNo ratings yet
- All About RespiratoryDocument69 pagesAll About RespiratoryMarcellina Awing100% (1)
- Neonatal Respiratory Care: Moderated By: Shyam Krishnan Presented By: A Sampath KumarDocument62 pagesNeonatal Respiratory Care: Moderated By: Shyam Krishnan Presented By: A Sampath KumarPrethy PhilipNo ratings yet
- 1 (Lung Development)Document12 pages1 (Lung Development)Dr.sonuNo ratings yet
- Embryo Development Lungs+Body CavityDocument8 pagesEmbryo Development Lungs+Body CavityKingNo ratings yet
- Human Lung DevelopmentDocument20 pagesHuman Lung DevelopmentMila KarmilaNo ratings yet
- M.03 Respiratory Disorders of Children Part 1 (Dr. Tandoc) (10-26-20)Document7 pagesM.03 Respiratory Disorders of Children Part 1 (Dr. Tandoc) (10-26-20)VanessaNo ratings yet
- Pedia Pulmo 1Document129 pagesPedia Pulmo 1Sven OrdanzaNo ratings yet
- Pedia Pulmo 1Document129 pagesPedia Pulmo 1Sven OrdanzaNo ratings yet
- Introduction To Physiological Changes in NEONATAL AND PEDIATRIC RESPICARE James Astrologo LamusaoDocument88 pagesIntroduction To Physiological Changes in NEONATAL AND PEDIATRIC RESPICARE James Astrologo LamusaoDanao, Aira A.No ratings yet
- ExamView - Chapter - 0124Document2 pagesExamView - Chapter - 0124Devin MckayNo ratings yet
- Respiratory, USMLE ENDPOINT BY DR AHMED SHEBLDocument91 pagesRespiratory, USMLE ENDPOINT BY DR AHMED SHEBLDaNy Chiriac100% (3)
- Neonatal Pulmonary PhysiologyDocument6 pagesNeonatal Pulmonary PhysiologyAnapaolaNo ratings yet
- ExamView - Chapter - 01Document2 pagesExamView - Chapter - 01Devin MckayNo ratings yet
- Embryology of Respiratory System NotesDocument3 pagesEmbryology of Respiratory System NotesJulienne Sanchez-SalazarNo ratings yet
- Respiratory Distress in The NewbornDocument146 pagesRespiratory Distress in The NewbornAmit RamrattanNo ratings yet
- Development of the Respiratory System and Its AnomaliesDocument17 pagesDevelopment of the Respiratory System and Its AnomaliesmichaelqurtisNo ratings yet
- Embryologi OF The Respiratory System: Arti Rosaria Dewi, DRDocument60 pagesEmbryologi OF The Respiratory System: Arti Rosaria Dewi, DRAsti NuriatiNo ratings yet
- Pulmonary EmbolismDocument21 pagesPulmonary EmbolismMadhu Bala100% (2)
- Embryology of Lower Respiratory TractDocument34 pagesEmbryology of Lower Respiratory TractMeryka Dwi Pramitha Sari100% (1)
- Neonatal Respiratory Distress SyndromeDocument5 pagesNeonatal Respiratory Distress SyndromeMaliha Zaman KhanNo ratings yet
- Development of Respiratory SystemDocument34 pagesDevelopment of Respiratory SystemNatalie HuiNo ratings yet
- Development of Respiratory SystemDocument23 pagesDevelopment of Respiratory SystemRas Siko SafoNo ratings yet
- Neonatal Respiration PhysiologyDocument6 pagesNeonatal Respiration PhysiologyRaja Ahmad Rusdan MusyawirNo ratings yet
- Corticosteroid in Lung MaturationDocument12 pagesCorticosteroid in Lung Maturationtommy japolaNo ratings yet
- RespiratorDocument97 pagesRespiratorandreaNo ratings yet
- Learning Aims WWW - Embryology.ch/indexen - HTML: at The End of This Module You Should Be Able ToDocument13 pagesLearning Aims WWW - Embryology.ch/indexen - HTML: at The End of This Module You Should Be Able ToMuhammad Luqman HakimNo ratings yet
- Developmental Biology of The Pulmonary Circulation: Alison HislopDocument10 pagesDevelopmental Biology of The Pulmonary Circulation: Alison HislopMarcela RodriguezNo ratings yet
- Anak 1Document72 pagesAnak 1Nency PurmayaNo ratings yet
- The Respiratory System: Supplement To Text, Chapter 9Document77 pagesThe Respiratory System: Supplement To Text, Chapter 9Christina GonezNo ratings yet
- 2006 Clearance of Fluid From LungsDocument7 pages2006 Clearance of Fluid From LungsyaritzaalviarezNo ratings yet
- Respiratory System EmbDocument29 pagesRespiratory System EmbDanish GujjarNo ratings yet
- Case 3 - Anatomy and Physiology - SalimbagatDocument4 pagesCase 3 - Anatomy and Physiology - SalimbagatChristine Pialan SalimbagatNo ratings yet
- Bronchioles Then Divide Into Three TypesDocument3 pagesBronchioles Then Divide Into Three TypesJeremy EvansNo ratings yet
- Illness in The NewbornDocument34 pagesIllness in The NewbornVivian Jean TapayaNo ratings yet
- Fetal Development Stages & Fertilization ExplainedDocument136 pagesFetal Development Stages & Fertilization ExplainedJade Louise FkshmNo ratings yet
- Development of The Respiratory System: Section of Embryology Department of AnatomyDocument41 pagesDevelopment of The Respiratory System: Section of Embryology Department of AnatomyChristian Pato SidabutarNo ratings yet
- RESPIDocument30 pagesRESPIARVIND KUMAR YADAVNo ratings yet
- Embryology Notes emDocument32 pagesEmbryology Notes emSavita HanamsagarNo ratings yet
- Development of The Respiratory SystemDocument8 pagesDevelopment of The Respiratory SystemDanielNo ratings yet
- Respiratory Distress Syndrome (RDS) GuideDocument18 pagesRespiratory Distress Syndrome (RDS) GuideMaricel DefiestaNo ratings yet
- Embryology of Salivary GlandsDocument21 pagesEmbryology of Salivary GlandsAssist Professor Dr-Bayad Jaza Mahmud100% (3)
- Embryology Notes emDocument18 pagesEmbryology Notes emLuqman AfifNo ratings yet
- Respiratory Disorders & TB in Children (Part I and Ii) - Dr. MendozaDocument17 pagesRespiratory Disorders & TB in Children (Part I and Ii) - Dr. MendozaRea Dominique CabanillaNo ratings yet
- Congenital Anomalies of Airway and Lung ParenchymaDocument71 pagesCongenital Anomalies of Airway and Lung ParenchymaGopal ChawlaNo ratings yet
- Respiratory SystemDocument2 pagesRespiratory SystemDearly Niña OsinsaoNo ratings yet
- Textbook Discussion On Acute Community-Acquired Pneumonia (BSN 3A-Group 6)Document9 pagesTextbook Discussion On Acute Community-Acquired Pneumonia (BSN 3A-Group 6)Jica Marie Bandiola GicaroNo ratings yet
- Dr. Taubel's STD Lecture, Part 1Document61 pagesDr. Taubel's STD Lecture, Part 1f3er3No ratings yet
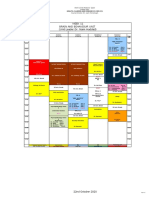
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 pageWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3No ratings yet
- Associate Professor of Medical Ethics (Education) Department of MedicineDocument6 pagesAssociate Professor of Medical Ethics (Education) Department of Medicinef3er3No ratings yet
- Psychiatry Case LogDocument6 pagesPsychiatry Case Logf3er3No ratings yet
- Dr. Taubel's STD Lecture, Part 2Document67 pagesDr. Taubel's STD Lecture, Part 2f3er3No ratings yet
- Aquifer Pediatrics Learning Objectives: Case 1Document10 pagesAquifer Pediatrics Learning Objectives: Case 1f3er3No ratings yet
- Psychiatry Case LogDocument6 pagesPsychiatry Case Logf3er3No ratings yet
- Dr. Sole's STD LectureDocument76 pagesDr. Sole's STD Lecturef3er3No ratings yet
- Discussion Questions - May 12, 2016Document7 pagesDiscussion Questions - May 12, 2016f3er3No ratings yet
- Psychiatry Case LogDocument6 pagesPsychiatry Case Logf3er3No ratings yet
- 12 Eating Disorders - mp4Document5 pages12 Eating Disorders - mp4f3er3No ratings yet
- AP Physics - Thermodynamics in 40 CharactersDocument7 pagesAP Physics - Thermodynamics in 40 Charactersf3er3No ratings yet
- BME 303 - Long and Short Term Weight RegulationDocument16 pagesBME 303 - Long and Short Term Weight Regulationf3er3No ratings yet
- Psychiatry Case LogDocument6 pagesPsychiatry Case Logf3er3No ratings yet
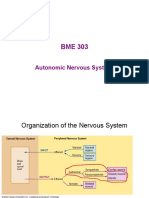
- BME 303 Autonomic Nervous System OrganizationDocument12 pagesBME 303 Autonomic Nervous System Organizationf3er3No ratings yet
- GI Physiology - Pancreatic, Liver, and Intestinal FunctionsDocument24 pagesGI Physiology - Pancreatic, Liver, and Intestinal Functionsf3er3No ratings yet
- BME 303-16-L7a EnergeticsiDocument35 pagesBME 303-16-L7a Energeticsif3er3No ratings yet
- Physics AP B Review Packet2012-2013Document26 pagesPhysics AP B Review Packet2012-2013netsam_flixsamNo ratings yet
- One Flew Over the Cuckoo's Nest QuizDocument3 pagesOne Flew Over the Cuckoo's Nest Quizf3er3No ratings yet
- One Flew Over The Cuckoo's Quiz #3Document3 pagesOne Flew Over The Cuckoo's Quiz #3f3er3No ratings yet
- HIDII Global Epdemic Precautions 2020-Dr MamtaniDocument21 pagesHIDII Global Epdemic Precautions 2020-Dr Mamtanif3er3No ratings yet
- Hong BAB JC5-Student Guide9.11.20finalDocument3 pagesHong BAB JC5-Student Guide9.11.20finalf3er3No ratings yet
- One Flew Over The Cuckoo's Quiz #2Document3 pagesOne Flew Over The Cuckoo's Quiz #2f3er3No ratings yet
- One Flew Over The Cuckoo's Quiz #4Document4 pagesOne Flew Over The Cuckoo's Quiz #4f3er3No ratings yet
- Thermodynamics Summer Assignment NMSIDocument14 pagesThermodynamics Summer Assignment NMSIf3er3No ratings yet
- HIDII Global Epdemic Precautions - SARS-CoV2-COVID - 2020 - DR CheemaDocument45 pagesHIDII Global Epdemic Precautions - SARS-CoV2-COVID - 2020 - DR Cheemaf3er3No ratings yet
- 10 - Stem Cell Transplants and Cellular TherapiesDocument71 pages10 - Stem Cell Transplants and Cellular Therapiesf3er3No ratings yet
- 10 - Respiratory System Under StressDocument53 pages10 - Respiratory System Under Stressf3er3No ratings yet
- Hormones and Renal System Review SummaryDocument2 pagesHormones and Renal System Review Summaryf3er3No ratings yet
- NYC's multifaceted approach to outbreak detectionDocument31 pagesNYC's multifaceted approach to outbreak detectionf3er3No ratings yet
- Exploring Marma TherapyDocument17 pagesExploring Marma TherapyIrina MartelNo ratings yet
- Multiple Choice Questions: A. B. C. DDocument27 pagesMultiple Choice Questions: A. B. C. DwanderagroNo ratings yet
- Meat Science 2Document10 pagesMeat Science 2nyxchura100% (1)
- USAFRICOM IDESPW Info Paper 20191009Document2 pagesUSAFRICOM IDESPW Info Paper 20191009Genry MercadoNo ratings yet
- Snoring Is Not Only Disturbance It Indicates To Care HealthDocument13 pagesSnoring Is Not Only Disturbance It Indicates To Care HealthRithika RamNo ratings yet
- Gyne - Benign LesionsDocument4 pagesGyne - Benign LesionsIsabel CastilloNo ratings yet
- HSHM 223/Hist 126 Doctors and Patients in Western MedicineDocument7 pagesHSHM 223/Hist 126 Doctors and Patients in Western MedicineLalalalaPineapplesNo ratings yet
- Superior Science Academy 10th Test 2 BioDocument1 pageSuperior Science Academy 10th Test 2 BioNaeem AmjidNo ratings yet
- Chapter 4 - Technologies That Enable MobilityDocument48 pagesChapter 4 - Technologies That Enable Mobilitysara sallaqNo ratings yet
- Chapter 12 Section 3Document21 pagesChapter 12 Section 3api-240305777No ratings yet
- Halen Dinata Atmaja - 10511910000003 - Quiz NotetakingDocument8 pagesHalen Dinata Atmaja - 10511910000003 - Quiz NotetakingAndika Surya HadiwinataNo ratings yet
- Case Study ThrombocytopeniaDocument8 pagesCase Study ThrombocytopeniaAmina TariqNo ratings yet
- CS Blue Sheet Mnemonics - USMLE Step 2 CSDocument1 pageCS Blue Sheet Mnemonics - USMLE Step 2 CSRafael G. Garcia SanchezNo ratings yet
- Possible Interview Questions For NursesDocument32 pagesPossible Interview Questions For NursesElisabeta Ivan75% (4)
- ADDICTA T 2017 0051 4 KopyaDocument11 pagesADDICTA T 2017 0051 4 KopyaLily FakhreddineNo ratings yet
- Radioiodine TherapyDocument5 pagesRadioiodine Therapyaccime24No ratings yet
- Azithromycin, Cefixime, Paracetamol Drug StudyDocument4 pagesAzithromycin, Cefixime, Paracetamol Drug StudyAzizah VillaminNo ratings yet
- PhysioEx Exercise 11 Activity 3Document3 pagesPhysioEx Exercise 11 Activity 3MEGAN NICOLE PERNILLA HERNANDEZNo ratings yet
- Medical Malpractice CasesDocument5 pagesMedical Malpractice Casesankitjakhar35No ratings yet
- Ge 111: Understanding The SelfDocument33 pagesGe 111: Understanding The SelfJonnah QuindoNo ratings yet
- Catalogue AMS A4 BD PapDocument29 pagesCatalogue AMS A4 BD PapHienNo ratings yet
- Dissertation Topics For Psychiatric NursingDocument6 pagesDissertation Topics For Psychiatric NursingWriteMyPaperReviewsUK100% (1)
- Ucspshs q1 Mod4 HumanBioCulturalEvolutionDocument34 pagesUcspshs q1 Mod4 HumanBioCulturalEvolutionTosee istosee100% (1)
- 2022.01.07.22268919v1.full Omicron 7 EneroDocument31 pages2022.01.07.22268919v1.full Omicron 7 EneroNancy Grisell RamirezNo ratings yet
- Elbow AssessmentDocument39 pagesElbow AssessmentshizarahimNo ratings yet
- A Companion To Fish's PsychopathologyDocument77 pagesA Companion To Fish's Psychopathologyolivukovic100% (1)
- Diagnosis, Treatment, and Prevention of Adenovirus Infection - UpToDateDocument28 pagesDiagnosis, Treatment, and Prevention of Adenovirus Infection - UpToDateMisael TaverasNo ratings yet
- Alagille Syndrome: A GuideDocument16 pagesAlagille Syndrome: A GuideKarla Edith Rodriguez NavaNo ratings yet
- Diagnosis and Treatment of Pericarditis: Massimo Imazio, Fiorenzo GaitaDocument11 pagesDiagnosis and Treatment of Pericarditis: Massimo Imazio, Fiorenzo GaitaJaziel Lopez PerezNo ratings yet
- Evaluating Diagnostic Tests - UpToDate 2019 PDFDocument17 pagesEvaluating Diagnostic Tests - UpToDate 2019 PDFNohelia Pino0% (1)